

PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs
PDF Version - Glidewell Dental Labs

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
■ THE DENTOGINGIVAL COMPLEX<br />
The dentogingival complex consists of a connective tissue<br />
attachment, an epithelial attachment (or junctional epithelium),<br />
and the gingival sulcus. As described by Spear 1 and<br />
Kois 2 , the most critical relationship for biologic health,<br />
when the clinician is placing a restoration at or below the<br />
free gingival margin (FGM), is the margin location relative<br />
to the crest of bone. Kois states that the distance from the<br />
FGM to the osseous crest on the facial aspect is 3.0 mm.<br />
Interproximally on anterior teeth, this distance is 4.0 mm<br />
due to the curvature of the cementoenamel junction. The<br />
height of the interdental papilla can also be predictably<br />
maintained at 4.0 mm incisal to the osseous crest between<br />
anterior teeth with normal root proximity, approximately<br />
2.0 to 3.0 mm at the osseous crest. With these parameters<br />
in mind, the clinician must first decide where the<br />
restorative margin will be placed. With all-ceramic restorations,<br />
if one does not have to block out undesirable<br />
dentin colors or core materials, then it may be desirable<br />
to place the restorative margin at the free gingival crest<br />
or even slightly supragingival. However, if an intracrevicular<br />
margin is required for aesthetic reasons, it should<br />
be placed no further than 0.5 mm into the gingival sulcus<br />
to avoid adverse biologic responses due to encroachment<br />
upon the attachment apparatus. Kois and Coslet, et al. 3<br />
also describe a variation in biologic width that compares<br />
the distance from the alveolar crest to the FGM and divide<br />
this into three categories: normal crest, high crest,<br />
and low crest. In simplified terms, normal-crest patients<br />
(about 70 percent) have approximately a 2.0 mm combined<br />
epithelial and connective tissue attachment and 1.0<br />
mm average sulcus depth. If the sulcus depth is greater<br />
than 1.0 mm, the free gingival excess can be safely resected<br />
and upon healing will result in a dentogingival<br />
complex measuring 3.0 mm on the facial aspect. Patients<br />
with a high crest often have a shallower sulcus depth<br />
and a combined epithelial and connective tissue attach-<br />
“If diastemata are present, the<br />
interproximal margin of the<br />
preparation should be carried<br />
lingually to the linguoproximal<br />
line angle and be placed slightly<br />
intracrevicularly in the proximal<br />
area to help ‘squeeze’<br />
the gingival papilla.”<br />
28 Maximize Your Aesthetic Results<br />
ment of less than 2.0 mm. These patients have relatively<br />
stable FGM positions and are not prone to recession upon<br />
manipulation of the tissues. Low-crest patients often have<br />
normal sulcus depth (1.0 mm to 3.0 mm) and a combined<br />
epithelial and connective tissue attachment that is less<br />
than 2.0 mm. These patients are highly prone to recession<br />
and must be treatment planned accordingly. The FGM of<br />
low-crest patients will tend to apically reposition and turn<br />
into a normal-crest situation after gingival retraction or<br />
surgery. Therefore, the most important factor in achieving<br />
post-restorative gingival health and stability is the position<br />
of the restorative margin relative to the bony crest,<br />
not the preoperative health and/or the position of the<br />
gingival tissues.<br />
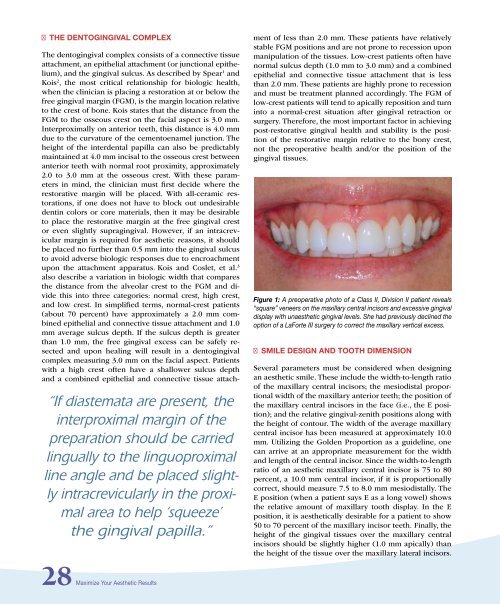
Figure 1: A preoperative photo of a Class II, Division II patient reveals<br />
“square” veneers on the maxillary central incisors and excessive gingival<br />
display with unaesthetic gingival levels. She had previously declined the<br />
option of a LaForte III surgery to correct the maxillary vertical excess.<br />
■ SMILE DESIGN AND TOOTH DIMENSION<br />
Several parameters must be considered when designing<br />
an aesthetic smile. These include the width-to-length ratio<br />
of the maxillary central incisors; the mesiodistal proportional<br />
width of the maxillary anterior teeth; the position of<br />
the maxillary central incisors in the face (i.e., the E position);<br />
and the relative gingival-zenith positions along with<br />
the height of contour. The width of the average maxillary<br />
central incisor has been measured at approximately 10.0<br />
mm. Utilizing the Golden Proportion as a guideline, one<br />
can arrive at an appropriate measurement for the width<br />
and length of the central incisor. Since the width-to-length<br />
ratio of an aesthetic maxillary central incisor is 75 to 80<br />
percent, a 10.0 mm central incisor, if it is proportionally<br />
correct, should measure 7.5 to 8.0 mm mesiodistally. The<br />
E position (when a patient says E as a long vowel) shows<br />
the relative amount of maxillary tooth display. In the E<br />
position, it is aesthetically desirable for a patient to show<br />
50 to 70 percent of the maxillary incisor teeth. Finally, the<br />
height of the gingival tissues over the maxillary central<br />
incisors should be slightly higher (1.0 mm apically) than<br />
the height of the tissue over the maxillary lateral incisors.













