Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
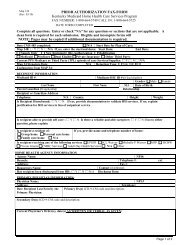
Required Information<br />
FIELD NUMBER NAME AND DESCRIPTION<br />
26 Patient’s Account No.<br />
Enter the office account number you have assigned to this member, if<br />
desired.<br />
28 Total Charge<br />
Enter the total of all individual charges entered in column 24F. Total<br />
each claim separately.<br />
29 Amount Paid<br />
Enter the amount paid, if any, by a private insurance not Medicare.<br />
30 Balance Due<br />
Enter the balance due if applicable.<br />
EXCEPTION: (If you are a certified Primary Care or Rural Health provider, or<br />
Community Mental Health provider, this field is only used for Medicare<br />
payments)<br />
Cabinet for Health and Family Services<br />
13