Sleep History Questionnaire - Emory Johns Creek Hospital
Sleep History Questionnaire - Emory Johns Creek Hospital
Sleep History Questionnaire - Emory Johns Creek Hospital
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
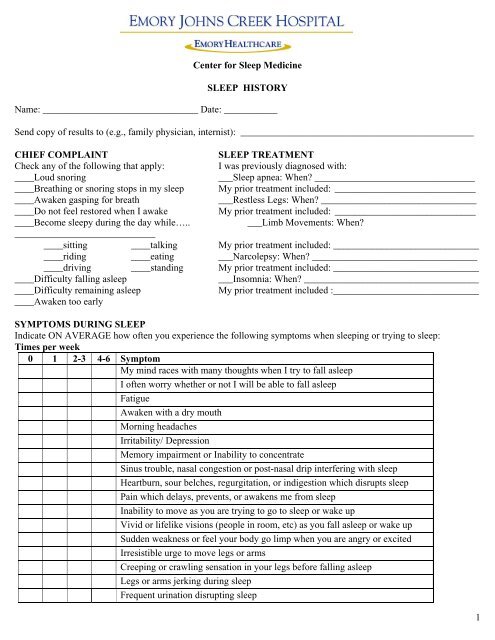
Center for <strong>Sleep</strong> Medicine<br />
SLEEP HISTORY<br />
Name: ________________________________ Date: ___________<br />
Send copy of results to (e.g., family physician, internist): ________________________________________________<br />
CHIEF COMPLAINT<br />
SLEEP TREATMENT<br />
Check any of the following that apply:<br />
I was previously diagnosed with:<br />
____Loud snoring<br />
___<strong>Sleep</strong> apnea: When _________________________________<br />
____Breathing or snoring stops in my sleep My prior treatment included: _____________________________<br />
____Awaken gasping for breath<br />
___Restless Legs: When ________________________________<br />
____Do not feel restored when I awake<br />
My prior treatment included: _____________________________<br />
____Become sleepy during the day while…..<br />
___Limb Movements: When<br />
_____________________________<br />
____sitting ____talking My prior treatment included: ______________________________<br />
____riding ____eating ___Narcolepsy: When __________________________________<br />
____driving ____standing My prior treatment included: ______________________________<br />
____Difficulty falling asleep<br />
___Insomnia: When ____________________________________<br />
____Difficulty remaining asleep<br />
My prior treatment included :______________________________<br />
____Awaken too early<br />
SYMPTOMS DURING SLEEP<br />
Indicate ON AVERAGE how often you experience the following symptoms when sleeping or trying to sleep:<br />
Times per week<br />
0 1 2-3 4-6 Symptom<br />
My mind races with many thoughts when I try to fall asleep<br />
I often worry whether or not I will be able to fall asleep<br />
Fatigue<br />
Awaken with a dry mouth<br />
Morning headaches<br />
Irritability/ Depression<br />
Memory impairment or Inability to concentrate<br />
Sinus trouble, nasal congestion or post-nasal drip interfering with sleep<br />
Heartburn, sour belches, regurgitation, or indigestion which disrupts sleep<br />
Pain which delays, prevents, or awakens me from sleep<br />
Inability to move as you are trying to go to sleep or wake up<br />
Vivid or lifelike visions (people in room, etc) as you fall asleep or wake up<br />
Sudden weakness or feel your body go limp when you are angry or excited<br />
Irresistible urge to move legs or arms<br />
Creeping or crawling sensation in your legs before falling asleep<br />
Legs or arms jerking during sleep<br />
Frequent urination disrupting sleep<br />
1
Name ____________________<br />
<strong>Sleep</strong> talking or <strong>Sleep</strong> walking<br />
SLEEP HABITS<br />
At what time do you usually get in the bed___________AM/PM<br />
How long does it take you to fall asleep after you have turned out the lights_________minutes/hours<br />
How often do you awaken each night___________minutes/<br />
The total time I spend awake in bed____________minutes/hours<br />
I usually wake up from sleep at_______________AM/PM<br />
What time do you usually get out of bed from sleep______________AM/PM<br />
Indicate total length of naps daily_____________<br />
If you do rotating shift work, or have other work schedule changes and need more space to describe:<br />
___________________________________________________________________________________________<br />
___________________________________________________________________________________________________<br />
MEDICAL HISTORY<br />
Please check if you have had any of the following:<br />
( )Heart disease List type: ____________________ ( )Diabetes ( )Depression<br />
( )High blood pressure ( )Asthma/Emphysema ( )Reflux ( )Thyroid condition<br />
( )Fibromyalgia ( )Anxiety ( )Seizures ( )Parkinson’s disease<br />
( )Stroke ( )Head Injury or brain surgery<br />
( )Other medical problems (please list):______________________________________________________________<br />
______________________________________________________________________________________________<br />
WEIGHT HISTORY<br />
What do you weigh now _______ What was your weight 1 year ago _______ 5 years ago _______<br />
Any changes in collar size 1 year ago _______ 5 years ago _______<br />
MEDICATION<br />
Do you take anything to help you sleep<br />
What______________________ How often___________<br />
List any drug allergies and reactions: ________________________________________________________________<br />
List current medications and dosages, including both prescriptions and over-the-counter medications: ____________<br />
______________________________________________________________________________________________<br />
______________________________________________________________________________________________<br />
SOCIAL HISTORY<br />
Do you smoke __ Did you previously smoke ______How many years of smoking _____ How much per day____<br />
Do you drink alcohol How much __________ drinks per (day/week/month) (please circle)<br />
How much caffeinated coffee, tea or cola do you drink daily _______________<br />
FAMILY HISTORY (Please check all that apply)<br />
Is there a family history of:<br />
Apnea Snoring Narcolepsy Insomnia Restless Legs<br />
Syndrome<br />
Other <strong>Sleep</strong><br />
Disturbances<br />
Mother <br />
Father <br />
Sister(s) <br />
.<br />
2
Name ____________________<br />
Brother(s) <br />
Grandparent(s) <br />
Epworth <strong>Sleep</strong>iness Scale<br />
How likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired This refers to<br />
your usual way of life in recent times. Even if you have not done some of these things recently, try to work out how<br />
they would have affected you. Use the following scale to choose the most appropriate number for each situation.<br />
0 = would never doze<br />
1 = slight chance of dozing<br />
2 = moderate chance of dozing<br />
3 = high chance of dozing<br />
Situation<br />
Chance of<br />
Dozing<br />
Sitting and reading<br />
……………………………………………………………………….<br />
Watching TV …………………………………………………………………………….<br />
Sitting, inactive, in a public place (e.g., a theater or a meeting) ………………...............<br />
As a passenger in a car for an hour without a break<br />
……………………………………..<br />
Lying down to rest in the afternoon when circumstances permit<br />
………………………..<br />
Sitting and talking with someone……………………………… ………………………..<br />
Sitting quietly after a lunch without alcohol …………………………………………….<br />
In a car, while stopped for a few minutes in traffic ……………………………………..<br />
Total<br />
_________<br />
_________<br />
_________<br />
_________<br />
_________<br />
_________<br />
_________<br />
_________<br />
_________<br />
.<br />
3