Health & Lifestyle Questionnaire Goal Profile Lifestyle Profile
Health & Lifestyle Questionnaire Goal Profile Lifestyle Profile
Health & Lifestyle Questionnaire Goal Profile Lifestyle Profile

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
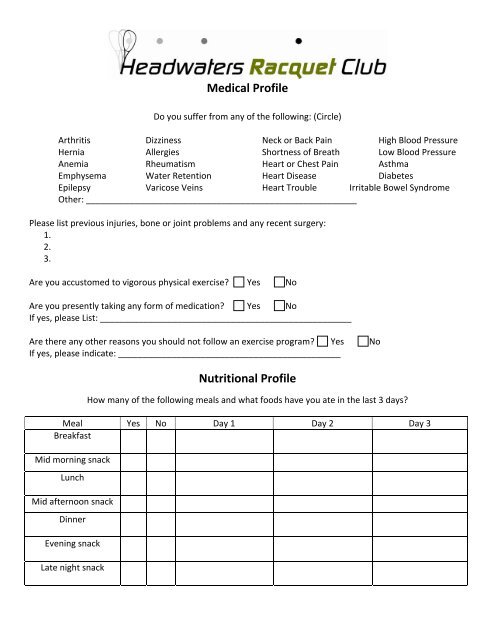
Medical <strong>Profile</strong><br />
Do you suffer from any of the following: (Circle)<br />
Arthritis Dizziness Neck or Back Pain High Blood Pressure<br />
Hernia Allergies Shortness of Breath Low Blood Pressure<br />
Anemia Rheumatism Heart or Chest Pain Asthma<br />
Emphysema Water Retention Heart Disease Diabetes<br />
Epilepsy Varicose Veins Heart Trouble Irritable Bowel Syndrome<br />
Other: ________________________________________________________<br />
Please list previous injuries, bone or joint problems and any recent surgery:<br />
1.<br />
2.<br />
3.<br />
Are you accustomed to vigorous physical exercise? Yes No<br />
Are you presently taking any form of medication? Yes No<br />
If yes, please List: ____________________________________________________<br />
Are there any other reasons you should not follow an exercise program? Yes No<br />
If yes, please indicate: ______________________________________________<br />
Nutritional <strong>Profile</strong><br />
How many of the following meals and what foods have you ate in the last 3 days?<br />
Meal Yes No Day 1 Day 2 Day 3<br />
Breakfast<br />
Mid morning snack<br />
Lunch<br />
Mid afternoon snack<br />
Dinner<br />
Evening snack<br />
Late night snack