Pain Center Initial Visit Evaluation Form - Emory Johns Creek Hospital
Pain Center Initial Visit Evaluation Form - Emory Johns Creek Hospital
Pain Center Initial Visit Evaluation Form - Emory Johns Creek Hospital

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
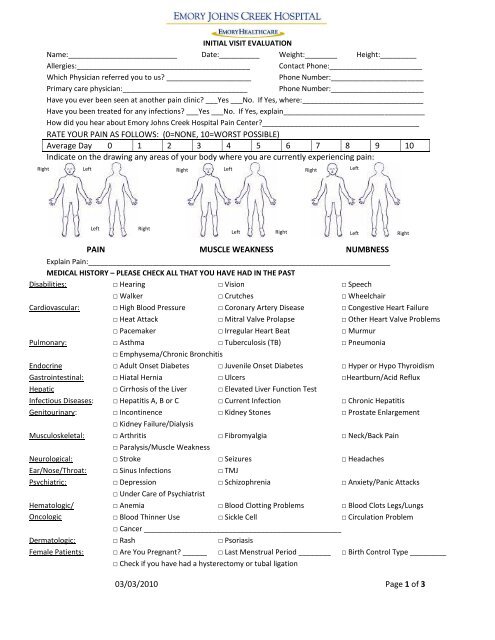
INITIAL VISIT EVALUATION<br />
Name:___________________________ Date:__________ Weight:________ Height:_________<br />
Allergies:___________________________________________ Contact Phone:_______________________<br />
Which Physician referred you to us _____________________ Phone Number:_______________________<br />
Primary care physician:_______________________________ Phone Number:_______________________<br />
Have you ever been seen at another pain clinic ___Yes ___No. If Yes, where:______________________________<br />
Have you been treated for any infections ___Yes ___No. If Yes, explain___________________________________<br />
How did you hear about <strong>Emory</strong> <strong>Johns</strong> <strong>Creek</strong> <strong>Hospital</strong> <strong>Pain</strong> <strong>Center</strong>_______________________________________<br />
RATE YOUR PAIN AS FOLLOWS: (0=NONE, 10=WORST POSSIBLE)<br />
Average Day 0 1 2 3 4 5 6 7 8 9 10<br />
Indicate on the drawing any areas of your body where you are currently experiencing pain:<br />
Right<br />
Left<br />
Right<br />
Left<br />
Right<br />
Left<br />
Left<br />
Right<br />
Left<br />
Right<br />
Left<br />
Right<br />
PAIN MUSCLE WEAKNESS NUMBNESS<br />
Explain <strong>Pain</strong>:___________________________________________________________________________<br />
MEDICAL HISTORY – PLEASE CHECK ALL THAT YOU HAVE HAD IN THE PAST<br />
Disabilities: □ Hearing □ Vision □ Speech<br />
□ Walker □ Crutches □ Wheelchair<br />
Cardiovascular: □ High Blood Pressure □ Coronary Artery Disease □ Congestive Heart Failure<br />
□ Heat Attack □ Mitral Valve Prolapse □ Other Heart Valve Problems<br />
□ Pacemaker □ Irregular Heart Beat □ Murmur<br />
Pulmonary: □ Asthma □ Tuberculosis (TB) □ Pneumonia<br />
□ Emphysema/Chronic Bronchitis<br />
Endocrine □ Adult Onset Diabetes □ Juvenile Onset Diabetes □ Hyper or Hypo Thyroidism<br />
Gastrointestinal: □ Hiatal Hernia □ Ulcers □Heartburn/Acid Reflux<br />
Hepatic □ Cirrhosis of the Liver □ Elevated Liver Function Test<br />
Infectious Diseases: □ Hepatitis A, B or C □ Current Infection □ Chronic Hepatitis<br />
Genitourinary: □ Incontinence □ Kidney Stones □ Prostate Enlargement<br />
□ Kidney Failure/Dialysis<br />
Musculoskeletal: □ Arthritis □ Fibromyalgia □ Neck/Back <strong>Pain</strong><br />
□ Paralysis/Muscle Weakness<br />
Neurological: □ Stroke □ Seizures □ Headaches<br />
Ear/Nose/Throat: □ Sinus Infections □ TMJ<br />
Psychiatric: □ Depression □ Schizophrenia □ Anxiety/Panic Attacks<br />
□ Under Care of Psychiatrist<br />
Hematologic/<br />
Oncologic<br />
□ Anemia □ Blood Clotting Problems □ Blood Clots Legs/Lungs<br />
□ Blood Thinner Use □ Sickle Cell □ Circulation Problem<br />
□ Cancer _________________________________________________<br />
Dermatologic: □ Rash □ Psoriasis<br />
Female Patients: □ Are You Pregnant ______ □ Last Menstrual Period ________ □ Birth Control Type _________<br />
□ Check if you have had a hysterectomy or tubal ligation<br />
03/03/2010 Page 1 of 3
CURRENT MEDICATIONS INCLUDING OVER-THE-COUNTER, COUMADIN OR OTHER TYPE OF BLOOD THINNER, VITAMIN E<br />
Name Dose Frequency<br />
Prior Surgeries/Anesthesia/<strong>Pain</strong> Treatments<br />
Approximate Date<br />
Family History: List diseases that run in your family:________________________________________________<br />
Social History: Smoking (Packs/Day______ Drugs____________ Alcohol Use (Amount)____________________<br />
Occupation:_____________________ Disabled ___Yes ___No If Yes, give reason________________________<br />
REVIEW OF SYSTEMS – PLEASE CHECK IF YOU HAVE ANY OF THE FOLLOWING NOW:<br />
Constitutional: □ Fatigue □ Drowsiness □ Weight Gain □ Weight Loss<br />
□ Dizziness<br />
□ Fever<br />
Cardiovascular: □ Chest <strong>Pain</strong> □ Palpitations □ Fainting<br />
Pulmonary: □ Shortness of Breath □ Cough □ Wheezing<br />
Gastrointestinal: □ Nausea □ Vomiting □ Abdominal <strong>Pain</strong><br />
□ Heartburn □ Diarrhea □ Constipation<br />
□ Bleeding<br />
□ Bowel Incontinence<br />
Genitourinary: □Difficulty Urinating □ Burning □ Urinary Incontinence<br />
□ Frequency<br />
□ Discharge<br />
Musculoskeletal: □ Muscle Aches □ Muscle Weakness □ Decreased Range of Motion<br />
□ Neck <strong>Pain</strong><br />
□ Back <strong>Pain</strong><br />
Ear/Nose/Throat: □ Sinus Infections □ TMJ<br />
Dermatological: □ Swelling □ Rash □ Bruises □ Lesions<br />
Psychiatric: □ Decreased Appetite □ Difficulty Sleeping □ Mania □ Paranoia<br />
□ Depression □ Early Morning Awakening □ Agitation □ Anxiety<br />
Hematologic: □ Bleeding Problems<br />
Discharge Planning<br />
Who will acompany you to the hospital on the day of your procedure __________________________<br />
Who will assist you at home after your procedure __________________________________________<br />
How Do You Learn Best Choose the best methods:<br />
□ Demonstration □ Reading □ Hearing □ Diagrams □ Videos □ Pamphlets<br />
Education: □ I have received the <strong>Pain</strong> Management guide and understand use of pain scale to evaluate intensity of<br />
pain.<br />
□ I have questions about the pain scale<br />
03/03/2010 Page 2 of 3
Signature of Patient or Person Completing <strong>Form</strong><br />
Date<br />
03/03/2010 Page 3 of 3