Pulpal Diagnosis - University at Buffalo
Pulpal Diagnosis - University at Buffalo
Pulpal Diagnosis - University at Buffalo

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Eugene A. Pantera, Jr., DDS, MS<br />
Department of Periodontics and Endodontics<br />
Clinical <strong>Diagnosis</strong><br />
<strong>University</strong> <strong>at</strong> <strong>Buffalo</strong><br />
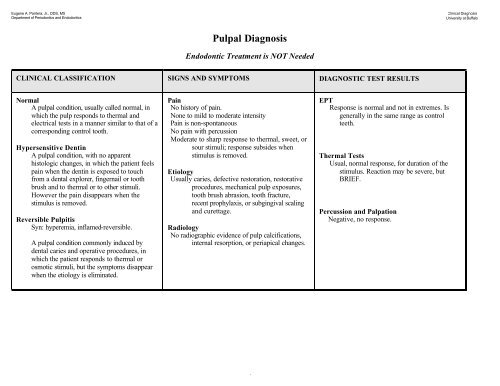
<strong>Pulpal</strong> <strong>Diagnosis</strong><br />
Endodontic Tre<strong>at</strong>ment is NOT Needed<br />
CLINICAL CLASSIFICATION SIGNS AND SYMPTOMS DIAGNOSTIC TEST RESULTS<br />
Normal<br />
A pulpal condition, usually called normal, in<br />
which the pulp responds to thermal and<br />
electrical tests in a manner similar to th<strong>at</strong> of a<br />
corresponding control tooth.<br />
Hypersensitive Dentin<br />
A pulpal condition, with no apparent<br />
histologic changes, in which the p<strong>at</strong>ient feels<br />
pain when the dentin is exposed to touch<br />
from a dental explorer, fingernail or tooth<br />
brush and to thermal or to other stimuli.<br />
However the pain disappears when the<br />
stimulus is removed.<br />
Reversible Pulpitis<br />
Syn: hyperemia, inflamed-reversible.<br />
A pulpal condition commonly induced by<br />
dental caries and oper<strong>at</strong>ive procedures, in<br />
which the p<strong>at</strong>ient responds to thermal or<br />
osmotic stimuli, but the symptoms disappear<br />
when the etiology is elimin<strong>at</strong>ed.<br />
Pain<br />
No history of pain.<br />
None to mild to moder<strong>at</strong>e intensity<br />
Pain is non-spontaneous<br />
No pain with percussion<br />
Moder<strong>at</strong>e to sharp response to thermal, sweet, or<br />
sour stimuli; response subsides when<br />
stimulus is removed.<br />
Etiology<br />
Usually caries, defective restor<strong>at</strong>ion, restor<strong>at</strong>ive<br />
procedures, mechanical pulp exposures,<br />
tooth brush abrasion, tooth fracture,<br />
recent prophylaxis, or subgingival scaling<br />
and curettage.<br />
Radiology<br />
No radiographic evidence of pulp calcific<strong>at</strong>ions,<br />
internal resorption, or periapical changes.<br />
EPT<br />
Response is normal and not in extremes. Is<br />
generally in the same range as control<br />
teeth.<br />
Thermal Tests<br />
Usual, normal response, for dur<strong>at</strong>ion of the<br />
stimulus. Reaction may be severe, but<br />
BRIEF.<br />
Percussion and Palp<strong>at</strong>ion<br />
Neg<strong>at</strong>ive, no response.<br />
1
Eugene A. Pantera, Jr., DDS, MS<br />
Department of Periodontics and Endodontics<br />
<strong>Pulpal</strong> <strong>Diagnosis</strong><br />
Endodontic Tre<strong>at</strong>ment IS Needed<br />
CLINICAL CLASSIFICATION SIGNS AND SYMPTOMS DIAGNOSTIC TEST RESULTS<br />
Irreversible Pulpitis<br />
Irreversible pulpitis without periapical p<strong>at</strong>hosis<br />
A pulpal condition, usually caused by deep<br />
dental caries or restor<strong>at</strong>ions, in which<br />
spontaneous pain may occur or be<br />
precipit<strong>at</strong>ed by thermal or other stimuli.<br />
Radiographs show no periapical changes.<br />
The pain last for several minutes to hours.<br />
Irreversible pulpitis with periapical p<strong>at</strong>hosis<br />
A pulpal condition similar to above, but in<br />
which periapical or l<strong>at</strong>eral radiographic<br />
changes are evident.<br />
Pain<br />
May have acute or chronic symptoms.<br />
Sharp, exagger<strong>at</strong>ed, painful response to thermal<br />
stimulus; pain lingers after stimulus is<br />
removed.<br />
Pain may be spontaneous; maybe past repe<strong>at</strong>ed<br />
episodes of pain, often continuous pain.<br />
Pain with mastic<strong>at</strong>ion.<br />
Etiology<br />
Deep caries and/or restor<strong>at</strong>ions, evidence of<br />
previous pulp cap.<br />
Exposed dentin (<strong>at</strong>trition, abrasion, and erosion).<br />
Traum<strong>at</strong>ic injuries.<br />
Resorption (especially perfor<strong>at</strong>ing).<br />
Orthodontic forces.<br />
EPT<br />
Tooth may test within normal limits.<br />
Response may be markedly different from<br />
control, rapid/delayed onset, persistent, and<br />
may be of severe intensity.<br />
Thermal Test<br />
A key factor in making a diagnosis.<br />
May be abnormal, rapid/delayed onset, gre<strong>at</strong>er<br />
intensity and longer dur<strong>at</strong>ion.<br />
Percussion Test<br />
May or may not be positive.<br />
Palp<strong>at</strong>ion<br />
May or may not be positive.<br />
Radiology<br />
May be normal.<br />
Radiographic evidence may reveal normal pulp,<br />
calcific<strong>at</strong>ions, narrow pulp chamber,<br />
"calcified" canals, , or condensing osteitis.<br />
An enlarged PDL may also be present.<br />
2
Eugene A. Pantera, Jr., DDS, MS<br />
Department of Periodontics and Endodontics<br />
<strong>Pulpal</strong> <strong>Diagnosis</strong><br />
Endodontic Tre<strong>at</strong>ment IS Needed<br />
CLINICAL CLASSIFICATION SIGNS AND SYMPTOMS DIAGNOSTIC TEST RESULTS<br />
Necrotic Pulp<br />
Necrotic pulp without periapical p<strong>at</strong>hosis<br />
A pulpal condition in which there may or<br />
may not be spontaneous moder<strong>at</strong>e to severe<br />
pain or pain elicited by various stimuli.<br />
Response to various testing modalities is<br />
usually absent. Radiographic changes are not<br />
evident.<br />
Necrotic pulp with periapical p<strong>at</strong>hosis<br />
A pulpal condition similar to above, except<br />
th<strong>at</strong> in this c<strong>at</strong>egory periapical or l<strong>at</strong>eral<br />
lesions are evident in radiographs.<br />
Pain<br />
May have acute or chronic symptoms.<br />
Pain may be spontaneous; maybe past repe<strong>at</strong>ed<br />
episodes of pain, often continuous, dull,<br />
throbbing, pain.<br />
Pain with mastic<strong>at</strong>ion.<br />
Etiology<br />
Deep caries and/or restor<strong>at</strong>ions, evidence of<br />
previous pulp cap.<br />
Carious pulp exposures.<br />
Exposed dentin (<strong>at</strong>trition, abrasion, and erosion).<br />
Traum<strong>at</strong>ic injuries.<br />
Resorption (especially perfor<strong>at</strong>ing).<br />
Orthodontic forces.<br />
EPT<br />
No response.<br />
May have false positives.<br />
Thermal Test<br />
No response.<br />
Percussion Test<br />
May or may not be positive.<br />
Palp<strong>at</strong>ion<br />
May or may not be positive.<br />
Radiology<br />
May be normal.<br />
May be periapical lesions or l<strong>at</strong>eral lesions.<br />
An enlarged PDL may also be present.<br />
3
Eugene A. Pantera, Jr., DDS, MS<br />
Department of Periodontics and Endodontics<br />
Periapical <strong>Diagnosis</strong><br />
There MAY be Need for Endodontic Tre<strong>at</strong>ment<br />
PULPAL DIAGNOSIS IS REQUIRED FOR DEFINITIVE DETERMINATION<br />
CLINICAL CLASSIFICATION SIGNS AND SYMPTOMS DIAGNOSTIC TEST RESULTS<br />
Acute Apical Periodontitis<br />
Pain<br />
History of pulpal pain.<br />
Moder<strong>at</strong>e to severe intensity th<strong>at</strong> may be<br />
intermittent.<br />
Periapical pain usually requires stimulus (eg<br />
mastic<strong>at</strong>ion).<br />
Pain can be sharp.<br />
Aggrav<strong>at</strong>ing factors are usually present.<br />
Etiology<br />
Irreversible pulpitis, traum<strong>at</strong>ic injuries,<br />
periodontal disease, orthodontic forces maxillary<br />
sinusitis, pressure from periapical tumors,<br />
restor<strong>at</strong>ion in hyperocclusion.<br />
Pulp Tests<br />
EPT and Thermal tests may be normal, or<br />
similar to irreversible pulpitis or pulpal<br />
necrosis.<br />
Percussion<br />
Moder<strong>at</strong>e to severe pain.<br />
Palp<strong>at</strong>ion<br />
Moder<strong>at</strong>e to severe pain.<br />
Radiology<br />
Usually thickening of PDL, also can have<br />
periapical or l<strong>at</strong>eral radiolucency, or normal.<br />
Chronic Apical Periodontitis<br />
A periapical condition characterized by none<br />
to slight pain on mastic<strong>at</strong>ion but may present<br />
itself with varying degrees of apical swelling.<br />
Radiographs reveal periapical or l<strong>at</strong>eral<br />
radiolucencies.<br />
Pain<br />
History of pain.<br />
Slight intensity to no pain. Pain may be absent or<br />
constant.<br />
Periapical pain can be spontaneous.<br />
Pain is dull throbbing.<br />
Pain can occur with mastic<strong>at</strong>ion.<br />
Etiology<br />
Same as for Acute apical periodontitis.<br />
Pulp Tests<br />
EPT and Thermal tests may be normal, or<br />
similar to irreversible pulpitis or pulpal<br />
necrosis.<br />
Percussion<br />
Moder<strong>at</strong>e to none.<br />
Palp<strong>at</strong>ion<br />
Moder<strong>at</strong>e to none. May be swelling.<br />
Radiology<br />
Periapical or l<strong>at</strong>eral radiolucency.<br />
4
Eugene A. Pantera, Jr., DDS, MS<br />
Department of Periodontics and Endodontics<br />
Periapical <strong>Diagnosis</strong><br />
There IS a Need for Endodontic Tre<strong>at</strong>ment<br />
PULPAL DIAGNOSIS IS REQUIRED FOR DEFINITIVE DETERMINATION<br />
CLINICAL CLASSIFICATION SIGNS AND SYMPTOMS DIAGNOSTIC TEST RESULTS<br />
Chronic Suppur<strong>at</strong>ive Apical Periodontitis<br />
A periapical condition characterized by non<br />
pain on mastic<strong>at</strong>ion. A draining sinus tract or<br />
other evidence of suppur<strong>at</strong>ion is evident.<br />
Radiographs reveal periapical or l<strong>at</strong>eral<br />
radiolucencies.<br />
Acute Alveolar Abscess<br />
Syn: Acute apical abscess<br />
An acute alveolar abscess is a severe clinical<br />
manifest<strong>at</strong>ion of periapical infectious<br />
disease, characterized by severe pain and<br />
swelling.<br />
Pain<br />
History of pain.<br />
Usually no pain present.<br />
Etiology<br />
Irreversible pulpitis, traum<strong>at</strong>ic injuries,<br />
periodontal disease, orthodontic forces,<br />
restor<strong>at</strong>ion in hyperocclusion.<br />
Pain<br />
History of pain.<br />
Severe intensity.<br />
Constant and spontaneous pain.<br />
Pain is pulsing and throbbing.<br />
Pain can occur with mastic<strong>at</strong>ion.<br />
Etiology<br />
The result of coronal apical progression of pulpal<br />
necrosis with resultant release of antigens into<br />
the periapical tissues.<br />
Pulp Tests<br />
EPT and Thermal tests may be normal, or<br />
similar to irreversible pulpitis or pulpal<br />
necrosis. (Is this a lesion of endodontic origin)<br />
Percussion<br />
None to slight pain.<br />
Palp<strong>at</strong>ion<br />
Slightly tender.<br />
Radiology<br />
Periapical or l<strong>at</strong>eral radiolucency.<br />
Visual<br />
Sinus tract present.<br />
Pulp Tests<br />
No response.<br />
Percussion<br />
Moder<strong>at</strong>e to severe.<br />
Palp<strong>at</strong>ion<br />
Moder<strong>at</strong>e to severe. Swelling probable.<br />
Radiology<br />
PDL thickening, periapical or l<strong>at</strong>eral<br />
radiolucency.<br />
5