CHAT Tool - Offender Health Research Network
CHAT Tool - Offender Health Research Network
CHAT Tool - Offender Health Research Network

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
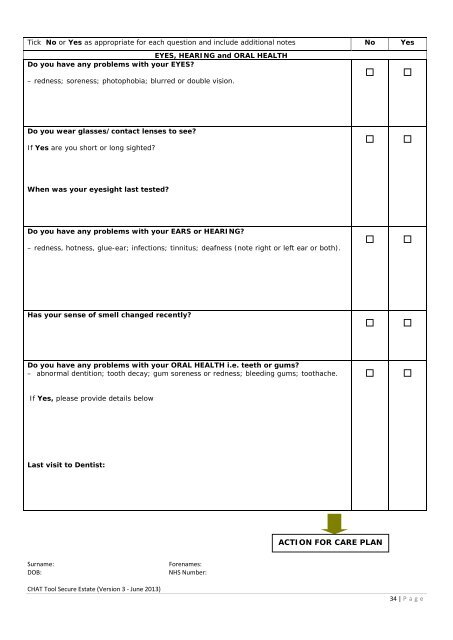
Tick No or Yes as appropriate for each question and include additional notes No Yes<br />
EYES, HEARING and ORAL HEALTH<br />
Do you have any problems with your EYES<br />
– redness; soreness; photophobia; blurred or double vision.<br />
Do you wear glasses/contact lenses to see<br />
If Yes are you short or long sighted<br />
When was your eyesight last tested<br />
Do you have any problems with your EARS or HEARING<br />
– redness, hotness, glue-ear; infections; tinnitus; deafness (note right or left ear or both).<br />
Has your sense of smell changed recently<br />
Do you have any problems with your ORAL HEALTH i.e. teeth or gums<br />
– abnormal dentition; tooth decay; gum soreness or redness; bleeding gums; toothache.<br />
If Yes, please provide details below<br />
Last visit to Dentist:<br />
ACTION FOR CARE PLAN<br />
Surname:<br />
DOB:<br />
Forenames:<br />
NHS Number:<br />
<strong>CHAT</strong> <strong>Tool</strong> Secure Estate (Version 3 - June 2013)<br />
34 | P age