Understanding & Discussing Women's Sexual Functioning: How to ...
Understanding & Discussing Women's Sexual Functioning: How to ...
Understanding & Discussing Women's Sexual Functioning: How to ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Understanding</strong> & <strong>Discussing</strong><br />
Women’s s <strong>Sexual</strong> <strong>Functioning</strong>:<br />
<strong>How</strong> <strong>to</strong> talk with your patients<br />
Karin E. Larsen, Ph.D.<br />
Assistant Professor<br />
Obstetrics Gynecology and<br />
Women’s s Health<br />
University of MN<br />
klarsen@umphysicians.umn.edu<br />
<strong>Sexual</strong> Dysfunctions/Disorders<br />
Desire<br />
Disorders<br />
Hypoactive<br />
<strong>Sexual</strong> Desire<br />
Disorder (302.71)<br />
<strong>Sexual</strong><br />
Aversion<br />
Disorder (302.79)<br />
Arousal<br />
Disorders<br />
Orgasm<br />
Disorders<br />
Female <strong>Sexual</strong><br />
Female<br />
Arousal Disorder<br />
Orgasmic<br />
(302.72)<br />
Disorder (302.73,<br />
formerly<br />
Male<br />
Inhibited Female<br />
Erectile Disorder<br />
Orgasm)<br />
(302.72, formerly<br />
Impotence)<br />
Male<br />
Orgasmic<br />
Disorder<br />
(302.74, formerly<br />
Inhibited Male<br />
Orgasm)<br />
Premature<br />
Ejaculation<br />
(302.75)<br />
Pain<br />
Disorders<br />
Dyspareunia<br />
(302.76)<br />
Vaginismus<br />
(306.51)<br />
Overview<br />
<strong>Sexual</strong> function and dysfunctions<br />
– DSM-IV Diagnostic Categories<br />
– Definition of sexual health<br />
Talking about sexual functioning<br />
– Difficulties talking w/patients about sexual functioning<br />
– Strategies for talking w/patients about sexual health<br />
Theory/model of human sexual fxn<br />
Theories/models of sexual functioning<br />
Establishing realistic ideas around “normal”<br />
sexual functioning<br />
Hypoactive <strong>Sexual</strong> Desire<br />
Disorder (HSDD) (302.71)<br />
A. Persistently or recurrently deficient (or absent) sexual<br />
fantasies and desire for sexual activity. The judgment of<br />
deficiency or absence is made by the clinician, taking<br />
in<strong>to</strong> account fac<strong>to</strong>rs that affect sexual functioning, such<br />
as age and the context of the person’s s life<br />
B. The disturbance causes marked distress or<br />
interpersonal difficulty<br />
C. The sexual dysfunction is not better accounted for by<br />
another Axis I disorder (except another <strong>Sexual</strong><br />
Dysfunction) and is not due exclusively <strong>to</strong> the direct<br />
physiological effects of a substance (e.g., a drug of<br />
abuse, a medication) or a general medical condition<br />
BR<br />
<strong>Sexual</strong> Aversion Disorder (302.79)<br />
A. Persistent or recurrent extreme<br />
aversion <strong>to</strong>, and avoidance of, all (or<br />
almost all) genital sexual contact with a<br />
sexual partner<br />
B. The disturbance causes marked<br />
distress or interpersonal difficulty<br />
C. The sexual dysfunction is not better<br />
accounted for by another Axis I disorder<br />
(except another <strong>Sexual</strong> Dysfunction)<br />
1
Female/Male <strong>Sexual</strong> Arousal<br />
Disorder (302.72)<br />
A. Persistent or recurrent inability <strong>to</strong> attain,<br />
or <strong>to</strong> maintain until completion of the<br />
sexual activity, an adequate lubrication-<br />
swelling response of sexual excitement<br />
B. The disturbance causes marked distress or<br />
interpersonal difficulty<br />
C. The orgasmic dysfunction is not better accounted for<br />
by another Axis I disorder (except another <strong>Sexual</strong><br />
Dysfunction) and is not due exclusively <strong>to</strong> the direct<br />
physiological effects of a substance (e.g., a drug of<br />
abuse, a medication) or a general medical condition<br />
Vaginismus (306.51)<br />
A. Recurrent or persistent involuntary<br />
spasm of the musculature of the outer<br />
third of the vagina that interferes with<br />
sexual intercourse<br />
B. The disturbance causes marked distress or<br />
interpersonal difficulty<br />
C. The disturbance is not better accounted for by<br />
another Axis I disorder (e.g., Somatization Disorder) and<br />
is not due exclusively <strong>to</strong> the direct physiological effects<br />
of a general medical condition<br />
Female Orgasmic Disorder (302.73)<br />
A. Persistent or recurrent delay in, or absence of,<br />
orgasm following a normal sexual excitement phase.<br />
Women exhibit wide variability in the type or intensity<br />
of stimulation that triggers orgasm. The diagnosis of<br />
Female Orgasmic Disorder should be based on the<br />
clinician’s s judgment that the woman’s s orgasmic<br />
capacity is less than would be reasonable for her age,<br />
sexual experience, and the adequacy of sexual<br />
stimulation she receives.<br />
B. The disturbance causes marked distress or interpersonal<br />
difficulty<br />
C. The orgasmic dysfunction is not better accounted for by<br />
another Axis I disorder (except another <strong>Sexual</strong> Dysfunction) and<br />
is not due exclusively <strong>to</strong> the direct physiological effects of a<br />
substance (e.g., a drug of abuse, a medication) or a general<br />
medical condition<br />
Fac<strong>to</strong>rs affecting sexual functioning<br />
Medical Conditions<br />
– Geni<strong>to</strong>urinary<br />
– Vascular<br />
– Neurological<br />
– Endocrine<br />
Medications<br />
– Psychotropic (e.g. SSRIs)<br />
– OCPs<br />
Psychosocial fac<strong>to</strong>rs<br />
– <strong>Sexual</strong> his<strong>to</strong>ry (eg(<br />
trauma)<br />
– Messages about sexuality<br />
– Dyadic stress<br />
– Body Image<br />
– Mental Health (eg(<br />
depression, anxiety, “stress”)<br />
Dyspareunia (302.76)<br />
A. Recurrent or persistent genital pain<br />
associated with sexual intercourse<br />
B. The disturbance causes marked distress or<br />
interpersonal difficulty<br />
C. The orgasmic dysfunction is not caused exclusively<br />
by Vaginismus or lack of lubrication, is not better<br />
accounted for by another Axis I disorder (except another<br />
<strong>Sexual</strong> Dysfunction) and is not due exclusively <strong>to</strong> the<br />
direct physiological effects of a substance (e.g., a drug of<br />
abuse, a medication) or a general medical condition<br />
Prevalence of Female <strong>Sexual</strong><br />
Dysfunctions<br />
For women (as opposed <strong>to</strong> men) Hypoactive <strong>Sexual</strong> Desire Disorder<br />
(HSDD) decreases with age<br />
Vaginismus<br />
– 1% prevalence<br />
Dyspareunia –<br />
– 18-72% (US)<br />
– Likelihood may increase post-menopause<br />
Orgasmic disorder<br />
– Kinsey (1953) 10% lifetime prevalence anorgasmia<br />
– Laumann et al (1999) 24% 1-yr 1<br />
prevalence of problems<br />
– Depending on definition: 4-24% 4<br />
– Lower SES and less education related <strong>to</strong> lower likelihood <strong>to</strong> experience<br />
orgasm. (Laumann(<br />
et al, 1994)<br />
<strong>Sexual</strong> Arousal disorder<br />
– Problems with lubrication:14-43% 43% US, (1-yr prevalence); 6% Iceland<br />
(lifetime prevalence); 8% Sweden (1-yr prevalence)…..<br />
– Increases with age for both men and women<br />
2
Defining <strong>Sexual</strong> Health<br />
The World Health Organization (WHO) definition of sexual health<br />
is "A state of physical, emotional, mental and social well-being<br />
related <strong>to</strong> sexuality; not merely the absence of disease, dysfunction<br />
or infirmity. <strong>Sexual</strong> health requires a positive and respectful<br />
approach <strong>to</strong> sexuality and sexual relationships, as well as the<br />
possibility of having pleasurable and safe sexual experiences, free f<br />
of coercion, discrimination and violence. For sexual health <strong>to</strong> be b<br />
attained and maintained, the sexual rights of all persons must be b<br />
protected, respected and fulfilled".<br />
“Thus the notion of sexual health implies a<br />
positive approach <strong>to</strong> human sexuality, and the<br />
purposes of sexual health care should be the<br />
enhancement of life and personal relationships,<br />
and not merely the counseling and care related<br />
<strong>to</strong> procreation or sexually transmitted diseases”<br />
Reasons physicians do not take<br />
a good sexual his<strong>to</strong>ry<br />
Discomfort or embarrassment of physician<br />
A belief that a sex his<strong>to</strong>ry is not relevant <strong>to</strong><br />
chief complaint<br />
Not adequately trained<br />
Merrill, JM, Lau, LF and Thornbby, , JI Why doc<strong>to</strong>rs have difficulty with sex<br />
his<strong>to</strong>ries. South Med J, 1990, 83, 613-618.<br />
618.<br />
Taking a<br />
<strong>Sexual</strong> His<strong>to</strong>ry<br />
Talking About<br />
Sex<br />
Kinsey’s s rule<br />
Never invite a negative answer or<br />
a closed ended answer<br />
e.g., NOT...<br />
– Have you ever<br />
Instead...<br />
– When was the last time<br />
– <strong>How</strong> many times<br />
– When did you begin<br />
Some his<strong>to</strong>ry on sex talk<br />
Surgeon Generals<br />
– Joycelyn Elders-1993<br />
apptd Surgeon General<br />
by Clin<strong>to</strong>n, ’94 spoke out on masturbation, ’94<br />
“fired” by Clin<strong>to</strong>n<br />
More Strategies<br />
Before “talking sex” with patients, work on<br />
– Developing sexual language<br />
– Not assuming that people know what sex<br />
words mean<br />
– David Satcher – 2001 -The Call <strong>to</strong> Action <strong>to</strong><br />
Promote <strong>Sexual</strong> Health and Responsible<br />
<strong>Sexual</strong> Behavior<br />
When “talking sex” with patients, work on<br />
– Teaching and role modeling: Use explicit &<br />
specific sexual terms and descriptions.<br />
3
“Assessment” Feedback<br />
Assessment<br />
Identify fac<strong>to</strong>rs that appear <strong>to</strong> be<br />
responsible for the development and<br />
maintenance of the problem<br />
– Medical conditions<br />
– Medications<br />
– Psychosocial fac<strong>to</strong>rs<br />
Interviewing Strategies<br />
Start with easy questions<br />
– Leave challenging (sexual) ones for later<br />
Some questions <strong>to</strong> start the discussion<br />
– What kinds of questions do you have about<br />
your sexuality or what concerns do you have<br />
about your sex life<br />
– What is your sex life like at this point Is that<br />
where you want it <strong>to</strong> be<br />
– <strong>How</strong> happy are you with your sex life Is your<br />
sexual activity pleasurable<br />
“Assessment” Feedback (cont<br />
(cont’d)<br />
Review problem and normalize it; providing<br />
some education<br />
It’s normal for someone <strong>to</strong><br />
– avoid doing something that is painful, anxiety-<br />
provoking, very difficult etc.<br />
– have difficulties with sexual functioning after a really<br />
stressful (traumatic) experience<br />
– have difficulty with sexual function when you are<br />
really down/depressed/sad/stressed out.<br />
– have difficulties with sexual functioning when you are<br />
having difficulties in your relationship<br />
Illness-related Questions<br />
What sexual changes, if any, have you noticed<br />
– Since your illness/injury<br />
– Since you began taking your medications<br />
What questions or concerns do you have about<br />
these changes<br />
Would you like <strong>to</strong> talk with anyone further about<br />
these changes<br />
Adapted from: Villeneuve & Ozolins, , AXON, 1990<br />
“Assessment” Feedback (cont<br />
Invite feedback<br />
Provide education: address any<br />
medical/sexual misinformation<br />
– Also consider “good enough sex” model<br />
(cont’d)<br />
Outline treatment components (e.g.<br />
medication changes, psychotherapy/sex<br />
therapy, sexual medicine, psychiatric, etc.)<br />
4
Theories and Models around<br />
<strong>Sexual</strong> <strong>Functioning</strong><br />
Improving <strong>Sexual</strong>ity –<br />
sex is not just intercourse<br />
Broaden definition of sex beyond genitals<br />
and goal-oriented oriented sexuality. What does<br />
sex mean <strong>to</strong> you<br />
“I’m m suggesting we call sex something else,<br />
and it should include everything from<br />
kissing <strong>to</strong> standing close <strong>to</strong>gether”<br />
-- Shere Hite<br />
BR<br />
Quality of Good-Enough Sex in Well-<br />
<strong>Functioning</strong>, Satisfied Couples<br />
McCarthy, J of Sex & Marital Therapy, , 1984, McCarthy Conference (2007) in<br />
Blooming<strong>to</strong>n, MN; McCarthy & Metz, 2008, p. 108<br />
35-45%<br />
20-25%<br />
25%<br />
15-20%<br />
Very satisfying. Both partners will be aroused &<br />
involved, experience is very good for both<br />
partners<br />
Good (at least 1 partner). Both partners will enjoy<br />
sex but one will be much more aroused and<br />
involved.<br />
Okay, not remarkable<br />
5-15%<br />
Unsatisfying, mediocre failures or “blah”<br />
**Normal duration of sexual intercourse is 7-10 minutes<br />
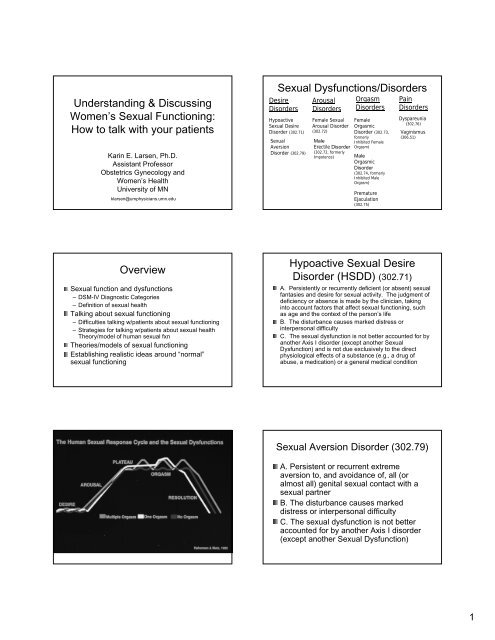
Women’s s <strong>Sexual</strong> Response<br />
Cycle<br />
(Basson,, 1999)<br />
Intimacy<br />
BR<br />
Sex contributes <strong>to</strong> relationship<br />
satisfaction<br />
Positive physical and<br />
emotional outcome<br />
<strong>Sexual</strong> desire<br />
Arousal<br />
Intimacy needs<br />
stimuli<br />
Sought stimuli<br />
processed<br />
<strong>Sexual</strong>ity adds 15-20% <strong>to</strong> couple satisfaction<br />
BUT<br />
a troubled sexual relationship plays a 50-75% role<br />
in marital dissatisfaction.<br />
---McCarthy, B, & McCarthy, E. (2003). Rekindling desire: A step-by-step<br />
program <strong>to</strong> help low sex and no-sex marriages.NY: Brunner-Routledge.<br />
5
General Guidelines for a Satisfying<br />
<strong>Sexual</strong> Relationship<br />
Realistic expectations: cannot re-live initial “passion, passion,” demand equal<br />
desire, mutual orgasm, etc.<br />
Personal responsibility/intimate team model<br />
– You are responsible for your own desire and orgasm. It is not<br />
your partner’s s responsibility <strong>to</strong> know what pleasures you, it is<br />
your responsibility <strong>to</strong> communicate and work <strong>to</strong>wards your own<br />
pleasure and listen <strong>to</strong> your partner’s s desires and respond <strong>to</strong><br />
them or propose alternatives.<br />
Giving and receiving pleasurable <strong>to</strong>uch is essential for sexual<br />
satisfaction<br />
Eroticism and arousal can lead <strong>to</strong> intercourse, but intercourse is not<br />
necessary for a satisfying sexual experience.<br />
Satisfying sexuality integrates, intimacy, non-demand pleasuring<br />
and eroticism<br />
Resources<br />
McCarthy, B, & McCarthy, E. (2003). Rekindling desire: A step-bystep<br />
program <strong>to</strong> help low sex and no-sex marriages.NY: Brunner-<br />
Routledge<br />
www.sexual<br />
sexualityandu.ca/<br />
is committed <strong>to</strong> providing you<br />
credible and up-<strong>to</strong><br />
<strong>to</strong>-date information and education<br />
on sexual health. This web site is administered by<br />
the Society of Obstetricians and Gynaecologists of<br />
Canada.<br />
http://www.aasect.org/ The American Association of<br />
<strong>Sexual</strong>ity Educa<strong>to</strong>rs, Counselors and Therapists<br />
(AASECT)<br />
Program in Human <strong>Sexual</strong>ity, University of Minnesota<br />
http://www.fm.umn.edu/phs<br />
www.fm.umn.edu/phs/<br />
6