322-0263 RESTRAINT SECFUSION ORDER FORM rev 04-09
322-0263 RESTRAINT SECFUSION ORDER FORM rev 04-09
322-0263 RESTRAINT SECFUSION ORDER FORM rev 04-09

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
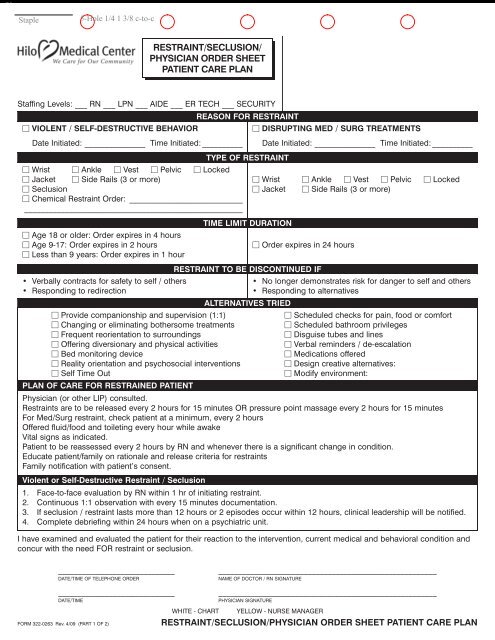
<strong>RESTRAINT</strong>/SECLUSION/<br />
PHYSICIAN <strong>ORDER</strong> SHEET<br />
PATIENT CARE PLAN<br />
Staffing Levels: ___ RN ___ LPN ___ AIDE ___ ER TECH ___ SECURITY<br />
VIOLENT / SELF-DESTRUCTIVE BEHAVIOR<br />
Date Initiated: _______________ Time Initiated: __________<br />
Wrist Ankle Vest Pelvic Locked<br />
Jacket Side Rails (3 or more)<br />
Seclusion<br />
Chemical Restraint Order: ____________________________<br />
______________________________________________________<br />
Age 18 or older: Order expires in 4 hours<br />
Age 9-17: Order expires in 2 hours<br />
Less than 9 years: Order expires in 1 hour<br />
• Verbally contracts for safety to self / others<br />
• Responding to redirection<br />
Provide companionship and supervision (1:1)<br />
Changing or eliminating bothersome treatments<br />
Frequent reorientation to surroundings<br />
Offering diversionary and physical activities<br />
Bed monitoring device<br />
Reality orientation and psychosocial interventions<br />
Self Time Out<br />
PLAN OF CARE FOR RESTRAINED PATIENT<br />
REASON FOR <strong>RESTRAINT</strong><br />
TYPE OF <strong>RESTRAINT</strong><br />
TIME LIMIT DURATION<br />
ALTERNATIVES TRIED<br />
DISRUPTING MED / SURG TREATMENTS<br />
Date Initiated: _______________ Time Initiated: __________<br />
Wrist Ankle Vest Pelvic Locked<br />
Jacket Side Rails (3 or more)<br />
Order expires in 24 hours<br />
<strong>RESTRAINT</strong> TO BE DISCONTINUED IF<br />
• No longer demonstrates risk for danger to self and others<br />
• Responding to alternatives<br />
Scheduled checks for pain, food or comfort<br />
Scheduled bathroom privileges<br />
Disguise tubes and lines<br />
Verbal reminders / de-escalation<br />
Medications offered<br />
Design creative alternatives:<br />
Modify environment:<br />
Physician (or other LIP) consulted.<br />
Restraints are to be released every 2 hours for 15 minutes OR pressure point massage every 2 hours for 15 minutes<br />
For Med/Surg restraint, check patient at a minimum, every 2 hours<br />
Offered fluid/food and toileting every hour while awake<br />
Vital signs as indicated.<br />
Patient to be reassessed every 2 hours by RN and whenever there is a significant change in condition.<br />
Educate patient/family on rationale and release criteria for restraints<br />
Family notification with patient’s consent.<br />
Violent or Self-Destructive Restraint / Seclusion<br />
1. Face-to-face evaluation by RN within 1 hr of initiating restraint.<br />
2. Continuous 1:1 observation with every 15 minutes documentation.<br />
3. If seclusion / restraint lasts more than 12 hours or 2 episodes occur within 12 hours, clinical leadership will be notified.<br />
4. Complete debriefing within 24 hours when on a psychiatric unit.<br />
I have examined and evaluated the patient for their reaction to the intervention, current medical and behavioral condition and<br />
concur with the need FOR restraint or seclusion.<br />
______________________________<br />
DATE/TIME OF TELEPHONE <strong>ORDER</strong><br />
______________________________________________________<br />
NAME OF DOCTOR / RN SIGNATURE<br />
______________________________<br />
______________________________________________________<br />
DATE/TIME<br />
PHYSICIAN SIGNATURE<br />
WHITE - CHART YELLOW - NURSE MANAGER<br />
<strong>FORM</strong> <strong>322</strong>-<strong>0263</strong> Rev. 4/<strong>09</strong> (PART 1 OF 2)<br />
<strong>RESTRAINT</strong>/SECLUSION/PHYSICIAN <strong>ORDER</strong> SHEET PATIENT CARE PLAN
GUIDELINES FOR REDUCTION OF <strong>RESTRAINT</strong>/SECLUSION<br />
ALTERNATIVE INTERVENTIONS<br />
<strong>RESTRAINT</strong>/SECLUSION<br />
INTERVENTIONS<br />
Wandering Mentally Impaired<br />
• Buddy system: family, volunteer, nursing staff.<br />
• Patient alarm device.<br />
• Activate IDT, <strong>rev</strong>iew/modify plan of care.<br />
• Assign diversional activity.<br />
• Safety belt.<br />
• Vest restraint.<br />
• Wrist restraints (only if removing essential, invasive<br />
tubing, IV, etc., or attempting to mutilate self).<br />
• Assess for pain, hunger, thirst, need to use<br />
the bathroom.<br />
• Place near nursing station.<br />
• Offer prn medication, as prescribed.<br />
Unconscious, attempting to remove medical devices.<br />
• Buddy system: family, volunteer.<br />
• Cover invasive tubing, IVs, etc. with gauze.<br />
• Mitt restraint.<br />
• Wrist restraint.<br />
• Sedation as ordered.<br />
Uncontrollable hyper-motor-activity, p<strong>rev</strong>enting implementation of clinical care.<br />
• Temporary holding for completion of procedure.<br />
• Scheduled exercise/toileting/activity.<br />
• Meaning activity, use personal stereo (walkman)<br />
with patient’s favorite music.<br />
• Elbow restraint.<br />
• Mummy restraint.<br />
• Wrist restraint (if causing injury to self).<br />
• Offer prn medication, as prescribed.<br />
• Diversional activity, place soft items in both hands.<br />
Intrusive behavior/physical aggression to self or others.<br />
• Therapeutic conversation.<br />
• Remove excessive stimulation.<br />
• 15 minute self time out.<br />
• Verbal interaction/redirecting.<br />
• Seclusion.<br />
• Wrist restraint.<br />
• Vest restraint.<br />
• Locked restraint.<br />
• PRN medication, as prescribed.<br />
This is not meant to exhaust all possibilities, but to act as a guide for potential behavior problems, alternative<br />
interventions, and appropriate choices of least to most restrictive restraint/seclusion interventions.
<strong>RESTRAINT</strong>/SECLUSION/<br />
PHYSICIAN <strong>ORDER</strong> SHEET<br />
PATIENT CARE PLAN<br />
Staffing Levels: ___ RN ___ LPN ___ AIDE ___ ER TECH ___ SECURITY<br />
VIOLENT / SELF-DESTRUCTIVE BEHAVIOR<br />
Date Initiated: _______________ Time Initiated: __________<br />
Age 18 or older: Order expires in 4 hours<br />
Age 9-17: Order expires in 2 hours<br />
Less than 9 years: Order expires in 1 hour<br />
• Verbally contracts for safety to self / others<br />
• Responding to redirection<br />
<strong>RESTRAINT</strong> REVIEW SECTION<br />
Provide companionship and supervision (1:1)<br />
Changing or eliminating bothersome treatments<br />
Frequent reorientation to surroundings<br />
Offering diversionary and physical activities<br />
Bed monitoring device<br />
Reality orientation and psychosocial interventions<br />
Self Time Out<br />
YES NO<br />
Alternatives Tried / Documented <br />
Patient / Family Educated <br />
Code Grey Required <br />
Patient Injury <br />
Staff Injury <br />
Close Watch Completed <br />
Interdisciplinary Progress Notes<br />
Completed <br />
Restraint Initiated by: ________________________________<br />
Time Removed: _______________ Length (hrs): __________<br />
Review Section completed by: ________________________<br />
REASON FOR <strong>RESTRAINT</strong><br />
TIME LIMIT DURATION<br />
ALTERNATIVES TRIED<br />
DISRUPTING MED / SURG TREATMENTS<br />
Date Initiated: _______________ Time Initiated: __________<br />
TYPE OF <strong>RESTRAINT</strong><br />
Wrist Ankle Vest Pelvic Locked<br />
Jacket Side Rails (3 or more)<br />
Wrist Ankle Vest Pelvic Locked<br />
Seclusion<br />
Jacket Side Rails (3 or more)<br />
Chemical Restraint Order: ____________________________<br />
______________________________________________________<br />
Order expires in 24 hours<br />
<strong>RESTRAINT</strong> TO BE DISCONTINUED IF<br />
• No longer demonstrates risk for danger to self and others<br />
• Responding to alternatives<br />
Scheduled checks for pain, food or comfort<br />
Scheduled bathroom privileges<br />
Disguise tubes and lines<br />
Verbal reminders / de-escalation<br />
Medications offered<br />
Design creative alternatives:<br />
Modify environment:<br />
UNIT ER Laulima Hale Ho‘ola<br />
CCU Medical OB<br />
CV Med/Surg Other ____________<br />
COMPLETE THIS BOX FOR VIOLENT<br />
OR SELF-DESTRUCTIVE BEHAVIOR YES NO<br />
1 hr face-to-face assessment by LP or RN <br />
Staff participating documented in <br />
Medical Record<br />
Debriefing documentation complete <br />
(Behavioral Health department only)<br />
Clinical leadership notified if >12 hrs <br />
OR 2 episodes within 12 hrs<br />
I have examined and evaluated the patient for their reaction to the intervention, current medical and behavioral condition and<br />
concur with the need FOR restraint or seclusion.<br />
______________________________<br />
DATE/TIME OF TELEPHONE <strong>ORDER</strong><br />
______________________________________________________<br />
NAME OF DOCTOR / RN SIGNATURE<br />
______________________________<br />
______________________________________________________<br />
DATE/TIME<br />
PHYSICIAN SIGNATURE<br />
WHITE - CHART YELLOW - NURSE MANAGER<br />
<strong>FORM</strong> <strong>322</strong>-<strong>0263</strong> Rev. 4/<strong>09</strong> (PART 1 OF 2)<br />
<strong>RESTRAINT</strong>/SECLUSION/PHYSICIAN <strong>ORDER</strong> SHEET PATIENT CARE PLAN
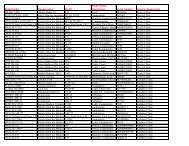
<strong>FORM</strong> <strong>322</strong>-<strong>0263</strong> Rev. 4/<strong>09</strong> (PART 2 OF 2)<br />
VIOLENT OR SELF<br />
DESTRUCTIVE BEHAVIOR<br />
CLOSE WATCH<br />
List of participants in this episode were:<br />
________________________________________________________________<br />
Restraint Order: Wrist Ankle Vest Pelvic Jacket Siderails (3 or more) Locked<br />
Restraint Code: A = restraint applied B = restraint released Family notified Yes No Declines Unable to reach<br />
Date Initiated _______________ Time initiated ____________ Initiated by: ____________________________________<br />
Time / Code<br />
Initials Time / Code<br />
Initials Time / Code<br />
Initials Nursing Assessment/Intervention Codes<br />
0015<br />
0815<br />
1615<br />
C= One hour RN face to face assessment<br />
0030<br />
0830<br />
1630<br />
D= Assessment by RN for physical and<br />
0<strong>04</strong>5<br />
0845<br />
1645<br />
psychological status and comfort. Determine<br />
readiness for discontinuation of restraints.<br />
0100<br />
<strong>09</strong>00<br />
1700<br />
E= Education provided to patient/family on<br />
0115<br />
<strong>09</strong>15<br />
1715<br />
rationale for restraint and release criteria<br />
0130<br />
0145<br />
0200<br />
<strong>09</strong>30<br />
<strong>09</strong>45<br />
1000<br />
1730<br />
1745<br />
1800<br />
F= Circulation check to restrained limbs<br />
G= Continuous 1:1 (in person) monitoring with<br />
15 minute assessment<br />
0215<br />
1015<br />
1815<br />
H= Restraints released for range of motion<br />
every 2 hours for 15 minutes OR Position<br />
0230<br />
1030<br />
1830<br />
change/pressure point massage every 2 hours<br />
0245<br />
1<strong>04</strong>5<br />
1845<br />
for 15 minutes<br />
0300<br />
1100<br />
1900<br />
I= Offered Fluid and Toileting every hour while<br />
awake<br />
0315<br />
1115<br />
1915<br />
J= High risk medical conditions identified<br />
0330<br />
1130<br />
1930<br />
K= History of sexual abuse identified<br />
0345<br />
1145<br />
1945<br />
L= Refer to Interdisciplinary progress record for<br />
<strong>04</strong>00<br />
1200<br />
2000<br />
details<br />
<strong>04</strong>15<br />
<strong>04</strong>30<br />
<strong>04</strong>45<br />
0500<br />
0515<br />
0530<br />
1215<br />
1230<br />
1245<br />
1300<br />
1315<br />
1330<br />
2015<br />
2030<br />
2<strong>04</strong>5<br />
2100<br />
2115<br />
2130<br />
Patient Behavior Codes<br />
1= Severely aggressive behavior which is a<br />
danger to others<br />
2= Severely aggressive behavior which is a<br />
danger to self<br />
3= Patient appears asleep at this time<br />
4= Patient meets criteria for release at this time<br />
0545<br />
0600<br />
0615<br />
0630<br />
0645<br />
0700<br />
0715<br />
0730<br />
0745<br />
0800<br />
1345<br />
1400<br />
1415<br />
1430<br />
1445<br />
1500<br />
1515<br />
1530<br />
1545<br />
1600<br />
2145<br />
2200<br />
2215<br />
2230<br />
2245<br />
2300<br />
2315<br />
2330<br />
2345<br />
2400<br />
Initials<br />
Signature / Title<br />
WHITE - PERMANENT MEDICAL RECORD
Patient Debriefing Process / documentation<br />
Debriefing after seclusion/restraint is important in reducing the recurrent use of seclusion/restraint. The patient and<br />
a family member with consent participate with the staff involved in the episode (Excluding staff which may<br />
jeopardize the well-being of the patient). This should occur as soon as possible but no longer than 24 hours after<br />
the episode.<br />
Document below what was identified in the session:<br />
What led to the incident ________________________________________________________________________________<br />
______________________________________________________________________________________________________<br />
______________________________________________________________________________________________________<br />
What alternatives were tried that failed____________________________________________________________________<br />
______________________________________________________________________________________________________<br />
______________________________________________________________________________________________________<br />
Were the patient’s physical well being, psychological comfort and privacy addressed Yes _________ No ________<br />
Explain:________________________________________________________________________________________________<br />
What could have been handled differently ________________________________________________________________<br />
______________________________________________________________________________________________________<br />
If indicated counsel patient for any trauma than may have resulted from episode. Yes __________ No __________<br />
__________________________________________________________________________________________________________________<br />
If indicated how is the treatment plan being modified ______________________________________________________<br />
______________________________________________________________________________________________________<br />
______________________________________________________________________________________________________<br />
List Participants: ________________________________________________________________________________________<br />
______________________________________________________________________________________________________<br />
Date and time of debriefing: _________________________________________ Document additional information in the<br />
interdisciplinary notes.<br />
__________________________________________________________________________________________________________________