Antenatal Home Care Program Referral Form
Antenatal Home Care Program Referral Form
Antenatal Home Care Program Referral Form

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
AHCP pager # 932-7973<br />
AHCP fax #940-2189<br />
Women’s:<br />
ANTENATAL HOME CARE PROGRAM<br />
REFERRAL FORM (Draft)<br />
WRS5____PNAU___Other____<br />
NAME:<br />
D.O.B.<br />
MHSC#:<br />
ADDRESSOGRAPH<br />
St. Boniface: B3____Triage___Other____<br />
PHIN#:<br />
Dr.<br />
Diagnosis: HYPERTENSION PPROM TPTL Other______________<br />
Address: ______________________________Temporary address:<br />
Phone: _______________________________<br />
Contact person name & phone: __________________________________<br />
G________P________ Gestation____________ EDC_______________________<br />
Social Supports: _____________________________________________<br />
Hospital admission date: ____________ Discharge date: ___________________<br />
Range of vital signs (past 24 hours):_____________________________________________<br />
BP cuff size: Regular Large WT: __________<br />
Condition Summary/ Significant Psychosocial and Medical Hx:<br />
____________________________________________________________________________________<br />
_______________________________________________________________________________<br />
______________________________________________________________________________<br />
_____________________________________________________________________________________<br />
Discharge Medications: _________________________________________________________<br />
FAU:<br />
Date___________BPS:________Presentation___________AFV____________EFW______<br />
Next Appointments:<br />
FAU ______________ Dr. ____________________ Other ____________________<br />
Include with referral form: Prenatal sheet<br />
FAU report<br />
Vital signs flow sheet<br />
Latest lab results<br />
Nursing database<br />
Completed by:(Print)_________________(Signature):________________ Date:____________<br />
July 26, 2009
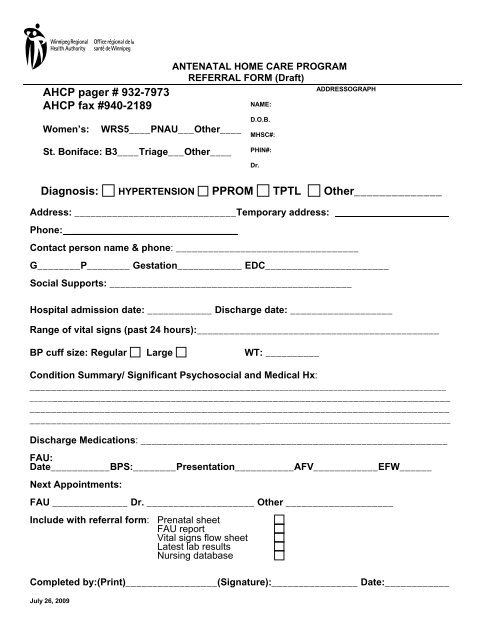
Guidelines for Completion of the AHCP <strong>Referral</strong> <strong>Form</strong><br />
In early 2009 revisions to the <strong>Antenatal</strong> <strong>Home</strong> <strong>Care</strong> <strong>Program</strong>’s referral form were made in consultation with the<br />
nursing staff at both the St. Boniface and Women’s Hospitals. The form now consists of a one page document with<br />
the date July 26, 2009 at the bottom. The goal of the form is to provide key information to the AHCP nurses while<br />
increasing ease of use for nurses on the busy inpatient units.<br />
The same referral form is used by the hospital staff in the following areas: triage/PNAU, antepartum, L&D/LDRP<br />
and FAU. The <strong>Antenatal</strong> <strong>Home</strong> <strong>Care</strong> nurses use the form to take referrals from doctor’s office and clinics via the<br />
phone.<br />
The following key points may assist inpatient sites in making a referral:<br />
1. The patient referred to the program from hospital normally has the requested information on various forms, within<br />
her hospital chart i.e. lab results, vital sign flow sheet. These forms can be faxed as is, rather than having a nurse<br />
or unit clerk duplicate information by writing it out again on the referral form.<br />
2. The pager and fax numbers for the AHCP are in the top left portion of the form, under the area identifying the<br />
hospital and unit generating the referral.<br />
Any questions, just contact the caseload coordinator. A call prior to faxing the referral is necessary to ensure there<br />
is room on the program for your patient. Page 932-7973 and a nurse will call you back.<br />
3. Use addressograph to avoid writing in key demographic information.<br />
4. Check the box in front of the condition patient requires monitoring of.<br />
5. Complete address, temporary address if applicable, and phone numbers (home and cellular) as this is vital<br />
information to ensure that the client can be contacted and visited promptly after she leaves hospital.<br />
6. Contact person- will be called if client is not at home address or phone number listed.<br />
7. Gravida/ Parity/ Gestation and EDC- must be completed.<br />
8. Hospital admission date and discharge date- a referral form may be sent on a client prior to discharge home.<br />
The AHCP nurse will refer to the discharge date, and on that date will confirm patient has gone home and whether<br />
any changes in condition have occurred.<br />
9. Range of vital signs (past 24 hrs): no need to complete if sending by fax the vital signs flow sheet from patient<br />
chart.<br />
10. BP cuff size: indicate by checking appropriate sized cuff that was used on the patient in the hospital.<br />
The AHCP lends each GH patient an auto BP cuff- knowing in advance the cuff size ensures the proper cuff is<br />
brought to the visit.<br />
11. Weight: most recent weight in kilograms, used for ongoing 24 hr urine samples to run creatinine clearance.<br />
12. Condition summary/Significant psychosocial and medical history:<br />
List frequency of warning signs and symptoms related to current condition, presence of any chronic illnesses,<br />
previous pregnancy complications.<br />
When client has received corticosteroids in hospital, note it here.<br />
13. Discharge medications: complete name, dose and schedule for all medications client is to take when at home.<br />
14. FAU: if report will be faxed separately, no need to complete this area.<br />
15. Next appointments: identify dates as booked. If return appointment needs to be arranged by patient or<br />
program nurse, write that in.<br />
16. Include with referral form: check off the items being sent with referral form. All items listed are requested by<br />
the program.<br />
17. Completed by: (Print) / (Signature) of person completing the form. Used by AHCP nurses as contact for more<br />
information when required.<br />
18. Date: date form once completed. This referral form becomes the first portion of the patient’s home chart and<br />
should include date information was transferred to AHCP.<br />
Created on May 10, 2009 by Karen Daeninck, revised June 27 and July 26, 2009