SKILLED CARE DURING CHILDBIRTH - Family Care International
SKILLED CARE DURING CHILDBIRTH - Family Care International
SKILLED CARE DURING CHILDBIRTH - Family Care International

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
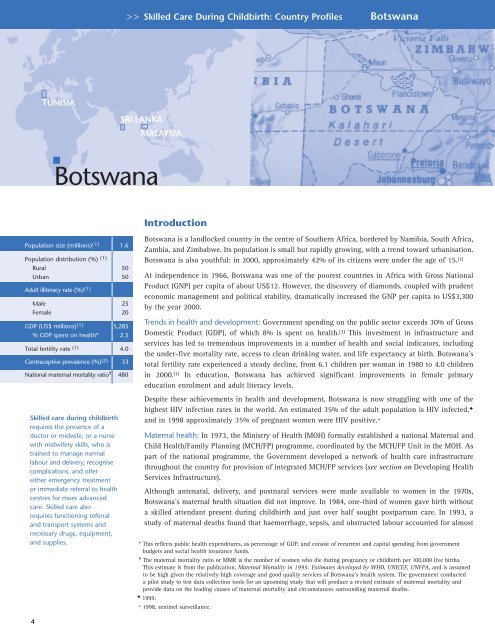
Skilled <strong>Care</strong> During Childbirth: Country Profiles Botswana<br />
TUNISIA<br />
SRI LANKA<br />
MALAYSIA<br />
Botswana<br />
Introduction<br />
Population size (millions) (1) 1.6<br />
Population distribution (%) (1)<br />
Rural 50<br />
Urban 50<br />
Adult illiteracy rate (%) (1)<br />
Male 25<br />
Female 20<br />
GDP (US$ millions) (1) 5,285<br />
% GDP spent on health* 2.5<br />
Total fertility rate (1) 4.0<br />
Contraceptive prevalence (%) (2) 33<br />
National maternal mortality ratio ✝ 480<br />
Skilled care during childbirth<br />
requires the presence of a<br />
doctor or midwife, or a nurse<br />
with midwifery skills, who is<br />
trained to manage normal<br />
labour and delivery, recognise<br />
complications, and offer<br />
either emergency treatment<br />
or immediate referral to health<br />
centres for more advanced<br />
care. Skilled care also<br />
requires functioning referral<br />
and transport systems and<br />
necessary drugs, equipment,<br />
and supplies.<br />
Botswana is a landlocked country in the centre of Southern Africa, bordered by Namibia, South Africa,<br />
Zambia, and Zimbabwe. Its population is small but rapidly growing, with a trend toward urbanisation.<br />
Botswana is also youthful: in 2000, approximately 42% of its citizens were under the age of 15. (1)<br />
At independence in 1966, Botswana was one of the poorest countries in Africa with Gross National<br />
Product (GNP) per capita of about US$12. However, the discovery of diamonds, coupled with prudent<br />
economic management and political stability, dramatically increased the GNP per capita to US$3,300<br />
by the year 2000.<br />
Trends in health and development: Government spending on the public sector exceeds 30% of Gross<br />
Domestic Product (GDP), of which 8% is spent on health. (3) This investment in infrastructure and<br />
services has led to tremendous improvements in a number of health and social indicators, including<br />
the under-five mortality rate, access to clean drinking water, and life expectancy at birth. Botswana’s<br />
total fertility rate experienced a steady decline, from 6.1 children per woman in 1980 to 4.0 children<br />
in 2000. (1) In education, Botswana has achieved significant improvements in female primary<br />
education enrolment and adult literacy levels.<br />
Despite these achievements in health and development, Botswana is now struggling with one of the<br />
highest HIV infection rates in the world. An estimated 35% of the adult population is HIV infected, ✦<br />
and in 1998 approximately 35% of pregnant women were HIV positive. +<br />
Maternal health: In 1973, the Ministry of Health (MOH) formally established a national Maternal and<br />
Child Health/<strong>Family</strong> Planning (MCH/FP) programme, coordinated by the MCH/FP Unit in the MOH. As<br />
part of the national programme, the Government developed a network of health care infrastructure<br />
throughout the country for provision of integrated MCH/FP services (see section on Developing Health<br />
Services Infrastructure).<br />
Although antenatal, delivery, and postnatal services were made available to women in the 1970s,<br />
Botswana’s maternal health situation did not improve. In 1984, one-third of women gave birth without<br />
a skilled attendant present during childbirth and just over half sought postpartum care. In 1993, a<br />
study of maternal deaths found that haemorrhage, sepsis, and obstructed labour accounted for almost<br />
* This reflects public health expenditures, as percentage of GDP, and consist of recurrent and capital spending from government<br />
budgets and social health insurance funds.<br />
✝ The maternal mortality ratio or MMR is the number of women who die during pregnancy or childbirth per 100,000 live births.<br />
This estimate is from the publication, Maternal Mortality in 1995: Estimates developed by WHO, UNICEF, UNFPA, and is assumed<br />
to be high given the relatively high coverage and good quality services of Botswana’s health system. The government conducted<br />
a pilot study to test data collection tools for an upcoming study that will produce a revised estimate of maternal mortality and<br />
provide data on the leading causes of maternal mortality and circumstances surrounding maternal deaths.<br />
✦ 1999.<br />
+ 1998, sentinel surveillance.<br />
4