Understanding Your Explanation of Benefits - WPS Health Insurance ...
Understanding Your Explanation of Benefits - WPS Health Insurance ...
Understanding Your Explanation of Benefits - WPS Health Insurance ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Understanding</strong> <strong>Your</strong><br />
<strong>Explanation</strong> <strong>of</strong> <strong>Benefits</strong><br />
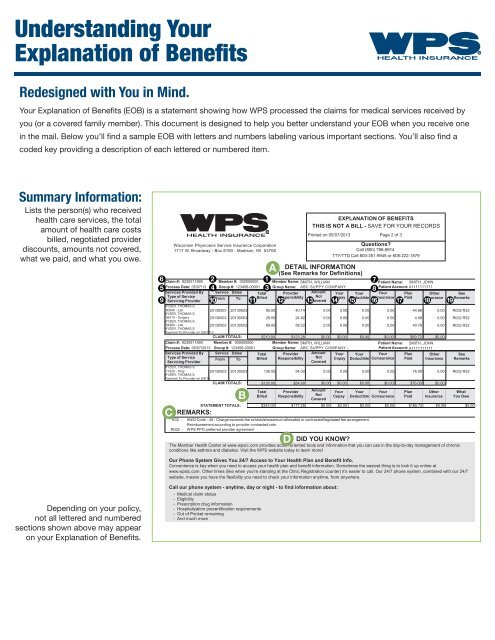
Redesigned with You in Mind.<br />
<strong>Your</strong> <strong>Explanation</strong> <strong>of</strong> <strong>Benefits</strong> (EOB) is a statement showing how <strong>WPS</strong> processed the claims for medical services received by<br />
you (or a covered family member). This document is designed to help you better understand your EOB when you receive one<br />
in the mail. Below you’ll find a sample EOB with letters and numbers labeling various important sections. You’ll also find a<br />
coded key providing a description <strong>of</strong> each lettered or numbered item.<br />
Summary Information:<br />
Lists the person(s) who received<br />
health care services, the total<br />
amount <strong>of</strong> health care costs<br />
billed, negotiated provider<br />
discounts, amounts not covered,<br />
what we paid, and what you owe.<br />
6<br />
5<br />
Total<br />
Billed<br />
Provider<br />
Responsibility<br />
EXPLANATION OF BENEFITS<br />
THIS IS NOT A BILL - SAVE FOR YOUR RECORDS<br />
Printed on 05/07/2013 Page 2 <strong>of</strong> 3<br />
DETAIL INFORMATION<br />
(See Remarks for Definitions)<br />
Amount<br />
Not<br />
Covered<br />
Questions<br />
Call (800) 798-8914<br />
TTY/TTD Call 800-351-9945 or 608-222-1879<br />
Claim #: 9239311890 Member #: 000000000 Member Name: SMITH, WILLIAM Patient Name: SMITH, JOHN<br />
Process Date: 05/07/13<br />
4<br />
Group #: 123456-00001<br />
3<br />
Group Name: ABC SUPPY COMPANY Patient Account: A1111111111<br />
8<br />
Services Provided By Service Dates Total Provider Amount <strong>Your</strong> <strong>Your</strong> <strong>Your</strong> Plan Other See<br />
Type <strong>of</strong> Service<br />
From To Billed Responsibility Not Copay Deductible Coinsurance Paid <strong>Insurance</strong> Remarks<br />
Servicing Provider<br />
Covered<br />
HYZER, THOMAS S.<br />
80048 - Lab<br />
20130503 20130503 85.00<br />
40.14 0.00 0.00 0.00 0.00 44.86 0.00<br />
HYZER, THOMAS S.<br />
36415 - Surgery<br />
20130503 20130503 29.00<br />
24.92 0.00 0.00 0.00 0.00<br />
4.08 0.00<br />
HYZER, THOMAS S.<br />
84484 - Lab<br />
20130503 20130503 99.00<br />
58.22 0.00 0.00 0.00 0.00 40.78 0.00<br />
HYZER, THOMAS S.<br />
Payment To Provider on 5/8/2013<br />
CLAIM TOTALS: $213.00 $123.28 $0.00 $0.00 $0.00 $0.00 $89.72 $0.00<br />
Claim #: 9239311890 Member #: 000000000 Member Name: SMITH, WILLIAM Patient Name: SMITH, JOHN<br />
Process Date: 05/07/2013 Group #: 123456-00001 Group Name: ABC SUPPY COMPANY - Patient Account: A1111111111<br />
Services Provided By Service Dates Total Provider Amount <strong>Your</strong> <strong>Your</strong> <strong>Your</strong> Plan Other See<br />
Type <strong>of</strong> Service<br />
Servicing Provider<br />
From To Billed Responsibility Not<br />
Covered<br />
<strong>Your</strong><br />
Copay<br />
<strong>Your</strong><br />
Deductible<br />
<strong>Your</strong><br />
Coinsurance<br />
Plan<br />
Paid<br />
Other<br />
<strong>Insurance</strong><br />
R032 R32<br />
R032 R32<br />
R032 R32<br />
Copay Deductible Coinsurance Paid <strong>Insurance</strong> Remarks<br />
HYZER, THOMAS S.<br />
71020 - Xray<br />
20130503 20130503 130.00 54.00 0.00 0.00 0.00 0.00 76.00 0.00 R032 R32<br />
HYZER, THOMAS S.<br />
Payment To Provider on 5/8/13<br />
CLAIM TOTALS: $130.00 $54.00 $0.00 $0.00 $0.00 $0.00 $76.00 $0.00<br />
C<br />
Wisconsin Physicians Service <strong>Insurance</strong> Corporation<br />
1717 W. Broadway - Box 8190 - Madison, WI 53708<br />
2<br />
STATEMENT TOTALS:<br />
REMARKS:<br />
B<br />
1<br />
A<br />
9 10 11 12 13 14 15 16 17 18 19<br />
What<br />
You Owe<br />
$343.00 $177.28 $0.00 $0.00 $0.00 $0.00 $165.72 $0.00 $0.00<br />
R32 - ANSI Code - 45 : Charge exceeds fee schedule/maximum allowable or contracted/legislated fee arrangement.<br />
Reimbursement according to provider contracted rate.<br />
R032 - <strong>WPS</strong> PPO preferred provider agreement<br />
D<br />
DID YOU KNOW<br />
The Member <strong>Health</strong> Center at www.wpsic.com provides action-oriented tools and information that you can use in the day-to-day management <strong>of</strong> chronic<br />
conditions like asthma and diabetes. Visit the <strong>WPS</strong> website today to learn more!<br />
7<br />
Our Phone System Gives You 24/7 Access to <strong>Your</strong> <strong>Health</strong> Plan and Benefit Info.<br />
Convenience is key when you need to access your health plan and benefit information. Sometimes the easiest thing is to look it up online at<br />
www.wpsic.com. Other times (like when you're standing at the Clinic Registration counter) it's easier to call. Our 24/7 phone system, combined with our 24/7<br />
website, means you have the flexibility you need to check your information anytime, from anywhere.<br />
Depending on your policy,<br />
not all lettered and numbered<br />
sections shown above may appear<br />
on your <strong>Explanation</strong> <strong>of</strong> <strong>Benefits</strong>.<br />
Call our phone system - anytime, day or night - to find information about:<br />
- Medical claim status<br />
- Eligibility<br />
- Prescription drug information<br />
- Hospitalization precertification requirements<br />
- Out <strong>of</strong> Pocket remaining<br />
- And much more
A<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
7<br />
8<br />
9<br />
10<br />
11<br />
12<br />
13<br />
14<br />
15<br />
16<br />
Detail Information<br />
Provides details on each medical service provided.<br />
Member Name: The person insured by <strong>WPS</strong><br />
(policyholder).<br />
Member Number: Number associated with each<br />
member, shown on your <strong>WPS</strong> ID card.<br />
Group Name: Employer Name (if covered under<br />
a group plan) or Individual Plan Name (if covered<br />
under an individual plan).<br />
Group-Division Number: Unique code identifying<br />
your health plan in our claims system.<br />
Process Date: The date <strong>WPS</strong> processed this claim.<br />
Claim Number: Unique code identifying the claim<br />
submitted.<br />
Patient Name: Lists the person(s) who received<br />
health care services.<br />
Patient Account: Unique health care provider code<br />
identifying the patient treated.<br />
Services Provided By: The provider that performed<br />
the procedure, plus the code and general category <strong>of</strong><br />
the procedure performed.<br />
Service Dates: The start and end date during which<br />
the listed procedure was performed.<br />
Total Billed: The total cost <strong>of</strong> the procedure, as<br />
billed by the provider.<br />
Provider Responsibilityt: The discount <strong>WPS</strong> negotiated<br />
with your provider, which will be subtracted from the<br />
total cost. Usually based on contractual agreements<br />
between <strong>WPS</strong> and providers in your <strong>WPS</strong> network.<br />
Amount Not Covered: The portion <strong>of</strong> the total cost<br />
not covered under your health plan. This portion is<br />
your responsibility. See Remarks codes in the last<br />
column and the Remarks box for explanation.<br />
<strong>Your</strong> Copay: The portion <strong>of</strong> the total cost you<br />
are responsible to pay before any deductible or<br />
coinsurance is applied for certain covered services<br />
(e.g., <strong>of</strong>fice visits).<br />
<strong>Your</strong> Deductible: The portion <strong>of</strong> total cost applied<br />
to your deductible. (<strong>Your</strong> deductible is the amount<br />
<strong>of</strong> covered charges you must pay each calendar year<br />
before <strong>WPS</strong> pays benefits).(e.g., <strong>of</strong>fice visits).<br />
<strong>Your</strong> Coinsurance: The balance <strong>of</strong> total cost after<br />
subtracting provider discount, ineligible amount,<br />
copay, and deductible.<br />
17<br />
18<br />
19<br />
B<br />
C<br />
D<br />
Plan Plaid: The percentage <strong>of</strong> the coinsurance<br />
amount paid by <strong>WPS</strong>.<br />
Other <strong>Insurance</strong>: The portion <strong>of</strong> the coinsurance<br />
paid by another insurance plan (e.g., auto<br />
insurance).<br />
See Remarks: The procedure performed may have<br />
triggered additional comments that do not fit in<br />
the chart. Match the Remarks code to those in the<br />
Remarks box under the chart to view the specific<br />
comment.<br />
Statement Totals<br />
A summary <strong>of</strong> total charges billed by health care<br />
providers, negotiated provider discounts, <strong>WPS</strong>’<br />
financial responsibility and yours. What you owe<br />
is the portion <strong>of</strong> coinsurance you are responsible<br />
to pay. Includes copay, deductible, coinsurance,<br />
and any amount not covered. Paid directly to your<br />
provider, who will send you a bill.<br />
Remarks<br />
Includes explanations <strong>of</strong> any Remarks codes listed<br />
in the See Remarks column.<br />
Did You Know<br />
Tips and announcements to help you get the most<br />
out <strong>of</strong> your benefit plan.<br />
Please consult your Member Guide for more<br />
detailed definitions <strong>of</strong> these terms. If you have any<br />
questions, please contact Member Services at the<br />
number listed on the back <strong>of</strong> your <strong>WPS</strong> ID card.<br />
©2013 Wisconsin Physicians Service <strong>Insurance</strong> Corporation. All rights reserved. 18502-021- 1008