SKILLED CARE DURING CHILDBIRTH - Family Care International
SKILLED CARE DURING CHILDBIRTH - Family Care International
SKILLED CARE DURING CHILDBIRTH - Family Care International

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Skilled <strong>Care</strong> During Childbirth: Country Profiles Sri Lanka<br />
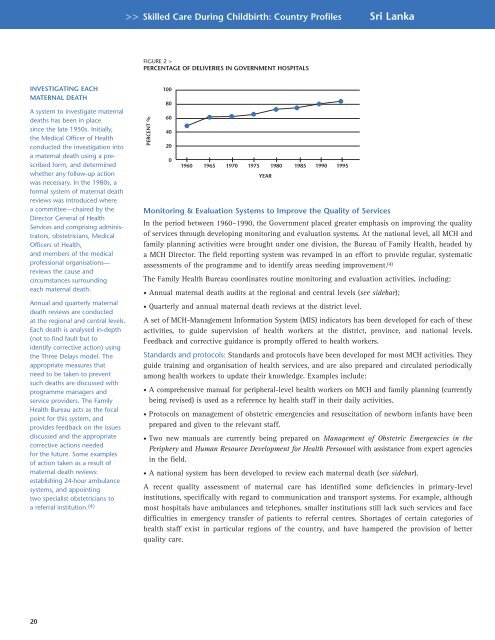
FIGURE 2 ><br />
PERCENTAGE OF DELIVERIES IN GOVERNMENT HOSPITALS<br />
INVESTIGATING EACH<br />
MATERNAL DEATH<br />
A system to investigate maternal<br />
deaths has been in place<br />
since the late 1950s. Initially,<br />
the Medical Officer of Health<br />
conducted the investigation into<br />
a maternal death using a prescribed<br />
form, and determined<br />
whether any follow-up action<br />
was necessary. In the 1980s, a<br />
formal system of maternal death<br />
reviews was introduced where<br />
a committee—chaired by the<br />
Director General of Health<br />
Services and comprising administrators,<br />
obstetricians, Medical<br />
Officers of Health,<br />
and members of the medical<br />
professional organisations—<br />
reviews the cause and<br />
circumstances surrounding<br />
each maternal death.<br />
Annual and quarterly maternal<br />
death reviews are conducted<br />
at the regional and central levels.<br />
Each death is analysed in-depth<br />
(not to find fault but to<br />
identify corrective action) using<br />
the Three Delays model. The<br />
appropriate measures that<br />
need to be taken to prevent<br />
such deaths are discussed with<br />
programme managers and<br />
service providers. The <strong>Family</strong><br />
Health Bureau acts as the focal<br />
point for this system, and<br />
provides feedback on the issues<br />
discussed and the appropriate<br />
corrective actions needed<br />
for the future. Some examples<br />
of action taken as a result of<br />
maternal death reviews:<br />
establishing 24-hour ambulance<br />
systems, and appointing<br />
two specialist obstetricians to<br />
a referral institution. (4)<br />
PERCENT %<br />
100<br />
80<br />
60<br />
40<br />
20<br />
0<br />
1960 1965 1970 1975 1980 1985 1990 1995<br />
YEAR<br />
Monitoring & Evaluation Systems to Improve the Quality of Services<br />
In the period between 1960–1990, the Government placed greater emphasis on improving the quality<br />
of services through developing monitoring and evaluation systems. At the national level, all MCH and<br />
family planning activities were brought under one division, the Bureau of <strong>Family</strong> Health, headed by<br />
a MCH Director. The field reporting system was revamped in an effort to provide regular, systematic<br />
assessments of the programme and to identify areas needing improvement. (4)<br />
The <strong>Family</strong> Health Bureau coordinates routine monitoring and evaluation activities, including:<br />
• Annual maternal death audits at the regional and central levels (see sidebar);<br />
• Quarterly and annual maternal death reviews at the district level.<br />
A set of MCH-Management Information System (MIS) indicators has been developed for each of these<br />
activities, to guide supervision of health workers at the district, province, and national levels.<br />
Feedback and corrective guidance is promptly offered to health workers.<br />
Standards and protocols: Standards and protocols have been developed for most MCH activities. They<br />
guide training and organisation of health services, and are also prepared and circulated periodically<br />
among health workers to update their knowledge. Examples include:<br />
• A comprehensive manual for peripheral-level health workers on MCH and family planning (currently<br />
being revised) is used as a reference by health staff in their daily activities.<br />
• Protocols on management of obstetric emergencies and resuscitation of newborn infants have been<br />
prepared and given to the relevant staff.<br />
• Two new manuals are currently being prepared on Management of Obstetric Emergencies in the<br />
Periphery and Human Resource Development for Health Personnel with assistance from expert agencies<br />
in the field.<br />
• A national system has been developed to review each maternal death (see sidebar).<br />
A recent quality assessment of maternal care has identified some deficiencies in primary-level<br />
institutions, specifically with regard to communication and transport systems. For example, although<br />
most hospitals have ambulances and telephones, smaller institutions still lack such services and face<br />
difficulties in emergency transfer of patients to referral centres. Shortages of certain categories of<br />
health staff exist in particular regions of the country, and have hampered the provision of better<br />
quality care.<br />
20