New Privilege List - DI / Radiation Oncology - Sutter Medical Center
New Privilege List - DI / Radiation Oncology - Sutter Medical Center
New Privilege List - DI / Radiation Oncology - Sutter Medical Center

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
CRITERIA FOR DELINEATION OF PRIVILEGES<br />
<strong>Privilege</strong>s in the Department of <strong>DI</strong>RO (Diagnostic Imaging and <strong>Radiation</strong> <strong>Oncology</strong>) will be applied for by individual physicians (who are members of the <strong>Medical</strong> Staff of <strong>Sutter</strong><br />
<strong>Medical</strong> <strong>Center</strong>) using the attached form. The Administrative Committee of the Department (Chief, Immediate Past Chief, Vice Chief, Secretary and Chair of the Informal Sections<br />
of Diagnostic Radiology, Interventional Radiology, Nuclear Medicine and <strong>Radiation</strong> <strong>Oncology</strong>) will review the application and where indicated meet with the applicant personally<br />
to prepare recommendations for granting of privileges to the Credentials Committee of the <strong>Medical</strong> Staff.<br />
Physicians will submit documentation (when requested by the <strong>DI</strong>RO Administrative Committee) of their training, experience and evidence of Continuing <strong>Medical</strong> Education in<br />
those procedures for which they desire privileges. The basic criteria for department membership and delineation of privileges in Diagnostic Imaging and <strong>Radiation</strong> <strong>Oncology</strong> will<br />
be certification by the American Board of Radiology or the American Board of Nuclear Medicine, physicians who have completed an approved Radiology or Nuclear Medicine<br />
residency, or physicians with previous 10 years experience in a Joint Commission accredited hospital and have exercised similar privileges to those being requested.<br />
Within each general section, the procedures which are generally accepted as lying within the discipline will be included in the privileges. For example, General Diagnostic<br />
Radiology will include injection of contrast material, fluoroscopy, interpretation of radiographs, bronchography, CT and ultrasound under fluoroscopic control, etc. <strong>Radiation</strong><br />
<strong>Oncology</strong> will include those procedures related to application of external irradiation, interstitial or intracavitary sealed radioactive sources, therapeutic use of radioactive isotopes,<br />
etc. Nuclear Medicine will include injections of radionuclides for diagnostic or therapeutic purposes, interpretation of physiologic and anatomic radionuclide studies, in-vitro tests<br />
using radionuclides, and use of monoclonal antibodies for diagnosis and/or treatment. Non-Invasive Vascular Imaging will also be part of Nuclear Medicine.<br />
The subspecialty practices of Angiography, Ultrasonography, Non-Invasive Vascular Imaging, Neuroradiology and Interventional Radiology will be considered for granting of<br />
privileges when these disciplines are included in the residency training and examination. Where these skills are acquired after residency training, consideration for delineation will<br />
be on an individual basis and take into account current and recent practice, post-graduate courses, preceptor training, or other forms of additional post-graduate training, and may<br />
require prior performance of an acceptable number of procedures. <strong>Privilege</strong>s for General Diagnostic Imaging, Interventional Radiology, Neuroradiology and Interventional<br />
Neuroradiology require a Radiography Supervisor and Operator Permit.<br />
Consideration of granting of privileges to radiologists and non-radiologists must clearly reflect the major difference between specialists of various disciplines in view of the<br />
former’s knowledge of all available imaging modalities. Training and background will be primary criteria for delineation of privileges for any physician. The quality of training, as<br />
well as its duration, will necessarily continue to be a primary prerequisite in the privileging process.<br />
<strong>Privilege</strong>s are granted for <strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento and exercise of privileges is based on the type of care, treatment and services provided at each facility.<br />
<strong>Privilege</strong>s are granted for <strong>Sutter</strong> General Hospital, <strong>Sutter</strong> Memorial Hospital, <strong>Sutter</strong> <strong>Center</strong> for Psychiatry, Capital Pavilion Surgery <strong>Center</strong>, or <strong>Sutter</strong> Oaks Midtown<br />
and exercise of privileges is based on the type of care, treatment and services provided at each facility<br />
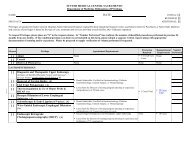
To request <strong>Privilege</strong>s, please place an “X” in the request column. In “Number Performed” box, indicate the number of identified procedures performed in previous 24<br />
months from any facility. If the condition/privilege you desire is not included on this form, please submit a separate written request along with appropriate<br />
documentation of training and/or experience. Please be prepared to supply verification of volume performance if requested.<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
Reappointment Number<br />
Requirements Performed<br />
[ ] Admitting <strong>Privilege</strong> NONE None None N/A<br />
[ ] H&P <strong>Privilege</strong><br />
Page 1 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
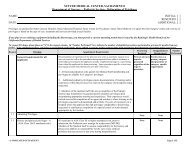
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
[ ] I. GENERAL <strong>DI</strong>AGNOSTIC IMAGING<br />
All aspects of patient management, exclusive of those<br />
listed below, which are within the generally recognized<br />
scope of Radiological practice.<br />
[ ] Stereotactic Breast Biopsy<br />
Stereotactic localization of breast lesions involves the<br />
use of dedicated radiographic equipment for targeting<br />
radiopaque breast lesions for subsequent biopsy.<br />
Stereotactic core needle type biopsy involves the use of<br />
the same radiographic equipment for localizing and<br />
subsequently performing percutaneous core needle type<br />
biopsy of breast lesions.<br />
Radiology Certificate Required<br />
Basic understanding of radiographic equipment and<br />
interpretation of mammographic abnormalities should be<br />
documented by certification of the American Board of<br />
Radiology and American College of Radiology,<br />
respectively. Physicians should meet the qualifications<br />
from the ACR standards for screening mammography<br />
and diagnostic mammography and problem solving<br />
breast evaluation and attest they meet Mammography<br />
Quality Standards Act (MQSA) standards.<br />
1. Specific experience and/or training may be<br />
documented by either of the following means:<br />
a. satisfactory completion of an accredited<br />
residency program which includes a minimum<br />
of twenty-five (25) stereotactic breast biopsy<br />
procedures;– OR –<br />
b. post graduate applicant should demonstrate<br />
competency by:<br />
1. Documentation of thirty (30) stereotactic<br />
localization and/or breast biopsy<br />
procedures with appropriate follow up<br />
documentation,<br />
– OR –<br />
2. Documentation of involvement in twenty-five (25)<br />
stereotactic localization and/or breast biopsy<br />
procedures under the supervision of a qualified<br />
physician preceptor and three hours of Category I<br />
CME didactic instruction in stereotactic biopsy.<br />
First five (5) cases<br />
AND<br />
Evaluations at 3, 6 &<br />
12 Months.<br />
NONE<br />
Reappointment<br />
Requirements<br />
None<br />
Minimum of<br />
twenty-five (25)<br />
cases in a two year<br />
period.<br />
Number<br />
Performed<br />
N/A<br />
(Continued on next page)<br />
• At least one half of these cases must be<br />
performed at the equivalent level of the<br />
primary operator.<br />
Page 2 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
[ ] Stereotactic Breast Biopsy - Continued • The five (5) cases should be performed within<br />
the previous one year at the time of application<br />
for privileges.<br />
• A letter of verification from the applicants<br />
primary tutor who has performed at least five<br />
(5) cases with the applicant stating that the<br />
applicant is qualified to perform this procedure<br />
as a primary operator.<br />
Reappointment<br />
Requirements<br />
Number<br />
Performed<br />
[ ] Magnetic Resonance Imaging NONE NONE N/A<br />
[ ] Coronary CT Angiography<br />
Coronary CTA is a heart-imaging test using computed<br />
tomography (CT) to image the coronary arteries, cardiac<br />
chambers, valves, myocardium and pericardium and can<br />
help assess cardiac function<br />
(Continued on next page)<br />
Prerequisite: Must currently hold General Diagnostic First three (3) cases.<br />
Imaging privileges<br />
1. Certification in radiology or diagnostic radiology by<br />
the American Board of Radiology, the American<br />
Osteopathic Board of Radiology, the Royal College<br />
of Physicians and Surgeons of Canada, or Le<br />
College des Medecins du Quebec and have<br />
completed 50 supervised interpretations of cardiac<br />
CT exams, excluding those performed exclusively<br />
for calcium scoring, in the past 36 months.<br />
Documentation of cases should be by case listing or<br />
a letter from the Chief of Staff or <strong>Medical</strong> Director<br />
of a Joint Commission accredited hospital where the<br />
cases were performed attesting to the number of<br />
cases.<br />
OR,<br />
2. Competed an Accreditation Council for Graduate<br />
<strong>Medical</strong> Education (ACGME)-approved radiology<br />
residency program and have completed 50<br />
supervised interpretations of cardiac CT exams,<br />
excluding those performed exclusively for calcium<br />
scoring, in the past 36 months. Documentation of<br />
cases should be by a letter from the director of the<br />
residency program attesting to the physician’s<br />
competence to perform the procedure and volume<br />
of cases.<br />
AND,<br />
Minimum of Fifty<br />
(50) cases in a two<br />
year period.<br />
Page 3 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
Coronary CT Angiography – Continued<br />
3. Completed at least 40 hours of category I continuing<br />
medical education (CME) in cardiac imaging,<br />
including cardiac CT/coronary CTA anatomy,<br />
physiology, and/or pathology or documented<br />
equivalent supervised experience in a center actively<br />
performing coronary CTA. Documentation of<br />
CME can be by copies of certificates or listing of<br />
CME programs with date, title of program and<br />
number Category 1 CME credits granted.<br />
Reappointment<br />
Requirements<br />
Number<br />
Performed<br />
[ ] II. INTERVENTIONAL RA<strong>DI</strong>OLOGY Radiography Certificate Required. First five (5) cases<br />
AND<br />
Evaluations at 3, 6 &<br />
12 Months<br />
[ ] Central venous catheter placement with<br />
subcutaneous tunnel<br />
[ ] Central venous catheter placement without<br />
subcutaneous tunnel<br />
[ ] Transvenous repositioning a central venous catheter<br />
[ ] Transvenous extraction of central venous catheter<br />
fragment<br />
[ ] Central venous catheter placement with<br />
subcutaneous port<br />
[ ] Removal of central venous catheter either tunneled<br />
or with subcutaneous port<br />
[ ] Exchange of central venous catheter either tunneled<br />
or non-tunneled<br />
[ ] Transvenous stripping of central venous catheter<br />
[ ] Thrombolytic infusion for non-functioning central<br />
venous catheter<br />
[ ] Thrombolytic infusion for deep venous thrombosis<br />
[ ] Venous angioplasty<br />
[ ] Parathyroid and thyroid venous sampling<br />
[ ] Renal venous sampling<br />
[ ] Adrenal venous sampling<br />
[ ] Visceral venous sampling<br />
[ ] Wedge hepatic venogram<br />
[ ] Wedge hepatic venous pressure measurement<br />
[ ] Trans splenic portal venogram<br />
Page 4 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
[ ] Transhepatic portal venogram<br />
[ ] Venous angioplasty with stenting<br />
[ ] Uterine vein embolizations<br />
[ ] Gonadal vein embolizations<br />
[ ] Percutaneous occlusion of splenic artery for<br />
[ ]<br />
hypersplenism<br />
Bronchial artery embolization for hemostatis or<br />
tumor<br />
[ ] Venous embolization for venous malformation<br />
[ ] Venous ethanol injection for venous malformation<br />
[ ] Angioplasty and stenting transhepatic portosystemic<br />
shunt<br />
[ ] Embolization esophageal and gastric varices<br />
[ ] Percutaneous transhepatic cholangiogram<br />
[ ] Percutaneous biliary drainage<br />
[ ] Percutaneous transhepatic internal/external biliary<br />
drainage<br />
[ ] Percutaneous transhepatic biliary drainage with<br />
stent placement<br />
[ ] Percutaneous transhepatic extraction of biliary duct<br />
stones<br />
[ ] Percutaneous cholecystostomy<br />
[ ] Percutaneous dilatation of biliary stricture<br />
[ ] Percutaneous trans T-tube extraction of biliary stone<br />
[ ] Percutaneous nephrostomy<br />
[ ] Percutaneous nephrostomy for access prior to<br />
nephrolithotomy<br />
[ ] Nephrostomy tube change<br />
[ ] Antigrade ureteral stenting<br />
[ ] Whitaker exam renal collecting system with<br />
manometry<br />
[ ] Percutaneous Gastrostomy<br />
[ ] Percutaneous jejunostomy<br />
[ ] Percutaneous dilatation of enteric obstructions,<br />
plus/minus stenting<br />
[ ] Conversion of gastrostomy to gastrojejunostomy<br />
[ ] Fallopian tube dilatation<br />
Reappointment<br />
Requirements<br />
Number<br />
Performed<br />
Page 5 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
[ ] Ultrasound guided thoracentesis<br />
[ ] Ultrasound guided Paracentesis<br />
[ ] CT guided thoracentesis<br />
[ ] CT guided Paracentesis<br />
[ ] CT, ultrasound or fluoroscopic guided placement to<br />
thoracostomy tube<br />
[ ] Ultrasound, CT or fluoroscopic guided drainage of<br />
abscess (lung, pancreatic, subdiaphragmatic,<br />
retroperitoneal, renal, perirenal and pelvic)<br />
[ ] Ultrasound, CT or fluoroscopic guided drainage of<br />
hepatic, renal or pancreatic cyst<br />
[ ] Ultrasound, fluoroscopic of CT guided sclerosis of<br />
hepatic, pancreatic or renal cyst<br />
[ ] Percutaneous drainage of pancreatic pseudocyst<br />
[ ] Percutaneous creation of pancreatic-gastric cyst<br />
Gastrostomy<br />
[ ] Transrectal or transvaginal drainage of pelvic<br />
abscess<br />
[ ] CT, ultrasound or fluoroscopic guided biopsy<br />
(thyroid, lung, liver, pancreatic, retroperitoneal,<br />
intraperitoneal, muscle, bone, lymphoid, breast and<br />
prostate)<br />
[ ] Transjugular liver biopsy<br />
[ ] Percutaneous placement of inferior cava filter<br />
[ ] Percutaneous retrieval of intravascular foreign body<br />
[ ] Vascular embolization for bleeding<br />
[ ] Vascular embolization for arterial venous<br />
malformation<br />
[ ] Vascular embolization for tumor<br />
[ ] Chemo embolization for tumor<br />
[ ] Visceral arterial infusion for ischemia<br />
[ ] Percutaneous fluoroscopic declotting of thrombosed<br />
arterial venous grafts or shunts created for dialysis<br />
using either balloon fogarty or non-balloon<br />
(thrombolytic) technique<br />
[ ] Percutaneous ethanol ablation of tumors<br />
[ ] Transluminal occlusion of ureter<br />
[ ] Ureteral angioplasty for strictures<br />
Reappointment<br />
Requirements<br />
Page 6 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.<br />
Number<br />
Performed
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
[ ] Percutaneous drainage of lymphocele<br />
[ ] Percutaneous celiac plexus blockade or ablation<br />
[ ] Percutaneous CT guided lumbar sympatholysis<br />
[ ] Percutaneous thrombectomy of pulmonary artery<br />
embolism<br />
[ ] Catheter directed intraarterial thrombolysis<br />
[ ] Catheter directed intravenous thrombolysis<br />
[ ] Peripheral Transluminal Angioplasty<br />
Peripheral angioplasty (PTA) is the percutaneous<br />
approach toArteriograph intervention by dilatation or<br />
atherectomy and may include stent placement. A<br />
diagnostic peripheral angiogram is any non-coronary<br />
or non-cerebral (intra/extra cranial) angiogram and is<br />
one that provides complete imaging of the entire<br />
vascular distribution and the runoff of the vessel(s) in<br />
question.<br />
(This privilege is shared with another department)<br />
(Continued on next page)<br />
Disciplines of Vascular Surgery, Radiology and<br />
Cardiology are eligible for credentialing.<br />
• Basic understanding of cardiovascular disease<br />
should be documented by eligibility or certification<br />
by any one of the following:<br />
• American Board of Radiology<br />
• American Board of Internal Medicine with special<br />
certification in Cardiovascular Medicine fellowship<br />
• American Board of Surgery with completion of a<br />
general vascular surgery one (1) year fellowship<br />
• Physicians seeking to qualify by having completed<br />
a training program shall have documentation of<br />
having performed 100 peripheral angiograms, 50<br />
peripheral interventional procedures (counted per<br />
lesion) within the past three years and shall have a<br />
letter from the Chief of his/her training program<br />
stating that the applicant is competent to perform<br />
peripheral vascular interventions as a primary<br />
operator.<br />
– OR –<br />
Documentation of having performed 100 peripheral<br />
angiograms, 50 peripheral angioplasties within the<br />
past three years at another Joint Commission<br />
accredited hospital and documentation of attendance<br />
at a dedicated symposium on PTA, which has live<br />
case demonstrations, shall be documented.<br />
– OR –<br />
Documentation of successful completion of an<br />
approved in-house learning program under the<br />
First Five (5)<br />
Interventional<br />
procedures<br />
Reappointment<br />
Requirements<br />
Minimum of 50<br />
therapeutic<br />
interventions<br />
(counted per<br />
patient) in a twoyear<br />
period Should<br />
an applicant not<br />
attain the suggested<br />
number of<br />
procedures<br />
proctoring may be<br />
initiated as<br />
determined by the<br />
Department<br />
Q.I./Administrative<br />
Committee.<br />
Page 7 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.<br />
Number<br />
Performed
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
Peripheral Transluminal Angioplasty - Continued<br />
[ ] Hepatic Artery Chemoembolization<br />
Sub-selective catheterization of the hepatic artery, or<br />
its branches, with subsequent infusion of<br />
chemotherapeutic agents and/or embolic agents (under<br />
fluoroscopic guidance) with immediate removal of the<br />
catheter after the procedure has been performed.<br />
[ ] Peripheral and Visceral Arteriography (noncoronary/non-cerebral<br />
diagnostic angiography)<br />
(This privilege is shared with another department)<br />
(Continued on next page)<br />
preceptorship of a senior qualified physician and<br />
the performance of at least 100 peripheral<br />
angiograms and 50 peripheral angioplasty<br />
procedures.<br />
Applicants will be required to provide such<br />
documentation from the Director of Fellowship<br />
training or by letter from primary hospital where<br />
he/she has been practicing for the previous two years:<br />
1. Fellowship training in Interventional Radiology<br />
OR<br />
2. Selective catheterization of the hepatic artery and<br />
performance of diagnostic Arteriography in at<br />
least ten (10) cases<br />
AND<br />
3. Evidence of performance of Hepatic Artery<br />
Chemoembolization under supervision of a<br />
physician experienced in the procedure in at least<br />
five (5) cases.<br />
1. Evidence of training and competency by<br />
certification, or admissible for certification by the<br />
American Board of Radiology, Cardiovascular<br />
Disease by the American Board of Internal Medicine<br />
or Vascular Surgery by the American Board of<br />
Surgery.<br />
– AND –<br />
2 Documentation from the training program that the<br />
training program included concentrated training and<br />
experience in angiography including at least 50 noncoronary<br />
arteriographic procedures performed<br />
proficiently and successfully.<br />
-OR – In the absence of residency training in<br />
this procedure, documentation of successful<br />
completion of 100 non-coronary angiographic<br />
procedures from a Joint Commission accredited<br />
hospital within the past three years is required. This<br />
documentation must also include a letter of reference<br />
from a physician who is familiar with the applicant’s<br />
NONE<br />
Five (5) non-cerebral<br />
peripheral angiography<br />
procedures.<br />
Reappointment<br />
Requirements<br />
Two (2) procedures<br />
within prior two<br />
year period<br />
Twenty (20) noncoronary,<br />
noncerebral<br />
peripheral<br />
and visceral<br />
arteriography<br />
procedures.<br />
Number<br />
Performed<br />
Page 8 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
Peripheral and Visceral Arteriography - Continued experience in arteriography.<br />
-OR – Successful completion of an approved<br />
In-house Learning and Teaching Program in noncerebral<br />
diagnostic peripheral angiography consisting<br />
of at least 50 procedures.<br />
[ ] Image Guided Tissue Ablation PRE-REQUISITE: It is understood that physicians<br />
who have been granted image-guided tissue ablation<br />
privileges may only utilize this therapy for the imageguided<br />
modality they hold privileges for (e.g., CT,<br />
ultrasound, MR, fluoroscopic).<br />
In order to perform image-guided tissue ablation, the<br />
physician must fulfill both criteria below:<br />
1. Physician must have performed a minimum of<br />
fifty (50) image-guided biopsy procedures.<br />
AND<br />
Reappointment<br />
Requirements<br />
NONE Minimum of 100<br />
image-guided<br />
biopsies or<br />
ablations over a<br />
two-year period, of<br />
which ten (10)<br />
must be ablations.<br />
Number<br />
Performed<br />
2. Physician must provide written documentation of<br />
proof of training for each tissue ablation technique<br />
requested, i.e. cryo, radiofrequency- or microablation.<br />
Acceptable training can include:<br />
a. Manufacturer sponsored course; OR<br />
. Fellowship training with at least ten (10)<br />
procedures performed as primary operator for<br />
each specific technique for which credentials<br />
are requested; OR<br />
c. Direct supervision through an In House<br />
Learning and Teaching Program at a Joint<br />
Commission accredited hospital by an<br />
attending physician/preceptor who has had<br />
significant training using the specific ablation<br />
technique requested. Significant training of<br />
the preceptor is defined as at least five (5)<br />
ablation procedures performed in previous<br />
year.<br />
Page 9 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
[ ] Endovascular Repair of Aortic Aneurysms Prerequisite:<br />
1. Must currently hold all Interventional<br />
Radiology privileges (to include peripheral<br />
arteriography, angioplasty, intravascular<br />
stenting, and intravascular embolization).<br />
2. Participation with physicians who are<br />
privileged to perform open repair of aortic<br />
aneurysms.<br />
3. Intensive care admitting privileges<br />
Training/Documentation Requirement:<br />
1. Completion of an interventional radiology<br />
fellowship program where endovascular aortic<br />
aneurysm repair was an integral part of the training.<br />
This training must have occurred within the previous<br />
two years. Verification of this training in the form of<br />
a letter from the fellowship director is required.<br />
- OR -<br />
2. Documentation of prior experience in a Joint<br />
Commission accredited hospital in endovascular aortic<br />
aneurysm repair. This experience must have occurred<br />
within the previous two years. Documentation must<br />
include a letter from the Chief of the Department or<br />
Chief of Staff documenting experience in at least ten<br />
(10) cases.<br />
- OR -<br />
1. Successful completion of an approved in-house<br />
teaching program at <strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>.<br />
-AND-<br />
Compliance with FDA guidelines for deployment of<br />
stent-graft devices in use.<br />
First two (2) cases.<br />
Reappointment<br />
Requirements<br />
Minimum of ten<br />
(10) cases from a<br />
JC accredited<br />
hospital.<br />
ALSO<br />
Continuing<br />
education should<br />
be in accordance<br />
with the American<br />
College of<br />
Radiology Practice<br />
Guidelines for<br />
Continuing<br />
<strong>Medical</strong> Education<br />
(150 hours of CME<br />
every 3 years, 70%<br />
in specialtyspecific<br />
or related<br />
areas to include a<br />
minimum of 10<br />
hours of category I<br />
CME specific to<br />
aortic pathology<br />
and endovascular<br />
repair).<br />
Number<br />
Performed<br />
Page 10 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
III. <strong>DI</strong>AGNOSTIC NEURORA<strong>DI</strong>OLOGY<br />
[ ] Core Diagnostic Neuroradiology<br />
Core Diagnostic Neuroradiology includes<br />
performance of diagnostic and image-guided<br />
diagnostic and therapeutic procedures related to the<br />
nervous system and head and neck. For example<br />
(not all inclusive): CT, MRI, myelography, spine<br />
injections, vertebroplasty, spine and maxillofacial<br />
biopsy. (Note: See separate multi-departmental<br />
privilege criteria for cerebral angiography.)<br />
[ ] Diagnostic Cerebral Angiography, Including<br />
WADA Test<br />
(This privilege is shared with another department)<br />
1. Current certification by the American Board of<br />
Radiology; AND,<br />
2. Completion of a neuroradiology fellowship and/or<br />
Certificate of Added Qualifications (CAQ) in<br />
Neuroradiology by the American Board of<br />
Radiology<br />
AND<br />
3. Fifty (50) diagnostic neuroradiology cases in the<br />
previous two years as demonstrated by a letter<br />
from the Director of the training program or<br />
Department Chief.<br />
1. Documentation of a formal training program in<br />
which diagnostic cerebral angiography was part of<br />
the training program. Documentation must be<br />
provided by the Director of the training program<br />
- OR-<br />
2. Post Residency or Fellowship Training<br />
documentation of prior experience at another Joint<br />
Commission accredited hospital within the past<br />
three (3) years. Documentation must be provided<br />
by the Department Chief at the other hospital.<br />
- OR –<br />
3. Successful completion of an approved in-house<br />
learning and teaching program. Documentation<br />
must be provided by the Preceptor at the end of<br />
the in-house training program.<br />
AND (Meet one of the following)<br />
1. Interventional Radiologists who hold Peripheral<br />
Transluminal Angioplasty privileges are required<br />
to provide evidence of training/experience in a<br />
minimum of 50 cerebral angiographies.<br />
2. Neuroradiologists with fellowship training in<br />
Neuroradiology or admissible for subspecialty<br />
Certificate of Added Qualification in<br />
Neuroradiology by the ABR or evidence of<br />
continuous practice in the field in the previous two<br />
years.<br />
First six (6) cases.<br />
Current senior staff<br />
members who qualify<br />
under these criteria and<br />
have been performing<br />
these procedures will be<br />
grandfathered in and<br />
proctoring will not be<br />
required.<br />
The first Six (6)<br />
cerebral angiography<br />
procedures.<br />
Proctoring will be<br />
performed by another<br />
Senior Staff physician<br />
who holds cerebral<br />
angiography privileges.<br />
Reappointment<br />
Requirements<br />
Twelve 12 different<br />
catheterizations in<br />
previous two years.<br />
Volume requirements<br />
can include<br />
cases the physician<br />
performed at other<br />
facilities and are<br />
not exclusive to<br />
SMCS patients.<br />
Twelve (12)<br />
cerebral<br />
angiography<br />
procedures.<br />
Should the<br />
applicant not attain<br />
the suggested<br />
number of<br />
procedures<br />
proctoring may be<br />
initiated as<br />
determined by the<br />
Department<br />
Q.I./Administrative<br />
Committee.<br />
Number<br />
Performed<br />
Page 11 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
IV. INTERVENTIONAL NEURORA<strong>DI</strong>OLOGY<br />
[ ] Core Neuro-Interventional Radiology<br />
Includes performance of image-guided therapeutic and<br />
diagnostic procedures which involve intracranial<br />
catheterization and/or instrumentation. For example<br />
(not all inclusive): aneurysm coiling; intracranial<br />
angioplasty and stenting; cerebral infusion treatment;<br />
embolizations intra and extra cranial; and, cord cyst<br />
puncture<br />
(This privilege criteria is shared with another<br />
department)<br />
[ ] Extra-Cranial Cerebral Revascularization<br />
Includes angioplasty and/or placement of stents in the<br />
extra-cranial circulation with proximal or distal<br />
protection devices.<br />
(This privilege is shared with another department)<br />
(Continued on next page)<br />
Pathway A:<br />
1. Current certification by the American Board of<br />
Radiology; AND<br />
2. Completion of a one or two-year Neuroradiology<br />
fellowship AND<br />
3. Completion of an interventional Neuroradiology<br />
fellowship<br />
-OR-<br />
Pathway B:<br />
1. Current certification by the American Board of<br />
Radiology; AND<br />
2. Completion of a two-year Neuroradiology<br />
fellowship<br />
AND<br />
3. Continuous practice in a Joint Commission<br />
accredited hospital since training in<br />
Neuroradiology with demonstration of<br />
interventional procedure experience in fellowship<br />
training.<br />
ALSO:<br />
Fifty (50) Neurointerventional Radiology cases in the<br />
previous two years as demonstrated by a letter from<br />
the Director of the training program or Department<br />
Chief.<br />
PREREQUISITES<br />
1. Hold one of the following groups of privileges:<br />
a. Neuro-Interventional Radiology and Cerebral<br />
Angiography <strong>Privilege</strong>s; or,<br />
b. Interventional Radiology Peripheral<br />
Transluminal Angioplasty and Cerebral<br />
Angiography <strong>Privilege</strong>s.<br />
– AND –<br />
2. Document prior experience in using distal<br />
protection devices in at least 20 cases in any<br />
vascular territory.<br />
First six (6) cases .<br />
Current senior staff<br />
members who qualify<br />
under these criteria and<br />
have been performing<br />
these procedures will be<br />
grandfathered in and<br />
proctoring will not be<br />
required.<br />
First six (6) extracranial<br />
revascularization<br />
procedures.. Proctoring<br />
will be performed by<br />
another Senior Staff<br />
physician who holds<br />
extra-cerebral<br />
revascularization<br />
privileges and who has<br />
also successfully<br />
completed proctoring.<br />
Reappointment<br />
Requirements<br />
Twelve (12)<br />
interventional<br />
Neuroradiology<br />
cases in previous<br />
two years.<br />
Requirements can<br />
include cases that<br />
the physician<br />
performed at other<br />
facilities and are<br />
not exclusive to<br />
<strong>Sutter</strong> <strong>Medical</strong><br />
<strong>Center</strong>, Sacramento<br />
patients.<br />
Physician should<br />
be prepared to<br />
supply verification<br />
of volume<br />
performance if<br />
requested.<br />
Six (6) intra-cranial<br />
cerebral<br />
revascularization<br />
(carotid stent)<br />
procedures with<br />
use of distal<br />
protection devices.<br />
Should an applicant<br />
not attain the<br />
suggested number<br />
Number<br />
Performed<br />
Page 12 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
Extra-Cranial Cerebral Revascularization -<br />
Continued<br />
TRAINING/EXPERIENCE REQUIREMENTS<br />
1. Documentation of a formal training program<br />
where extra-cranial revascularization (carotid<br />
stenting) was part of the training program.<br />
Applicant must have performed at least 10 extracranial<br />
cerebral revascularization (carotid stent)<br />
procedures. Documentation must be provided by<br />
the Director of the training program.<br />
OR-<br />
2. Post Residency or Fellowship Training<br />
a. Documentation of successful completion of a<br />
post-graduate course (approved by the<br />
department) - AND -<br />
b. Documentation of prior experience at another<br />
Joint Commission accredited hospital in at<br />
least 10 extra-cranial cerebral<br />
revascularization (carotid stent) procedures<br />
OR successful completion of an approved inhouse<br />
learning and teaching program in at<br />
least 10 extra-cranial cerebral<br />
revascularization (carotid stent) procedures.<br />
Documentation must be provided by the<br />
Chief of the Department of the other Joint<br />
Commission accredited hospital or by the<br />
Preceptor at the end of the in-house training<br />
program.<br />
Reappointment<br />
Requirements<br />
of procedures<br />
proctoring may be<br />
initiated as<br />
determined by the<br />
Department<br />
Q.I./Administrative<br />
Committee.<br />
Number<br />
Performed<br />
Page 13 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
V. NUCLEAR ME<strong>DI</strong>CINE Evaluations at 3, 6 &<br />
12 Months<br />
[ ] Diagnostic Nuclear Medicine 1. Completion of an approved Radiology or Nuclear<br />
Medicine residency within three years<br />
OR<br />
2. Current certification by the American Board of<br />
Radiology or the American Board of Nuclear<br />
Medicine<br />
OR<br />
A mix of fifty (50)<br />
cases representative of<br />
the privileges requested.<br />
A written report of their<br />
evaluation should be<br />
submitted and include<br />
the case numbers.<br />
Reappointment<br />
Requirements<br />
Maintain current<br />
California<br />
Radioactive<br />
Materials License<br />
Number<br />
Performed<br />
[ ] Therapeutic Nuclear Medicine<br />
(Includes Radioactive Iodine Thyroid Therapy<br />
<strong>Privilege</strong>s)<br />
3. Documentation of previous 10 years experience in<br />
diagnostic nuclear medicine at a Joint<br />
Commission accredited institution<br />
AND<br />
Current California Radioactive Materials<br />
License<br />
1. Completion of an approved Nuclear Medicine<br />
residency within three years<br />
OR<br />
2. Certification or admissible to the Board of Nuclear<br />
Medicine<br />
OR<br />
A mix of fifty (50)<br />
cases representative of<br />
the privileges requested.<br />
A written report of their<br />
evaluation should be<br />
submitted and include<br />
the case numbers.<br />
Minimum of at<br />
least ten (10)<br />
therapeutic nuclear<br />
medicine<br />
procedures during<br />
the previous two<br />
years.<br />
3. Documentation of previous 10 years experience in<br />
therapeutic nuclear medicine at a Joint Comission<br />
accredited institution with documentation of at<br />
least ten therapeutic nuclear medicine procedures<br />
performed at a Joint Commission accredited<br />
institution during the previous two years.<br />
Page 14 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
[ ] Non-invasive vascular testing 1. Currently granted Diagnostic or Therapeutic<br />
Nuclear Medicine privileges at <strong>Sutter</strong> <strong>Medical</strong><br />
<strong>Center</strong>, Sacramento (SMCS)<br />
AND<br />
2. Documentation of performance of at least 200<br />
vascular studies of which 100 cases need to be<br />
carotid ultrasound during previous three years.<br />
Documentation can be from residency program or a<br />
letter from the department medical director or<br />
medical staff department chief at a Joint<br />
Commission accredited institution.<br />
[ ] Cardiac Treadmill and Pharmacologic Stress Testing 1. Currently granted Diagnostic Nuclear Medicine<br />
privileges at SMCS;<br />
AND (one of the following☺<br />
1. Board certification or admissibility from the<br />
American Board of Radiology or American Board<br />
of Nuclear Medicine; or,<br />
2. Documentation of at least fifty (50) procedures<br />
performed at a Joint Commission accredited<br />
A mix of fifty (50)<br />
cases representative of<br />
the privileges requested.<br />
A written report of their<br />
evaluation should be<br />
submitted and include<br />
the case numbers.<br />
Six (6) cases are to be<br />
proctored by a SMCS<br />
Senior Staff physician<br />
granted similar<br />
privilege.<br />
institution during the previous two years.<br />
VI. RA<strong>DI</strong>ATION ONCLOLOGY<br />
[ ] Core <strong>Radiation</strong> <strong>Oncology</strong> First five (5) cases<br />
[ ] Intra-operative <strong>Radiation</strong> Therapy 1. Must have full specialty privileges in the<br />
Diagnostic Imaging and <strong>Radiation</strong> <strong>Oncology</strong><br />
Department.<br />
Reappointment<br />
Requirements<br />
NONE<br />
NONE<br />
First two (2) cases NONE<br />
Number<br />
Performed<br />
2. Must either observe or assist in one case wit<br />
documentation submitted at the time of privilege<br />
request.<br />
Page 15 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Request <strong>Privilege</strong> Appointment Requirements Proctoring Required<br />
Reappointment<br />
Requirements<br />
[ ] Gamma Knife 1. Must have full specialty privileges in the<br />
NONE Minimum of 10<br />
Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong><br />
(10) cases in a two<br />
Department at <strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>,<br />
year period.<br />
Sacramento.<br />
Also, must<br />
participate in<br />
2. Must be board certified or board eligible by<br />
emergency<br />
the American Board of Radiology.<br />
response<br />
procedures every<br />
3. Must have successfully completed<br />
month and must<br />
specialized training in gamma knife<br />
attend and<br />
stereotactic radiosurgery at an approved<br />
actively<br />
Elekta sponsored gamma knife radiosurgery<br />
participate in<br />
user training course.<br />
30% of all<br />
scheduled gamma<br />
4. Must have documentation of involvement in<br />
knife patient<br />
five (5) gamma knife procedures under the<br />
selection and<br />
supervision of a qualified physician preceptor<br />
follow up<br />
involving the application of ionizing<br />
conferences within<br />
radiation for the treatment of neurological<br />
a 24-month<br />
lesions using stereotactic techniques,<br />
period.<br />
including target localization, treatment<br />
planning, treatment procedures, radiation<br />
safety and emergency response procedures<br />
applicable to stereotactic radiosurgery<br />
techniques.<br />
Note: Critical Care Unit <strong>Privilege</strong>s are obtained through the Department of Medicine<br />
5. Must participate in emergency response<br />
procedures every twelve months and must<br />
attend and actively participate in 30% of all<br />
scheduled gamma knife patient selection and<br />
follow up conferences within a 24-month<br />
period. This requirement is necessary to<br />
obtain and maintain privileges.<br />
Number<br />
Performed<br />
Page 16 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.
<strong>Sutter</strong> <strong>Medical</strong> <strong>Center</strong>, Sacramento<br />
Department Of Diagnostic Imaging & <strong>Radiation</strong> <strong>Oncology</strong> - Delineation Of <strong>Privilege</strong>s<br />
NAME:<br />
Acknowledgment of Practitioner: I understand that (a) in exercising clinical privileges granted, I am constrained by <strong>Medical</strong> Staff Policies and Procedures, Rules and Regulations,<br />
and (b) any restriction on the clinical privileges granted to me is waived in an emergency situation and in such situation my actions are governed by the applicable section of the<br />
<strong>Medical</strong> Staff Bylaws.<br />
By completing and submitting this privilege delineation form, you are attesting that you have performed the stipulated number of procedures as indicated above.<br />
*********************************************************************************************************************************<br />
COMMITTEE APPROVALS<br />
Department QI/Administrative Committee Date:<br />
Or Dept Chief (in lieu of mtg)<br />
Credentials Committee Date:<br />
<strong>Medical</strong> Executive Committee Date:<br />
Board of Directors Date:<br />
TEMPORARY PRIVILEGE APPROVAL<br />
Department Chief:<br />
Date:<br />
DOCUMENT APPROVAL Dates:<br />
Dept of <strong>DI</strong>RO Administrative Committee October 12, 2011<br />
Credentials Committee November 8, 2011<br />
<strong>Medical</strong> Executive Committee December 20, 2011<br />
<strong>Medical</strong> Policy Committee January 5, 2012<br />
Board of Directors February 13, 2012<br />
Page 17 of 17<br />
Note: Approval is subject to the terms of the hospital's exclusive contract for Radiology services, i.e., approval is for second opinion consultations only, it being understood that the<br />
hospital's contracting Radiologists are primarily responsible for these services.