NH State Accident Report (pdf) - Town Of Atkinson
NH State Accident Report (pdf) - Town Of Atkinson
NH State Accident Report (pdf) - Town Of Atkinson

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
~<br />
8. ,~I<br />
single line UtIlIze a further report form If more than SIX persons .<br />
l~ WHICH VEHICLE<br />
OCCUPIED<br />
Y our vehicles owner's CURRENT name be signed and dated, else the repo t cannot be accepted.<br />
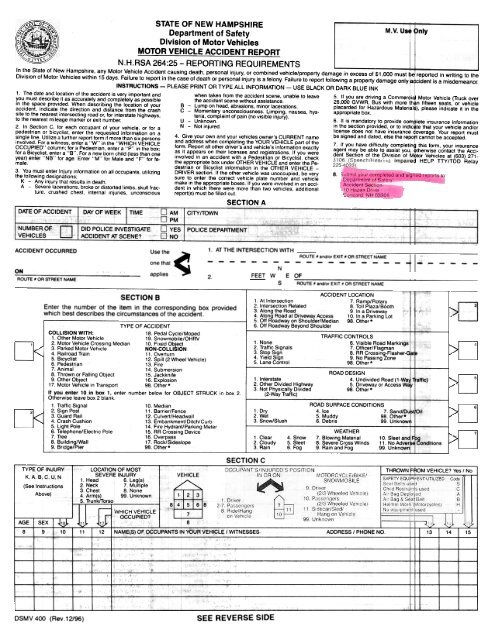
STATE OF NEW HAMPSHIRE<br />
Department of Safety<br />
Division of Motor Vehicles<br />
MOTOR VEHICLE ACCIDENT REPORT<br />
N.H.RSA 264:25 -REPORTING<br />
REQUIREMENTS<br />
M.V. Use Only<br />
In the <strong>State</strong> of New Hampshire, any Motor Vehicle <strong>Accident</strong> causing death, personal injury, or combined vehicle/property damage in excess of $1,000 must ~e reported in writing to the<br />
Division of Motor Vehicles within 15 days. Failure to report in the case of death or personal injury is a felony. Failure to report following a property damage only ~ cident is a misdemeanor.<br />
INSTRUCTIONS -PLEASE PRINT OR TYPE ALL INFORMATION -USE BLACK OR DARK BLUE INK<br />
1. The date and lo~ation of the accident is very important and when t~ken from the accident scene, unable to leave<br />
I<br />
5. If you are driving a Commer4i Motor Vehicle (Truck over<br />
you must describe It as accurately and completely as possible the accident scene wIthout assIstance. 26000 GVWR Bus with more jh n fifteen seats or vehicle<br />
in the space provided. Whe!1 describing the location of your B -Lump on head, abrasions, minor lacerations. placarded for Hazardous Material ), please indicate it in the<br />
accident, Indicate the direction and distance from the crash C -Momentary unconsciousness. Limping, nausea, hys- appropriate box.<br />
site to the nearest Intersecting road or, for interstate highways,<br />
teria, complaint of pain (no visible injury).<br />
to the nearest mileage marker or exit number. U -Unknown. 6. It IS mandatory to provide com lete Insurance Information<br />
2. In Section C, for each occupant of your vehlclll, or for a N -Not injured. in license the section does provided, not have insurance or to indlc overage te that your Your vehicle report and/or must<br />
pedestrian or biCycliSt, enter the requested InformatIon on a 4 Give your own and<br />
involved. For a witness, enter a "W" in the "WHICH VEHICLE and address when com~letl,ng the YOUR,VEHICLEpart of the 7. If you have difficulty completln this form, your insurance<br />
OCCUPIED" column; for a Pedestrian, enter a "P" in the box; form. <strong>Report</strong> all other drIver s and vehicle s In,formatlon exactly agent may be able to assist you, therwise contact the AcCifor<br />
a Bicyclist, enter a "B". For a new born child (less than one as It appears on their licenses and re~lstratlons. If you were dent Section of the Division of M tor Vehicles at (603) 271-<br />
year) enter "NB" for age Enter "M" for Male and "F" for fe- Involved In an accIdent with a Pedestrian or BICycliSt, check Impaire HELP TTY/TDD Relay<br />
male<br />
the appropriate box under OTHER VEHICLE and enter the Pe.<br />
3. You must enter Injury information on all occupants, utilizing<br />
destrian or Bicyclist information in the OTHER VEHICLE -<br />
DRIVER section. If the other vehicle was unoccupied, be very<br />
the following designations;<br />
sure to enter the correct vehicle plate number and vehicle<br />
K -Any injury that results in death make in the appropriate boxes. If you were involved in an acci.<br />
A -Severe lacerations, broke or distorted limbs, skull frac. dent in which there were more than two vehicles, additional<br />
ture. crushed chest, internal injuries, unconscious report(s) must be filled out<br />
SECTION A<br />
ACCIDENT OCCURRED<br />
ON<br />
ROUTE * OR STREET NAME<br />
Use the<br />
one that<br />
applies<br />
1. AT THE INTERSECTION WITH<br />
2.<br />
FEET W E OF<br />
N -_RO~E#.:nd/:EX~O~ST~ET~AM:- -i I~-<br />
s ROUTE 1/ and/or EXIT 1/ OR STREET NAME<br />
SECTION B<br />
Enter the number of the item in the corresponding box provided<br />
which best describes the circumstances of the accident.<br />
TYPE OF ACCIDENT<br />
COLLISION WITH:<br />
18 Pedal Cycle/Moped<br />
1 Other Motor Vehicle 19 Snowmobile/OHRV<br />
2 Motor Vehicle Crossing Median 10 Fixed Object<br />
3 Parked Motor Vehicle NON-COLLISION<br />
4 Railroad Train 11 Overturn<br />
5. Bicyclist 12 Spill (2 Wheel Vehicle)<br />
6 Pedestrian 13. Fire<br />
7. Animal 14. Submersion<br />
8. Thrown or Falling Object 15. Jackknife<br />
9 Other Object 16. Explosion<br />
17 Motor Vehicle in Transport 98. Other.<br />
If you enter 10 in box 1, enter number below for OBJECT STRUCK in box 2<br />
Otherwise leave box 2 blank<br />
1 Traffic Signal 10 Median<br />
2 Sign Post 11 Barrier/Fence<br />
3 Guard Rail 12. Culvert/Headwall<br />
4 Crash Cushion 13. Embankment/Ditch/Curb<br />
5 Light Pole 14. Fire Hydrant/Parking Meter<br />
6. Telephone/Electric Pole 15.RR Crossing Device<br />
7. Tree 16 Overpass<br />
8 Building/Wall 17. Rock/Sidesiope<br />
9. Bridge/Pier 98. Other.<br />
ACCIDENT LOCATION<br />
1 At Intersection 7. Ramp/Rotary<br />
2 Intersection Related 8. Toll Plaza/Booth<br />
3. Along the Road 9 In a Driveway<br />
4 Along Road at Driveway Access<br />
5 <strong>Of</strong>f Roadway on Shoulder/Median<br />
10 In a Parking Lot<br />
98. Other *<br />
6. <strong>Of</strong>f Roadway Beyond Shoulder<br />
1 None<br />
2. Traffic Signals<br />
3 Stop Sign<br />
4. Yield Sign<br />
5 Lane Control<br />
1 Dry<br />
2 Wet<br />
3. Snow/Slush<br />
1 Clear<br />
2 Cloudy<br />
3 Rain<br />
4 Snow<br />
5 Sleet<br />
6 Fog<br />
TRAFFIC CONTROLS<br />
I<br />
6. VIsible Road Markings t<br />
7 <strong>Of</strong>ficer/Flagman<br />
8 RR Crossing-Flasher-~<br />
9. No Passing Zone I<br />
98 Other.<br />
ROAD DESIGN<br />
4 Undivided Road (1.Wav -1alfic)<br />
5 Driveway or Access WiJ!J<br />
98 Other.<br />
ROAD SURFACE CONDITIONS<br />
4 Ice 7 Sand/Dtf 1 Oil<br />
5 Muddy 98 Other.<br />
6. Debris 99 Unknowrj<br />
WEATHER<br />
7 Blowing Material<br />
8. Severe Cross Winds<br />
9 Rain and Fog<br />
10 Sleet and fig<br />
11 No AdverB Conditions<br />
99 Unknown<br />
"<br />
TYPE OF INJURY<br />
K. A. B. C. U, N<br />
(See Instruc!ions<br />
Above)<br />
LOCATION OF MOST<br />
SEVERE INJURY<br />
1 Head 6 Leg(s)<br />
2 Neck 7 Multiple<br />
3 Chest 8. None<br />
4 Arm(s) 99. Unknown<br />
5. TrunklTorso<br />
SECTION C<br />
I THROWN F*OM-V-EHICLE Yes I No I<br />
AGE SEX I ~10.1. ~1'><br />
12 8<br />
8 9 10 11 '2 I NAME(S) OF OCCUPANTS IN YOUR VEHICLE I WITNESSES ADDRESS I PHONE NO 13 14 15<br />
DSMV 400 (Rev.12/96)<br />
SEE REVERSE SIDE
! I. I<br />
Light<br />
Truck<br />
.Wlthout DESCRIPTION OF ACCIDENT, ESTIMATE OF REPAIR, or OPERATOR'S SIGNATURE, report willi NOT be 8CCJPted,<br />
SECTION D , I<br />
YOUR VEI:IICLE<br />
OTHER VEHICLE<br />
DRIVER LICENSE NO STATE CLASSIFICATION DRIVER LICENSE NO STATE<br />
N<br />
DRIVER'S NAME LAST, FIRST. MIDDLE DRIVER'S NAME LAST. FIRST. MIDDLE<br />
D.C.B,<br />
SEX D.C.B. SEX<br />
I CURRENT ADDRESS.<br />
NUMBER AND<br />
-<br />
STREET<br />
PHONE NO.<br />
CURRENT ADDRESS, NUMBER AND STREET PHONE NO<br />
CITY/mWN STATE ZIP CODE<br />
CITv-/fuWN<br />
STATE<br />
ZIP CODE<br />
PLATE NO STATE TRAILER PLATE NO. STATE PLATE NO. STATE TRAILER PLATE N~.<br />
STATE<br />
I SAME<br />
~~IVER D<br />
OWNER NAME LAST. FIRST, MIDDLE I SAME OWNER NAME LAST, FIRST, ~IDDLE<br />
~~IVER 0<br />
CURRENT ADDRESS, NUMBER AND STREET PHONE NO CURRENT ADDRESS, NUMBER AND STREET PHONE NO.<br />
CITY/TOWN STATE ZIP CODE CITY/TOWN STATE ZIP CODE<br />
MAKE YEAR I COMMERCIAL<br />
MAKE YEAi'f1 VEHICLE COMMERCIAL<br />
V.I.N<br />
VEHICLE<br />
ACCIDENT<br />
0<br />
V.I.N.<br />
ACCIDENT<br />
VEHICLE<br />
TOWED<br />
BY<br />
TO<br />
VEHICLE<br />
D<br />
TOWED 0<br />
DESCRIBE DAMAGE TO VEHICLE DESCRIBE DAMAGE TO VEHICLE<br />
BY<br />
TO<br />
"ESTIMATED COST TO REPAIR *ESTIMiI;f'EDCO~ TO REPAIR<br />
YOUR INSURANCE CO<br />
SECTION E<br />
ESTIMATED PROPERTY DAMAGE (OTHER THAN VEHICLE)<br />
AGENT<br />
IDENTIFY DAMAGED PROPERTY OTHER THAN VEHICLE(S)<br />
ADDRESS<br />
POLICY NUMBER<br />
EFFECTIVE DATE<br />
ACCIDENT DIAGRAM<br />
SECTION F<br />
Check one of the diagrams if it adequately describes the accident. OR draw your own diagram<br />
VEHICLE TYPE<br />
on a separate sheet and attach. Number the vehicles. with your vehicle being No.1. 1 Automobile 9. Moped<br />
13. Other/unkn9 n<br />
2. Pick-Up/Light Truck 10. Motor Home<br />
Rear Passin .At. Turn I At. Turn Head On Sideswipe<br />
3. Panel/Van 11 Passenger Light Van 97. Motor Carrier<br />
B. Motorcycle 12 Utility Vehicle (4X4) 98. Other..<br />
-!> -!> -!><br />
.DESCRIBE<br />
1 2<br />
THE<br />
1. North<br />
2. East<br />
VEHICLE DIRECTION<br />
3. South<br />
4. West<br />
99. Unknown<br />
YOUR<br />
Vehicle<br />
Other<br />
Vehicle<br />
YOUR<br />
Vehicle<br />
Other<br />
Vehicle<br />
PRE-ACCIDENT ACTIO~j<br />
'OPERATOR'S SIGNATURE<br />
DATE/OF REjORT<br />
DAY MON YEAR<br />
VEHICLE:<br />
18. Avoid Something in Road<br />
(Box 20 and/or 21)<br />
19. Wrong Way on a 1-Way<br />
1. Following Roadway 97. OTHER Action in Road<br />
2. Right Turn on Red (Box 21 only)<br />
3. Making Right Turn 41. Crossing with Signal<br />
4 Making Left Turn 42. Crossing ag,!inst Signal<br />
5. Making U. Turn 43. Crossing at '::rosswalk No Signal<br />
6 Starting From Parked 44. Crossing No Signal/Crosswall<<br />
7 Starting in Traffic 45. Walk/Ride ,,'ith Traffic<br />
8. Slowing or Stopping 46. Walk/Ride against Traffic<br />
9. Stopped in Traffic 47. Emerge from Front/Rear of<br />
10. Entering Park Position Parked Vehicle<br />
11. Parked Properly 48. Get On/<strong>Of</strong>f !;Chool Bus<br />
12. Parked and Rolled 49. Get On/<strong>Of</strong>f '/ehicle<br />
13. Changing Lanes/Merging 50. Pushing/Working on Vehic.<br />
14. Overtaking/Passing 51. Playing/Jog'9ing<br />
15. Passing on Right 52. Standing/W,!lking<br />
16. Backing 98. OTHER Pedestrian/Bicycli"<br />
17. Parked Improperly Action<br />
YOUR<br />
Vehicle<br />
Other<br />
ve~~cle I<br />
Ped/Blke<br />
~ILJ~.