Packet for patients five years of age and older - Atlantic Health System
Packet for patients five years of age and older - Atlantic Health System
Packet for patients five years of age and older - Atlantic Health System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
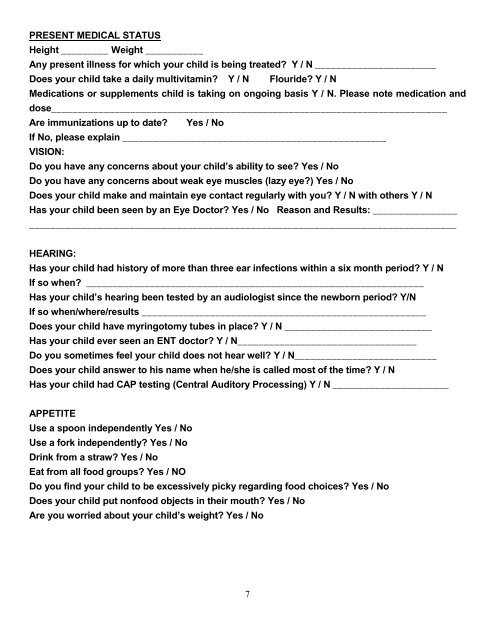
PRESENT MEDICAL STATUS<br />
Height _________ Weight ___________<br />
Any present illness <strong>for</strong> which your child is being treated? Y / N _______________________<br />
Does your child take a daily multivitamin? Y / N Flouride? Y / N<br />
Medications or supplements child is taking on ongoing basis Y / N. Please note medication <strong>and</strong><br />
dose___________________________________________________________________________<br />
Are immunizations up to date? Yes / No<br />
If No, please explain __________________________________________________<br />
VISION:<br />
Do you have any concerns about your child’s ability to see? Yes / No<br />
Do you have any concerns about weak eye muscles (lazy eye?) Yes / No<br />
Does your child make <strong>and</strong> maintain eye contact regularly with you? Y / N with others Y / N<br />
Has your child been seen by an Eye Doctor? Yes / No Reason <strong>and</strong> Results: ________________<br />
_________________________________________________________________________________<br />
HEARING:<br />
Has your child had history <strong>of</strong> more than three ear infections within a six month period? Y / N<br />
If so when? ________________________________________________________________<br />
Has your child’s hearing been tested by an audiologist since the newborn period? Y/N<br />
If so when/where/results ______________________________________________________<br />
Does your child have myringotomy tubes in place? Y / N ____________________________<br />
Has your child ever seen an ENT doctor? Y / N__________________________________<br />
Do you sometimes feel your child does not hear well? Y / N___________________________<br />
Does your child answer to his name when he/she is called most <strong>of</strong> the time? Y / N<br />
Has your child had CAP testing (Central Auditory Processing) Y / N ______________________<br />
APPETITE<br />
Use a spoon independently Yes / No<br />
Use a <strong>for</strong>k independently? Yes / No<br />
Drink from a straw? Yes / No<br />
Eat from all food groups? Yes / NO<br />
Do you find your child to be excessively picky regarding food choices? Yes / No<br />
Does your child put nonfood objects in their mouth? Yes / No<br />
Are you worried about your child’s weight? Yes / No<br />
7