

Pyrexia - PACT - ESICM
Pyrexia - PACT - ESICM
Pyrexia - PACT - ESICM

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Task 2. Determining the cause of fever in the critically ill patient<br />
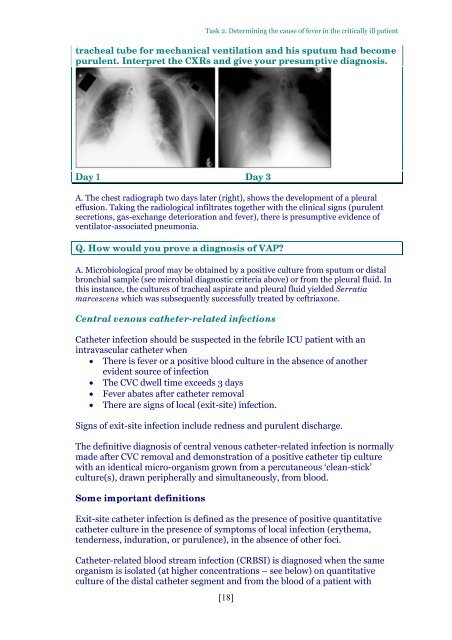
tracheal tube for mechanical ventilation and his sputum had become<br />
purulent. Interpret the CXRs and give your presumptive diagnosis.<br />
Day 1 Day 3<br />
A. The chest radiograph two days later (right), shows the development of a pleural<br />
effusion. Taking the radiological infiltrates together with the clinical signs (purulent<br />
secretions, gas-exchange deterioration and fever), there is presumptive evidence of<br />
ventilator-associated pneumonia.<br />
Q. How would you prove a diagnosis of VAP<br />
A. Microbiological proof may be obtained by a positive culture from sputum or distal<br />
bronchial sample (see microbial diagnostic criteria above) or from the pleural fluid. In<br />
this instance, the cultures of tracheal aspirate and pleural fluid yielded Serratia<br />
marcescens which was subsequently successfully treated by ceftriaxone.<br />
Central venous catheter-related infections<br />
Catheter infection should be suspected in the febrile ICU patient with an<br />
intravascular catheter when<br />
There is fever or a positive blood culture in the absence of another<br />
evident source of infection<br />
The CVC dwell time exceeds 3 days<br />
Fever abates after catheter removal<br />
There are signs of local (exit-site) infection.<br />
Signs of exit-site infection include redness and purulent discharge.<br />
The definitive diagnosis of central venous catheter-related infection is normally<br />
made after CVC removal and demonstration of a positive catheter tip culture<br />
with an identical micro-organism grown from a percutaneous ‘clean-stick’<br />
culture(s), drawn peripherally and simultaneously, from blood.<br />
Some important definitions<br />
Exit-site catheter infection is defined as the presence of positive quantitative<br />
catheter culture in the presence of symptoms of local infection (erythema,<br />
tenderness, induration, or purulence), in the absence of other foci.<br />
Catheter-related blood stream infection (CRBSI) is diagnosed when the same<br />
organism is isolated (at higher concentrations – see below) on quantitative<br />
culture of the distal catheter segment and from the blood of a patient with<br />
[18]














