Licensed Clinical Social Worker by Completing Provisional
Licensed Clinical Social Worker by Completing Provisional
Licensed Clinical Social Worker by Completing Provisional

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
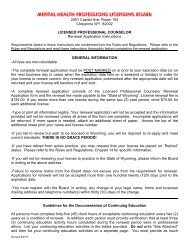
APPLICATION INSTRUCTIONS<br />
<strong>Licensed</strong> <strong>Clinical</strong> <strong>Social</strong> <strong>Worker</strong> <strong>by</strong> <strong>Completing</strong> <strong>Provisional</strong> (LCSW)<br />
Be aware that you must continue to work under administrative supervision and clinical supervision <strong>by</strong> your Designated<br />
<strong>Clinical</strong> Supervisor until the license for independent clinical practice is issued <strong>by</strong> the Board.<br />
Specific requirements are detailed in the Rules and Regulations. Please review the requirements prior to submitting an<br />
application.<br />
GENERAL INFORMATION<br />
• Application files will be presented to the Application Review Committee (Committee) for consideration when all<br />
required documentation has been received.<br />
• The Committee will not review your qualifications without receipt of a formal application and fee.<br />
• The application fee for licensure <strong>by</strong> completing the provisional is $200.00. Make checks payable to the “State of<br />
Wyoming”. Do not send cash. All fees are non-refundable regardless of the outcome.<br />
• All documents offered in support of the application must be submitted directly to the Committee from the source, not<br />
forwarded through you.<br />
Required Documents:<br />
• Complete application<br />
• Appropriate application fee<br />
• The provisional license identification card<br />
• A revised disclosure statement<br />
Additional Documents:<br />
• Verification and Evaluation of Supervised Experience<br />
• Official Exam Score Report<br />
DOCUMENTS<br />
INSTRUCTIONS<br />
Application<br />
• The check boxes for Discipline and Method are completed for you.<br />
• Type or print all information clearly.<br />
• Items #1-4 need no specific instruction.<br />
• Items #5 and 6 Current Employer- It is very important that you provide your current employer, and not your<br />
prospective employer. If you are currently unemployed, please leave this area blank.<br />
• Item #7 Preferred Mailing Address- If you do not indicate a preference our records will default to your home<br />
address.<br />
• Item #8 E-mail Address- Provide an e-mail address that you check regularly. We will notify you via e-mail when<br />
your application form is received. If there are any issues or questions concerning your application, these will be<br />
communicated to you through e-mail.<br />
Revised 8/2013 Page 1 of 2
• Item #9 Work History- List all employment since the issuance of your provisional license. Start with your most<br />
recent employment/experience and work backward in time. Account for all gaps in time such as periods of<br />
unemployment.<br />
• Items #10-19- Provide a written explanation for each of your “Yes” answers. Make sure that your name appears on<br />
additional documents. Include documentation such as certified copies of court records, state disciplinary action<br />
documents, letters of sanction from professional associations, etc.<br />
• Read the Warning, Agreement and Affidavit. Remember, you are stating that you have read, and agree to abide<br />
<strong>by</strong>, the rules and regulations. The rules are available on the Board’s web page at<br />
http://plboards.state.wy.us/mentalhealth. Read them. Sign and date the application. Please sign in blue ink. Mail<br />
the original application, appropriate fee and proof of legal presence to the Board.<br />
<strong>Provisional</strong> License Identification Card<br />
• Include the pocket sized provisional license identification card with your application.<br />
• If you are unable to return the card, attach a brief explanation of the reason.<br />
Revised Disclosure Statement<br />
• Include a copy of the revised Professional Disclosure Statement that you will use once you are granted a license <strong>by</strong><br />
the Board.<br />
• The particular criteria for the disclosure statement can be found in the Rules and Regulations, Chapter 15 Section<br />
1(xxvii), although you should have been providing a disclosure statement to your clients since the issue date of your<br />
provisional license.<br />
Verification and Evaluation of Supervised Experience<br />
• This form must be submitted <strong>by</strong> every Designated <strong>Clinical</strong> Supervisor you have had since the provisional license<br />
was granted, regardless of the length of time you were under their supervision.<br />
• This form must be send directly to the Board from the Supervisor. The Board will not accept this information from<br />
you or through your hands in any way.<br />
• This information is be kept confidential <strong>by</strong> the Board, although you may be informed of the number of hours<br />
reported.<br />
• Only clinical experience that was completed under the supervision of an approved designated clinical supervisor<br />
may be applied towards the experience and supervision requirements for licensure.<br />
Official Exam Score Report<br />
• The Board will accept the Association of <strong>Social</strong> Work Boards (ASWB) examination at the Advanced Generalist or<br />
<strong>Clinical</strong> Level.<br />
• Contact ASWB and request that an official examination score report be send directly to the Board. The Board will<br />
not accept this information from you or through your hands in any way.<br />
PROCEDURE<br />
You will receive an e-mail acknowledging that your application form and fee have been received. You may inquire about<br />
your application status <strong>by</strong> e-mailing to WyoMHPLB@wyo.gov. Please limit your inquiries to no more than twice per week.<br />
When all required supportive documents have been received, the Application Review Committee will evaluate your<br />
application. You will be notified of the outcome.<br />
Inquiries regarding these application procedures and application status may be directed to WyoMHPLB@wyo.gov.<br />
Mental Health Professions Licensing Board<br />
2001 Capitol Ave, Room 104<br />
Cheyenne, WY 82002<br />
Web Site: http://plboards.state.wy.us/mentalhealth<br />
Revised 8/2013 Page 2 of 2
MENTAL HEALTH PROFESSIONS LICENSING BOARD<br />
2001 Capitol Ave, Room 104<br />
Cheyenne WY 82002<br />
http://plboards.state.wy.us/mentalhealth<br />
WyoMHPLB@wyo.gov<br />
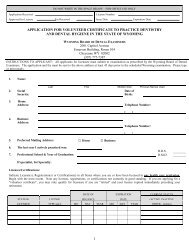
APPLICATION<br />
Specific requirements are detailed in the Rules and Regulations which are available on our web page. Review the requirements prior to submitting your application.<br />
Please type or print legibly, preferably in blue ink. The Board will only accept originally signed applications. Before mailing be sure to include payment of the<br />
application fee. Make checks payable to the “State of Wyoming”. Do not send cash. All fees are non-refundable regardless of the outcome.<br />
Incomplete applications WILL NOT be reviewed.<br />
Select from these check boxes if you are applying for certification at the bachelor’s degree level or equivalent, or with specialty training for the CAPA.<br />
ADDICTIONS PRACTITIONER<br />
ADDICTIONS PRACTITIONER ASSISTANT<br />
DISCIPLINE:<br />
(One only)<br />
SOCIAL WORKER<br />
METHOD:<br />
(One only)<br />
EXAMINATION<br />
RECIPROCAL<br />
Select from these check boxes if you are applying for licensure at the master’s degree level.<br />
ADDICTIONS THERAPIST<br />
PROVISIONAL<br />
DISCIPLINE: CLINICAL SOCIAL WORKER<br />
METHOD: COMPLETING PROVISIONAL<br />
(One only) MARRIAGE AND FAMILY THERAPIST (One only) EXAMINATION<br />
PROFESSIONAL COUNSELOR<br />
RECIPROCAL<br />
$300.00 fee<br />
$300.00 fee<br />
$150.00 fee<br />
$200.00 fee<br />
$350.00 fee<br />
$350.00 fee<br />
1. NAME:<br />
2.<br />
3.<br />
SOCIAL<br />
SECURITY:<br />
LEGAL<br />
PRESENCE: U.S. OTHER<br />
Last First Middle Initial Previous Names Used<br />
DATE OF<br />
BIRTH:<br />
(U.S. Code Title 8, Chapter 14, Section 1621 requires proof of legal presence in the United States. Attach<br />
acceptable documentation from enclosed List A and B.)<br />
TELEPHONE NUMBER(S):<br />
4.<br />
HOME<br />
ADDRESS:<br />
Street Address<br />
( )<br />
Home<br />
5.<br />
CURRENT<br />
EMPLOYER:<br />
( )<br />
City State Zip Cell<br />
Business Name<br />
TELEPHONE NUMBER(S):<br />
6.<br />
BUSINESS<br />
ADDRESS:<br />
Street Address<br />
( )<br />
Phone<br />
( )<br />
City State Zip Fax<br />
7. PREFERRED MAILING ADDRESS: HOME BUSINESS<br />
8. E-MAIL ADDRESS:<br />
Please provide an e-mail address that you check regularly. If there are any questions or issues regarding your<br />
application, the Board staff will communicate with you at this address.<br />
Revised 8/2013 Page 1 of 3
9. EXPERIENCE: List all employment since the issuance of your provisional license. Begin with today and work back in time. Note<br />
any interruptions in time, such as periods of unemployment. Refer to the application instructions for additional direction.<br />
From: To: Supervisor:<br />
Month/Year<br />
Month/Year<br />
Organization:<br />
Address:<br />
Brief Description of Work:<br />
From: To: Supervisor:<br />
Month/Year<br />
Month/Year<br />
Organization:<br />
Address:<br />
Brief Description of Work:<br />
From: To: Supervisor:<br />
Month/Year<br />
Month/Year<br />
Organization:<br />
Address:<br />
Brief Description of Work:<br />
From: To: Supervisor:<br />
Month/Year<br />
Month/Year<br />
Organization:<br />
Address:<br />
Brief Description of Work:<br />
Revised 8/2013 Page 2 of 3
HISTORY<br />
10. Have you ever, or are you now, providing any of the services regulated <strong>by</strong> W.S. 33-38-101 et seq. in the<br />
State of Wyoming, without meeting the requirement for licensure or certification, or without meeting an<br />
exemption provided in W.S. 33-38-103?<br />
Yes<br />
No<br />
11. Has any state rejected or denied your application for certification or licensure in any profession? Yes No<br />
12. Has any state revoked, suspended, refused to renew, or otherwise restricted your certificate or license in<br />
any profession?<br />
13. Have you ever voluntarily surrendered your certificate or license in any profession in order to avoid<br />
disciplinary action <strong>by</strong> a regulatory agency in any state?<br />
Yes<br />
Yes<br />
No<br />
No<br />
14. Have you ever been sanctioned <strong>by</strong> a professional association? Yes No<br />
15. Have you been convicted of a misdemeanor involving moral turpitude, including pleas of nolo contendere<br />
or no contest?<br />
Yes<br />
No<br />
16. Have you been convicted of a felony in any profession, including pleas of nolo contendere or no contest? Yes No<br />
17. Are you addicted to, or do you habitually use alcohol, any controlled substance, or other drugs having<br />
similar effects?<br />
Yes<br />
No<br />
18. Have you ever been judged incompetent <strong>by</strong> a court of law? Yes No<br />
19. Have you ever violated and been convicted of a charge under the Wyoming Controlled Substances Act? Yes No<br />
Attach a written explanation if you answered "YES" to any of questions 10 through 19 above. Include documentation related to your<br />
“YES” answer(s), including, but not limited to, certified copies of court records, letters of sanction, state board disciplinary action<br />
documents, etc.<br />
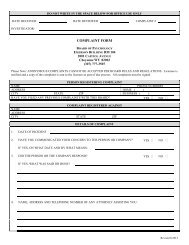
WARNING<br />
Making a false statement or giving a false answer to any question on this form is a felony punishable <strong>by</strong> imprisonment for not more than<br />
two (2) years, a fine of not more than two thousand dollars ($2,000.00), or both. (W.S. § 6-5-303.)<br />
AGREEMENT<br />
In signing this application, I do here<strong>by</strong> state that I have read, understand, and agree to abide <strong>by</strong> the rules and regulations promulgated<br />
<strong>by</strong> the Mental Health Professions Licensing Board, and W.S. § 33-38-101 through 113. I also agree to adhere to the codes of ethics<br />
applicable to my profession and this application.<br />
AFFIDAVIT<br />
The undersigned, being duly sworn, deposes and says that he or she is the person making the foregoing statements and that they are<br />
made in good faith and are true in every respect.<br />
SIGNATURE OF APPLICANT<br />
DATE<br />
Revised 8/2013 Page 3 of 3
MENTAL HEALTH PROFESSIONS LICENSING BOARD<br />
2001 Capitol Ave, Room 104<br />
Cheyenne WY 82002<br />
http://plboards.state.wy.us/mentalhealth<br />
WyoMHPLB@wyo.gov<br />
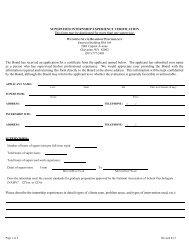
VERIFICATION AND EVALUATION OF SUPERVISED EXPERIENCE<br />
SUPERVISOR<br />
IT IS VERY IMPORTANT THAT YOU READ AND COMPLY WITH THESE DIRECTIONS.<br />
Your name has been submitted <strong>by</strong> the applicant as someone who has supervised their professional clinical experience. The Board, as well as<br />
the applicant, would appreciate your providing the information requested and returning this form directly to the Board at the above address.<br />
Please do not give the completed form to the applicant to be submitted to the Board. Please do not ask the applicant to complete any<br />
information on this form. The Board will not accept this information from the applicant or through the applicant’s hands in any way. This<br />
information will be kept confidential <strong>by</strong> the Board, although the applicant may be informed of the number of hours reported. The information<br />
provided will not be reviewed unless all areas of this form are completed. Incomplete forms will not be accepted and will be returned to the<br />
supervisor. Failure to return this form will affect the applicant’s ability to become independently licensed.<br />
APPLICANT’S<br />
NAME:<br />
Last First Middle Initial<br />
EXPERIENCE<br />
WAS EARNED<br />
AT:<br />
SUPERVISOR’S<br />
NAME:<br />
Business Name<br />
Street Address<br />
TELEPHONE NUMBER(S):<br />
( )<br />
Phone<br />
( )<br />
City State Zip Fax<br />
Last First Middle Initial<br />
TELEPHONE NUMBER(S):<br />
SUPERVISOR’S<br />
CURRENT<br />
ADDRESS:<br />
Street Address<br />
( )<br />
Home<br />
E-MAIL<br />
ADDRESS:<br />
( )<br />
City State Zip Cell<br />
Please provide an e-mail address that you check regularly. If there are any questions or issues regarding your responses, we will<br />
communicate with you at this address.<br />
REGISTRATION: List each license YOU held during the time you supervised this applicant. In order to be considered a qualified clinical<br />
supervisor, you must have been licensed for at least (2) years with at least four (4) years of experience PRIOR to supervising the applicant. Report<br />
the date that your license was originally issued, and not the date that it was last renewed.<br />
LICENSE TITLE<br />
LICENSE<br />
NUMBER<br />
STATE<br />
ORIGINAL<br />
ISSUE DATE<br />
EXPIRATION<br />
DATE<br />
Revised 8/2013 Page 1 of 3
CLINICAL EXPERIENCE<br />
Report the amount of clinical experience gained <strong>by</strong> the applicant. This includes all hours worked. Direct client contact hours must also be<br />
reported. Deduct for holidays, vacation, and other time off.<br />
FOR EXPERIENCE COMPLETED IN WYOMING- The “From” date cannot be prior to the date the <strong>Provisional</strong> Supervision Agreement<br />
was approved <strong>by</strong> the Board.<br />
FOR EXPERIENCE COMPLETED OUT-OF-STATE- The “From” date cannot be less than two (2) years after the issue date of the<br />
supervisor’s clinical license at the independent practice level.<br />
From: To: at an average of hours per week for a total of hours,<br />
MM/YYYY<br />
MM/YYYY<br />
which included<br />
hours of direct client contact.<br />
For example:<br />
From: 1/2000 To: 12/2000 at an average of 40 hours per week for a total of 1840 hours,<br />
MM/YYYY MM/YYYY (Time deducted for vacations and holidays.)<br />
which included 650 hours of direct client contact.<br />
DESCRIBE THE PROFESSIONAL DUTIES which the applicant performed under your supervision: (For Addictions Therapy and<br />
Marriage and Family Therapy applicants, indicate the percentage of time spent with addiction clients or couples and families.)<br />
CLINICAL SUPERVISION<br />
Report the amount of face-to-face supervision that you provide to the applicant. Group supervision MAY NOT be included in the report.<br />
TRIADIC supervision is an arrangement where the designated qualified clinical supervisor conducts clinical supervision with two (2) supervisees<br />
simultaneously.<br />
During the time frame noted above:<br />
Individual face-to-face supervision was provided at an average of hours per week for a total of hours.<br />
Triadic face-to-face supervision was provided at an average of hours per week for a total of hours.<br />
For example:<br />
TOTAL FACE-TO-FACE CLINICAL SUPERVISION:<br />
Individual face-to-face supervision was provided at an average of .5 hours per week for a total of 25 hours.<br />
Triadic face-to-face supervision was provided at an average of 1 hours per week for a total of 50 hours.<br />
TOTAL FACE-TO-FACE CLINICAL SUPERVISION: 75<br />
DESCRIBE THE CLINICAL SUPERVISION PROCESS:<br />
Revised 8/2013 Page 2 of 3
EVALUATE THE APPLICANT ON THE FOLLOWING:<br />
UNABLE<br />
TO<br />
EVALUATE<br />
POOR<br />
AVERAGE<br />
ABOVE<br />
AVERAGE SUPERIOR<br />
Skill Level<br />
Ability to establish and maintain good professional relations.<br />
Possession of emotional maturity & stability required for satisfactory work with clients and<br />
patients.<br />
Understanding of and adherence to approved standards of professional and ethical conduct.<br />
Personal character: honesty, integrity and general conduct.<br />
Reputation among colleagues as a professional.<br />
Capacity for professional growth and development.<br />
I would rate the applicant's overall performance under my supervision as:<br />
I would rate the applicant's competence to engage in independent clinical practice as:<br />
PROVIDE ANY ADDITIONAL INFORMATION REGARDING THE APPLICANT WHICH YOU MAY CONSIDER<br />
RELEVANT:<br />
I recommend that the applicant be considered for licensing without reservation.<br />
I recommend that the applicant be considered for licensing with reservation as outlined above.<br />
I do not recommend that the applicant be considered for licensing as outlined above.<br />
I here<strong>by</strong> certify that the information provided in this document is fair and accurate in every respect.<br />
SIGNATURE<br />
DATE<br />
The signed Verification and Evaluation of Supervised Experience may be e-mailed to WyoMHPLB@wyo.gov,<br />
or faxed to (307) 777-3508,<br />
or mailed to the address provided on this form.<br />
Revised 8/2013 Page 3 of 3