Pulpal Diagnosis - University at Buffalo
Pulpal Diagnosis - University at Buffalo
Pulpal Diagnosis - University at Buffalo

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Eugene A. Pantera, Jr., DDS, MS<br />
Department of Periodontics and Endodontics<br />
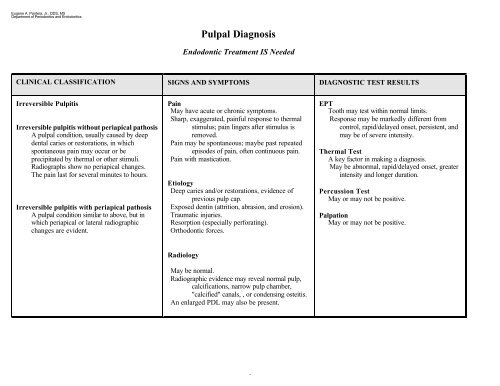
<strong>Pulpal</strong> <strong>Diagnosis</strong><br />
Endodontic Tre<strong>at</strong>ment IS Needed<br />
CLINICAL CLASSIFICATION SIGNS AND SYMPTOMS DIAGNOSTIC TEST RESULTS<br />
Irreversible Pulpitis<br />
Irreversible pulpitis without periapical p<strong>at</strong>hosis<br />
A pulpal condition, usually caused by deep<br />
dental caries or restor<strong>at</strong>ions, in which<br />
spontaneous pain may occur or be<br />
precipit<strong>at</strong>ed by thermal or other stimuli.<br />
Radiographs show no periapical changes.<br />
The pain last for several minutes to hours.<br />
Irreversible pulpitis with periapical p<strong>at</strong>hosis<br />
A pulpal condition similar to above, but in<br />
which periapical or l<strong>at</strong>eral radiographic<br />
changes are evident.<br />
Pain<br />
May have acute or chronic symptoms.<br />
Sharp, exagger<strong>at</strong>ed, painful response to thermal<br />
stimulus; pain lingers after stimulus is<br />
removed.<br />
Pain may be spontaneous; maybe past repe<strong>at</strong>ed<br />
episodes of pain, often continuous pain.<br />
Pain with mastic<strong>at</strong>ion.<br />
Etiology<br />
Deep caries and/or restor<strong>at</strong>ions, evidence of<br />
previous pulp cap.<br />
Exposed dentin (<strong>at</strong>trition, abrasion, and erosion).<br />
Traum<strong>at</strong>ic injuries.<br />
Resorption (especially perfor<strong>at</strong>ing).<br />
Orthodontic forces.<br />
EPT<br />
Tooth may test within normal limits.<br />
Response may be markedly different from<br />
control, rapid/delayed onset, persistent, and<br />
may be of severe intensity.<br />
Thermal Test<br />
A key factor in making a diagnosis.<br />
May be abnormal, rapid/delayed onset, gre<strong>at</strong>er<br />
intensity and longer dur<strong>at</strong>ion.<br />
Percussion Test<br />
May or may not be positive.<br />
Palp<strong>at</strong>ion<br />
May or may not be positive.<br />
Radiology<br />
May be normal.<br />
Radiographic evidence may reveal normal pulp,<br />
calcific<strong>at</strong>ions, narrow pulp chamber,<br />
"calcified" canals, , or condensing osteitis.<br />
An enlarged PDL may also be present.<br />
2