322-0732 TELEMETRY ORDERS rev 09-07
322-0732 TELEMETRY ORDERS rev 09-07
322-0732 TELEMETRY ORDERS rev 09-07
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
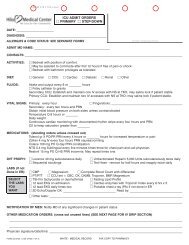
<strong>TELEMETRY</strong><br />
PHYSICIAN <strong>ORDERS</strong><br />
Date: _________________________________<br />
Check the reason(s) you are ordering telemetry.<br />
Arrythmia<br />
Chest pain rule out<br />
Atrial Fibrillation uncontrolled<br />
Mental status changes<br />
Medications that change rhythm<br />
Hypotension<br />
Tachycardia<br />
Electrolyte derangement<br />
Respiratory distress<br />
Other _____________________________________________________________<br />
NOTE: <strong>TELEMETRY</strong> WILL BE AUTOMATICALLY DISCONTINUED IN 72 HOURS UNLESS STIPULATED<br />
OTHERWISE<br />
OTHER: (cross out any unused lines)<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
PHYSICIAN SIGNATURE _____________________________________________ DATE/TIME: ____________________________<br />
FORM <strong>322</strong>-<strong><strong>07</strong>32</strong> 1/<strong>07</strong><br />
White: Chart copy Yellow: Pharmacy copy Pink: CCU copy<br />
<strong>TELEMETRY</strong> <strong>ORDERS</strong>
<strong>TELEMETRY</strong><br />
PHYSICIAN <strong>ORDERS</strong><br />
Date: _________________________________<br />
Check the reason(s) you are ordering telemetry.<br />
Arrythmia<br />
Chest pain rule out<br />
Atrial Fibrillation uncontrolled<br />
Mental status changes<br />
Medications that change rhythm<br />
Hypotension<br />
Tachycardia<br />
Electrolyte derangement<br />
Respiratory distress<br />
Other _____________________________________________________________<br />
NOTE: <strong>TELEMETRY</strong> WILL BE AUTOMATICALLY DISCONTINUED IN 72 HOURS UNLESS STIPULATED<br />
OTHERWISE<br />
OTHER: (cross out any unused lines)<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
PHYSICIAN SIGNATURE _____________________________________________ DATE/TIME: ____________________________<br />
FORM <strong>322</strong>-<strong><strong>07</strong>32</strong> 1/<strong>07</strong><br />
White: Chart copy Yellow: Pharmacy copy Pink: CCU copy<br />
<strong>TELEMETRY</strong> <strong>ORDERS</strong>
<strong>TELEMETRY</strong><br />
PHYSICIAN <strong>ORDERS</strong><br />
Date: _________________________________<br />
Check the reason(s) you are ordering telemetry.<br />
Arrythmia<br />
Chest pain rule out<br />
Atrial Fibrillation uncontrolled<br />
Mental status changes<br />
Medications that change rhythm<br />
Hypotension<br />
Tachycardia<br />
Electrolyte derangement<br />
Respiratory distress<br />
Other _____________________________________________________________<br />
NOTE: <strong>TELEMETRY</strong> WILL BE AUTOMATICALLY DISCONTINUED IN 72 HOURS UNLESS STIPULATED<br />
OTHERWISE<br />
OTHER: (cross out any unused lines)<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
____________________________________________________________________________________________________________<br />
PHYSICIAN SIGNATURE _____________________________________________ DATE/TIME: ____________________________<br />
FORM <strong>322</strong>-<strong><strong>07</strong>32</strong> 1/<strong>07</strong><br />
White: Chart copy Yellow: Pharmacy copy Pink: CCU copy<br />
<strong>TELEMETRY</strong> <strong>ORDERS</strong>