Packet for patients five years of age and older - Atlantic Health System
Packet for patients five years of age and older - Atlantic Health System
Packet for patients five years of age and older - Atlantic Health System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
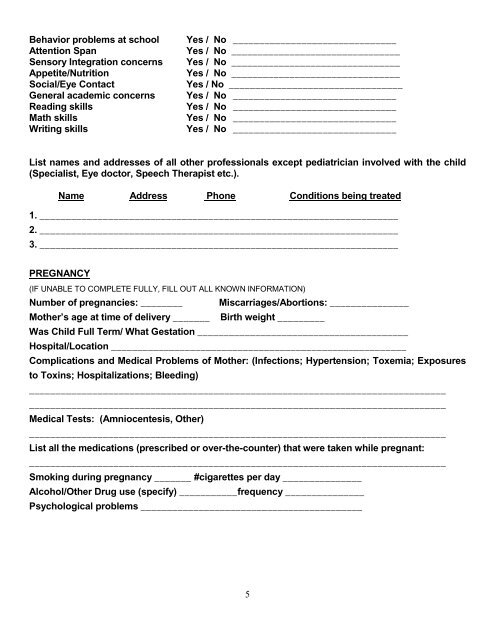
Behavior problems at school<br />
Attention Span<br />
Sensory Integration concerns<br />
Appetite/Nutrition<br />
Social/Eye Contact<br />
General academic concerns<br />
Reading skills<br />
Math skills<br />
Writing skills<br />
Yes / No _______________________________<br />
Yes / No ________________________________<br />
Yes / No ________________________________<br />
Yes / No ________________________________<br />
Yes / No _________________________________<br />
Yes / No _______________________________<br />
Yes / No _______________________________<br />
Yes / No _______________________________<br />
Yes / No _______________________________<br />
List names <strong>and</strong> addresses <strong>of</strong> all other pr<strong>of</strong>essionals except pediatrician involved with the child<br />
(Specialist, Eye doctor, Speech Therapist etc.).<br />
Name Address Phone Conditions being treated<br />
1. ____________________________________________________________________<br />
2. ____________________________________________________________________<br />
3. ____________________________________________________________________<br />
PREGNANCY<br />
(IF UNABLE TO COMPLETE FULLY, FILL OUT ALL KNOWN INFORMATION)<br />
Number <strong>of</strong> pregnancies: ________ Miscarri<strong>age</strong>s/Abortions: _______________<br />
Mother’s <strong>age</strong> at time <strong>of</strong> delivery _______ Birth weight _________<br />
Was Child Full Term/ What Gestation ________________________________________<br />
Hospital/Location ________________________________________________________<br />
Complications <strong>and</strong> Medical Problems <strong>of</strong> Mother: (Infections; Hypertension; Toxemia; Exposures<br />
to Toxins; Hospitalizations; Bleeding)<br />
_______________________________________________________________________________<br />
_______________________________________________________________________________<br />
Medical Tests: (Amniocentesis, Other)<br />
_______________________________________________________________________________<br />
List all the medications (prescribed or over-the-counter) that were taken while pregnant:<br />
_______________________________________________________________________________<br />
Smoking during pregnancy _______ #cigarettes per day _______________<br />
Alcohol/Other Drug use (specify) ___________frequency _______________<br />
Psychological problems __________________________________________<br />
5