Packet for patients five years of age and older - Atlantic Health System
Packet for patients five years of age and older - Atlantic Health System
Packet for patients five years of age and older - Atlantic Health System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
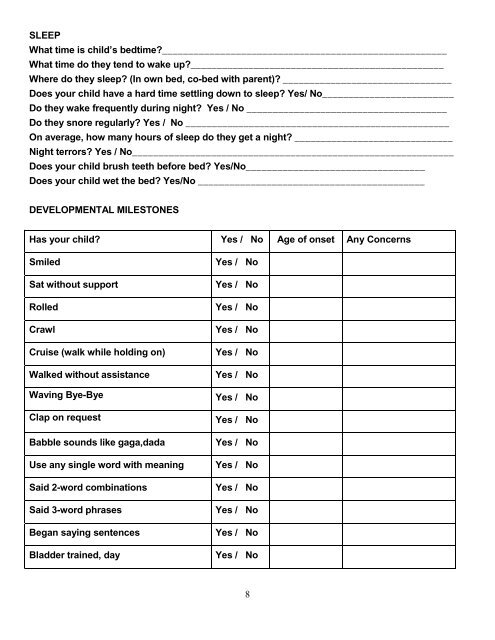
SLEEP<br />
What time is child’s bedtime?______________________________________________________<br />
What time do they tend to wake up?________________________________________________<br />
Where do they sleep? (In own bed, co-bed with parent)? ________________________________<br />
Does your child have a hard time settling down to sleep? Yes/ No_________________________<br />
Do they wake frequently during night? Yes / No ______________________________________<br />
Do they snore regularly? Yes / No __________________________________________________<br />
On aver<strong>age</strong>, how many hours <strong>of</strong> sleep do they get a night? ______________________________<br />
Night terrors? Yes / No_____________________________________________________________<br />
Does your child brush teeth be<strong>for</strong>e bed? Yes/No__________________________________<br />
Does your child wet the bed? Yes/No ___________________________________________<br />
DEVELOPMENTAL MILESTONES<br />
Has your child? Yes / No Age <strong>of</strong> onset Any Concerns<br />
Smiled<br />
Sat without support<br />
Rolled<br />
Crawl<br />
Cruise (walk while holding on)<br />
Walked without assistance<br />
Waving Bye-Bye<br />
Clap on request<br />
Babble sounds like gaga,dada<br />
Use any single word with meaning<br />
Said 2-word combinations<br />
Said 3-word phrases<br />
Began saying sentences<br />
Bladder trained, day<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
Yes / No<br />
8