mathematical modelling of hiv/aids dynamics with treatment ... - NOMA
mathematical modelling of hiv/aids dynamics with treatment ... - NOMA
mathematical modelling of hiv/aids dynamics with treatment ... - NOMA

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
MATHEMATICAL MODELLING OF HIV/AIDS DYNAMICSWITH TREATMENT AND VERTICAL TRANSMISSIONAbdalla Sheha WazirM.Sc. (Mathematical <strong>modelling</strong>) DissertationUniversity <strong>of</strong> Dar es salaamJuly, 2011
MATHEMATICAL MODELLING OF HIV/AIDS DYNAMICSWITH TREATMENT AND VERTICAL TRANSMISSIONByAbdalla Sheha WazirA Dissertation Submitted in Partial Fulfilment <strong>of</strong> the Requirements for theDegree <strong>of</strong> Master <strong>of</strong> Science (Mathematical Modelling) <strong>of</strong> the University <strong>of</strong>Dar es SalaamUniversity <strong>of</strong> Dar es salaamJuly, 2011
iCERTIFICATIONThe undersigned certify that they have read and hereby recommend for acceptanceby the University <strong>of</strong> Dar es salaam a dissertation entitled: Mathematical Modelling<strong>of</strong> HIV/AIDS Dynamics <strong>with</strong> Treatment and Vertical Transmission, in partialfulfilments <strong>of</strong> the requirements for the degree <strong>of</strong> Master <strong>of</strong> Science (Mathematical<strong>modelling</strong>) <strong>of</strong> the University <strong>of</strong> Dar es Salaam.………………………………Dr. E. S. Massawe(Supervisor)Date………………………………………………………..Pr<strong>of</strong>. Oluwole D. Makinde(Supervisor)Date 14 th June 2011
iiDECLARATIONANDCOPYRIGHTI, Abdalla Sheha Wazir, declare that this dissertation is my own original work andthat it has not been presented and will not be presented to any other University for asimilar or any other degree award.Signature ……………………………….This dissertation is copyright material protected under the Berne Convention, theCopyright Act 1999 and other international and national enactments, in that behalf,on intellectual property. It may not be reproduced by any means, in full or in part,except for short extracts in fair dealings, for research or private study, criticalscholarly review or discourse <strong>with</strong> an acknowledgement, <strong>with</strong>out the writtenpermission <strong>of</strong> the Directorate <strong>of</strong> Postgraduate Studies, on behalf <strong>of</strong> both the authorand the University <strong>of</strong> Dar es salaam.
iiiACKNOWLEDGEMENTSI have honoured to thank Almight God for giving me ability and effort to insurecompletion <strong>of</strong> the dissertation and taking me through my study successfully.I would like to express my sincere thanks and appreciation to my supervisors, Pr<strong>of</strong>.O. D. Makinde and Dr. E. S. Massawe for their constructive ideas, guidance,continuous supporting, suggestions and comments through my research work. I wishto express my sincere appreciation to Dr. W. Mahera (Course coordinator) and allstuff members in the Department <strong>of</strong> Mathematics for their support andencouragement for the whole period <strong>of</strong> my study.I acknowledge NORAD for supported and co-organized M.Sc in MathematicalModelling Program at University <strong>of</strong> Dar es Salaam. I am also very grateful to theMinistry <strong>of</strong> Education and Vocational Training-Zanzibar for an incredible partiallyfinancial support for the whole period <strong>of</strong> my study at University <strong>of</strong> Dar es Salaam.My special thanks are directed to my lovely wife Zena H. Makame and my lovelyson Abdulswamad A. Sheha for their patience, tolerance, motivation and support incompleting the program.Moreover, my sincere thanks also to my classmates for their encouragement andsupport throughout our course work program. Finally I thank all who supported medirectly or indirectly toward the struggle <strong>of</strong> attaining this academic level.
vABSTRACTThis study proposes and analyzes a non-linear <strong>mathematical</strong> model for the <strong>dynamics</strong><strong>of</strong> HIV/AIDS <strong>with</strong> <strong>treatment</strong> and vertical transmission. The equilibrium points <strong>of</strong> themodel system are found and their stability is investigated.The model exhibits two equilibria namely, the disease-free and the endemicequilibrium. It is found that if the basic reproduction number R0 1, the disease-freeequilibrium is always locally asymptotically stable and in such a case the endemicequilibrium does not exist. If R0 1, a unique equilibrium exist which locallyasymptotically stable and becomes globally asymptotically stable under certainconditions showing that the disease becomes endemic due to vertical transmission.By using stability theory and computer simulation, it is shown that by using<strong>treatment</strong> measures (ARVs) and by controlling the rate <strong>of</strong> vertical transmission, thespread <strong>of</strong> the disease can reduced significantly and also the equilibrium values <strong>of</strong>infective, pre-AIDS and AIDS population can be maintained at desired levels.A numerical study <strong>of</strong> the model is also used to investigate the influence <strong>of</strong> certainkey parameters on the spread <strong>of</strong> the disease.
viTABLE OF CONTENTSCertification...............................................................................................................iDeclaration and Copyright ........................................................................................iiAcknowledgements................................................................................................. iiiDedication ...............................................................................................................ivAbstract ....................................................................................................................vTable <strong>of</strong> Contents.....................................................................................................viList <strong>of</strong> Figures .......................................................................................................viiiList <strong>of</strong> Tables............................................................................................................xCHAPTER ONE: INTRODUCTION ....................................................................11.1 General Introduction.....................................................................................11.2 Statement <strong>of</strong> the Problem..............................................................................51.3 General Objectives .......................................................................................61.4 Specific Objectives.......................................................................................61.5 Significant <strong>of</strong> the Study ................................................................................6CHAPTER TWO: LITERATURE REVIEW .......................................................82.1 Research Hypothesis ..................................................................................102.2 Methodology..............................................................................................11CHAPTER THREE: THE MODEL DESCRIPION AND ANALYSIS .............123.0 Historical Background................................................................................123.1 Model Formulation.....................................................................................153.2 Positivity <strong>of</strong> Solutions ................................................................................21
vii3.3 Stability Analysis <strong>of</strong> the Model...................................................................253.4 Equilibrium Points <strong>of</strong> the Model.................................................................253.5 Computation <strong>of</strong> the Basic Reproduction Number, R0.................................263.6 Local Stability <strong>of</strong> the Disease Free Equilibrium..........................................283.7 The Endemic Equilibrium and Local Stability ............................................313.8 Existence <strong>of</strong> Forward Bifurcation ...............................................................363.9 Global Stability <strong>of</strong> the Endemic Equilibrium ..............................................43CHAPTER FOUR: THE NUMERICAL SIMULATIONS OF THEMODEL...494.1 Model Simulation.......................................................................................49CHAPTER FIVE: DISCUSSION, CONCLUTION AND FUTUREWORK .....705.1 Discussion..................................................................................................705.2 Conclusions................................................................................................745.3 Future Work...............................................................................................75REFFERENCES...................................................................................................76
viiiLIST OF FIGURES3.1 The flow chart <strong>of</strong> the model. .............................................................................163.2 Forward Bifurcation <strong>of</strong> the model (3.3). ............................................................434.1(a). Endemic equilibrium <strong>of</strong> proportion <strong>of</strong> infectives <strong>with</strong> Susceptible................504.1(b). Endemic equilibrium <strong>of</strong> proportion <strong>of</strong> Pre-AIDS population........................504.1(c). Endemic equilibrium <strong>of</strong> proportion <strong>of</strong> treated class ......................................514.1(d). Endemic equilibrium <strong>of</strong> proportion <strong>of</strong> AIDS population ..............................514.2(a) Variation <strong>of</strong> population in different classes for 0 and 0 .....................534.2(b) Variation <strong>of</strong> population in different classes for 0.1 and 0.2. ............534.3(a) Variation <strong>of</strong> infected population for different values <strong>of</strong> . .............................544.3(b) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> . ................................554.3(c) Variation <strong>of</strong> Treated class for different values <strong>of</strong> . .......................................554.4(a) Variation <strong>of</strong> Susceptible for different values <strong>of</strong> . .........................................564.4(b) Variation <strong>of</strong> Treated population for different values <strong>of</strong> . ............................574.4(c) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> . ...............................574.5(a) Variation <strong>of</strong> Infective population for different values <strong>of</strong> . ...........................584.5(b) Variation <strong>of</strong> pre-AIDS population for different values <strong>of</strong> . .........................594.5(c) Variation <strong>of</strong> Treated class for different values <strong>of</strong> . ......................................594.5(d) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> . ...............................604.6(a) Variation <strong>of</strong> pre-AIDS population for different values <strong>of</strong> 1.........................614.6(b) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> 1...............................614.6(c) Variation <strong>of</strong> Treated population for different values <strong>of</strong> 2............................624.6(d) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> 2...............................62
ix4.7(a) Variation <strong>of</strong> Susceptibles population for different values <strong>of</strong> 1.....................634.7(b) Variation <strong>of</strong> Infectives population for different values <strong>of</strong> 1.........................644.7(c) Variation <strong>of</strong> Susceptibles population for different values <strong>of</strong> 3.....................644.7(d) Variation <strong>of</strong> Infectives population for different values <strong>of</strong> 3.........................654.8(a) Variation <strong>of</strong> Susceptibles population for different values <strong>of</strong> c1......................664.8(b) Variation <strong>of</strong> Infectives population for different values <strong>of</strong> c1..........................664.8(c) Variation <strong>of</strong> Susceptibles population for different values <strong>of</strong> c3.....................674.8(d) Variation <strong>of</strong> Infectives population for different values <strong>of</strong> c3.........................674.9(a) Variation <strong>of</strong> AIDS patients for different values <strong>of</strong> k and . .......................684.9(a) Variation <strong>of</strong> AIDS patients for different values <strong>of</strong> k and . .......................684.10 Variation <strong>of</strong> AIDS populations for different values <strong>of</strong> ................................69
xLIST OF TABLES3.1 Definitions <strong>of</strong> Symbols used frequently. ........ …………………………………153.2 Definitions <strong>of</strong> Parameters used frequently………………………………………16
1CHAPTER ONEINTRODUCTION1.1 General IntroductionThe human immunodeficiency virus (HIV) infection which can lead to acquiredimmunodeficiency syndrome (AIDS), has become a hazard infectious disease in boththe developed and developing nations. It is a fatal disease, which breaks down thebody’s immune system, leaving the victim vulnerable to a host <strong>of</strong> life threateningopportunistic infections, neurological disorders or unusual malignancies. It hascaused mortality <strong>of</strong> millions <strong>of</strong> people and expenditure <strong>of</strong> enormous amount <strong>of</strong>money in health care and disease control (Naresh et. al.,2006).AIDS is one <strong>of</strong> the deadliest epidemics in human history. It was first identified in1981 in New York and California (USA). Shortly after its detection in the UnitedStates, AIDS quickly developed into a worldwide epidemic, affecting virtually everynation. About 90 percent <strong>of</strong> all HIV-infected people live in the developing countries(http://data.un<strong>aids</strong>.org/pub/GlobalReport/2008). In 2007 it was estimated that twothirds (67%) <strong>of</strong> the global total <strong>of</strong> 32.9 million people <strong>with</strong> HIV live in this region,and three quarters (75%) <strong>of</strong> all AIDS deaths in 2007 occurred(http://data.un<strong>aids</strong>.org/pub/GlobalReport/2008). Consequently, it is estimated that bythe year 2020 the nine most severely hit Sub-Saharan countries may lose 13%–26%<strong>of</strong> their agricultural labour force to HIV/AIDS. The Growth Domestic Product incountries <strong>with</strong> HIV prevalence rates 10% or higher could contract AIDS by 18% by2020 (Amoako et. al., 2008). Women in Sub-Saharan Africa account for 58% <strong>of</strong> all
2HIV infections in the region, but a striking 78% <strong>of</strong> those young people (ages 15–24years) living <strong>with</strong> HIV are females (http://data.un<strong>aids</strong>.org/pub/GlobalReport/2008).Sub-Saharan African women and children are particularly at risk for HIV/AIDS. InJune 2000, UNAIDS reported that one in five women under the age <strong>of</strong> 25 areinfected <strong>with</strong> HIV in Africa. HIV/AIDS transmission in Africa is primarily throughheterosexual sex and vertical transmission (mother-to-child). Forty percent <strong>of</strong> allHIV/AIDS cases result from mother to child transmission. While fewer than 300infants in the U.S acquired HIV through vertical transmission in 1997. In sub-Saharan Africa over 2.5 million children under the age <strong>of</strong> 15 have died <strong>of</strong> AIDS,most <strong>of</strong> these children were exposed to HIV during labour or breastfeeding.HIV/AIDS is a serious threat to future development in Africa. The cost <strong>of</strong> one year<strong>of</strong> basic healthcare for an individual living <strong>with</strong> HIV/AIDS is two to three timesmore than the average per-capita gross domestic product <strong>of</strong> some African countries.HIV prevention programs are less expensive than HIV care and should be a criticalcomponent <strong>of</strong> any HIV/AIDS intervention program (Adelman, 2001).In the United Republic <strong>of</strong> Tanzania there is a dynamic <strong>of</strong> HIV/AIDS epidemic,which is still growing. The first case <strong>of</strong> HIV/AIDS in Tanzania was reported in 1983.By 1985, an estimated number <strong>of</strong> people living <strong>with</strong> HIV/AIDS was 140,000 (1.3%prevalence) and by 1990 the estimated number was about 900,000 (7.2%prevalence). According to the surveillance report on HIV/AIDS and sexuallytransmitted infections issued July 2009 published by the National Aids ControlProgrammes(NACP), about 1.4 million Tanzanians (1,300,000 adults and 110,000children) are living <strong>with</strong> HIV infection, in a total population <strong>of</strong> 41 million. The
3social, economic, and environmental impact <strong>of</strong> the pandemic is sorely felt as anestimated 140,000 Tanzanians have perished, leaving behind as estimate 2.5 millionorphans and vulnerable children, representing approximately 10 to 12% <strong>of</strong> allTanzanian children. Since the National AIDS Control Programme was established in1985, the progress <strong>of</strong> the epidemic has been monitored through unlinked anonymoustesting <strong>of</strong> blood from pregnant women attending antennal clinics for the first time inselected sentinel sites.Treatment is the process <strong>of</strong> <strong>of</strong>fering the HIV positive individual <strong>with</strong> a lifeprolonging drugs/medicines known as antiretroviral (ARV) medicines or ART. ARTdrugs are the main types <strong>of</strong> <strong>treatment</strong> for HIV/AIDS. It is not a cure but it canprolong the life <strong>of</strong> a person for many years. It consists <strong>of</strong> drugs that have to be takenevery day for the rest <strong>of</strong> person’s life. It keeps the amount <strong>of</strong> HIV in the body at lowlevel which retards any weakening <strong>of</strong> immune system and allows it to recover fromany damage that HIV might have caused already (AVERT, 2010). Treatment <strong>with</strong>anti-retroviral increases the life expectancy <strong>of</strong> people infected <strong>with</strong> HIV. Even afterHIV has progressed to diagnosable AIDS, the average survival time <strong>with</strong>antiretroviral therapy was estimated to be more than 5 years as <strong>of</strong> 2005 (Schneider et.al.,2005).Without antiretroviral therapy, someone who has AIDS typically dies<strong>with</strong>in a year (Morgan et. al., 2002).WHO estimated that 1.2 million people started <strong>treatment</strong> in 2009 bringing the totalnumber <strong>of</strong> people receiving live saving HIV <strong>treatment</strong> in low and middle incomecountries to 5.2 million compared to 4 million at the end <strong>of</strong> 2008 (WHO, 2010). Bythe end <strong>of</strong> 2008, 2.9 millions adults and children in Sub-Saharan Africa were
4receiving ART while those in need were 6.7 million (UNAIDS/WHO 2009). InTanzania the number <strong>of</strong> HIV positive to be initiated on ART is expected to increasefrom 440,000 in 2008 to 600,000 in 2012 (ICAP Tanzania, 2004).Current <strong>treatment</strong> for HIV infection consists <strong>of</strong> Highly Active AntiretroviralTherapy, or HAART(http://www.hab.hrsa.gov/tools/HIVpocketguide05/PktGARTtables.htm). This hasbeen highly beneficial to many HIV-infected individuals since its introduction in1996, when the protease inhibitor-based HAART initially became available (Palellaet. al., 1998).The development <strong>of</strong> HAART as effective therapy for HIV infection has substantiallyreduced the death rate from this disease in those areas where these drugs are widelyavailable (Palella et. al., 1998). As the life expectancy <strong>of</strong> persons <strong>with</strong> HIV hasincreased in countries where HAART is widely used, the continuing spread <strong>of</strong> thedisease has caused the number <strong>of</strong> persons living <strong>with</strong> HIV to increase substantially.Vertical transmission is the transmission <strong>of</strong> the HIV virus from mother to the child.Vertical transmission from mother to child can occur in utero (during pregnancy),during labour and delivery, and through breastfeeding. In Sub-Saharan African, therisk <strong>of</strong> transmission through this means ranges between 10 percent and 30 percent.Without prophylaxis, between 20% and 25% <strong>of</strong> babies born to HIV-positive womenwill be infected <strong>with</strong> HIV. As a result, prevention <strong>of</strong> vertical transmission hasbecome a critical component <strong>of</strong> national and global responses to HIV. Women living<strong>with</strong> HIV have the right to enjoy the benefits <strong>of</strong> scientific progress and the healthservices that enable them to reduce the risk <strong>of</strong> transmitting HIV to their children.
5They also have the right, like all women, to become pregnant, to control the numberand spacing <strong>of</strong> their children, get married and form the family. In addition to theirHIV prevention impact, services to prevent vertical transmission are an obvious forrealising the integration <strong>of</strong> reproductive health and HIV/AIDS programmes, which isa public health goal in many countries and a recommendation <strong>of</strong> the World HealthOrganization (WHO) (Cset et. al., 2009).In the absence <strong>of</strong> <strong>treatment</strong>, the transmission rate up to birth between the mother andchild is around 25% (Coovadia, 2004). However, where combination antiretroivaldrug <strong>treatment</strong> and Cesarian section are available, this risk can be reduced to as lowas one percent. Postnatal mother-to-child transmission may be largely prevented bycomplete avoidance <strong>of</strong> breast feeding; however, this has significant associatedmorbidity. Exclusive breast feeding and the provision <strong>of</strong> extended antiretroviralprophylaxis to the infant are also efficacious in avoiding transmission(http://www.cochrane.org/reviews/en/ab006734.html).Naresh et. al.,(2006),carried a study on <strong>mathematical</strong> <strong>modelling</strong> <strong>of</strong> the spread <strong>of</strong>HIV/AIDS epidemic <strong>with</strong> vertical transmission. However they did not include<strong>treatment</strong> in their model. This study there fore aims at improving the model done by(Naresh et al.,2006) by considering <strong>treatment</strong> and vertical transmission in thedynamic <strong>of</strong> HIV/AIDS.1.2 Statement <strong>of</strong> the ProblemNaresh et. al.,(2006) developed a model for transmission <strong>of</strong> HIV into a population <strong>of</strong>varying size <strong>with</strong> vertical transmission, in which they assumed a varying size
6population recruiting non infected individuals. However, usually infected individualsare recruited or else immigrated into the population. In this research it is intended todevelop a <strong>mathematical</strong> model for transmission <strong>of</strong> HIV/AIDS into a population <strong>of</strong>varying size <strong>with</strong> vertical transmission in the presence <strong>of</strong> <strong>treatment</strong> and otherdemographic and epidemiological factors basing on the population into thecommunity. This will be an improved model from Naresh et al., (2006) as a result <strong>of</strong>including <strong>treatment</strong> which wasn’t considered in their model1.3 General ObjectivesThe general objective <strong>of</strong> this study is to formulate and analyse a model <strong>of</strong> HIV/AIDS<strong>dynamics</strong> <strong>with</strong> <strong>treatment</strong> and vertical transmission.1.4 Specific ObjectivesThe specific objectives <strong>of</strong> this study are:i. To establish a <strong>mathematical</strong> model <strong>of</strong> HIV/AIDS showing the effect <strong>of</strong><strong>treatment</strong> and vertical transmission on the transmission <strong>of</strong> HIV/AIDS.ii. To determine the stability <strong>of</strong> the disease free equilibrium point.iii. To determine the stability <strong>of</strong> endemic equilibrium point.iv. To determine the impact <strong>of</strong> each embedded parameter on the HIV/AIDStransmission.1.5 Significant <strong>of</strong> the StudyThe outcomes <strong>of</strong> this study will help the Government and NGO’s to establishpolicies, programmes and optimal plan for control <strong>of</strong> the disease by taking into
7account the aspect <strong>of</strong> <strong>treatment</strong> and vertical transmission. It will help the society ingeneral to have an understanding on how the disease can be controlled through<strong>treatment</strong> <strong>of</strong> infectives <strong>with</strong> ARV. Also it will add more knowledge to the existingliterature on HIV/AIDS and help Researchers to do more research on this disease.Lastly this study will help educationalist to develop educational seminars, workshopsor training programmes to educate people on the impact <strong>of</strong> <strong>treatment</strong> and verticaltransmission in curbing down the HIV/AIDS epidemic.
9infections in many sub Sahara Africa countries. The use <strong>of</strong> ARVs for prevention isestablished in the prevention <strong>of</strong> mother-to-child programmes and through postexposureprophylaxis for sexual assault and needle-stick injuries. They alsosuggested that, providing antiretroviral therapy infected <strong>with</strong> HIV would stop theHIV epidemic. The researchers narrated that their model assumes little or notransmission would occur from people on antiretroviral <strong>treatment</strong>, based on findingsfrom Uganda, Spain and Taiwan. The model also assumes that instead <strong>of</strong> treatingonly those <strong>with</strong> low CD4 cell counts, all HIV-positive people would receive<strong>treatment</strong> from the time <strong>of</strong> diagnosis to everyone in the world.Fred Brauer (1994), on Models for Diseases <strong>with</strong> Vertical Transmission andNonlinear Population Dynamics had a different approach regarding on the commonassumption to <strong>modelling</strong> communicable disease, most <strong>of</strong> what is known for verticaltransmission models assumes birth rates are proportional to population size, but hadconsidered models <strong>with</strong> nonlinear population <strong>dynamics</strong> and finite carrying capacityand analyze the stability <strong>of</strong> equilibrium in the special case in which the overall birthrate does not depend on infective population size.Busenberg and Cooke, (1993) discussed a variety <strong>of</strong> diseases that transmit bothhorizontally and vertically and gave a comprehensive survey <strong>of</strong> the formulation andthe <strong>mathematical</strong> analysis <strong>of</strong> compartmental models that also incorporate verticaltransmission.Naresh et. al., (2006) developed a model <strong>of</strong> transmission <strong>of</strong> HIV into population <strong>of</strong>varying size <strong>with</strong> vertical transmission and other demographical and epidemiolocalfactors. Their purpose was to formulate a model for AIDS epidemic that may be
10transmitted either directly or vertically in populations and to study its behaviourqualitatively and numerically. They found that an increase in the rate <strong>of</strong> verticaltransmission leads to increase the population <strong>of</strong> infective which in turn increases thepre-AIDS and AIDS population. Thus, they concluded that the vertical spread <strong>of</strong> thedisease should be controlled by the way <strong>of</strong> promoting effective <strong>treatment</strong> to keep theoverall infective population under control.Simwa et. al., (2003) in there paper dealt <strong>with</strong> a deterministic model for HIVepidemic <strong>with</strong> three stages <strong>of</strong> disease progression among infected patients. It isassumed that the patient once infected experiences disease progression up to fullblownAIDS. Using two systems <strong>of</strong> ordinary differential equations that are coupledthrough a delay in one <strong>of</strong> the systems, a compartmental model for the <strong>dynamics</strong> <strong>of</strong>the HIV/AIDS epidemic is constructed. The transmission <strong>of</strong> the disease is consideredto be only through heterosexual contact and vertically from an infected mother to herunborn child. Numerical integration <strong>of</strong> the equations is used for simulating the stagespecificepidemic curves, given the demographic and epidemiological parameters <strong>of</strong>the model. Through simulation it is noted that all the three stage-specific prevalencerate curves also satisfy this condition.2.1 Research HypothesisThe research hypotheses are:i. There exists a <strong>mathematical</strong> model <strong>of</strong> HIV/AIDS <strong>dynamics</strong> <strong>with</strong> <strong>treatment</strong> andvertical transmission.ii.The disease free equilibrium point can be made stable under certain condition.
11iii.iv.The endemic equilibrium point is stable under certain condition.The variations <strong>of</strong> the embedded parameters have positive correlation <strong>with</strong> modelresults.2.2 Methodology.It is proposed to formulate a <strong>mathematical</strong> model for the analysis <strong>of</strong> HIV/AIDS<strong>dynamics</strong> <strong>with</strong> <strong>treatment</strong> and vertical transmission <strong>of</strong> HIV/AIDS using differentialequations. The model to be established will be a modification <strong>of</strong> the modeldeveloped by Naresh et al., (2006). The basic reproduction number ( R ) which is thefundamental parameter governing the transmission or spreading <strong>of</strong> the disease will becomputed using the next generation operator method.oLocal and global stability <strong>of</strong> disease free equilibrium point (DFE) and local stability<strong>of</strong> an endemic equilibrium point (EEP) will be analysed.The model will besimulated to determine the behaviour <strong>of</strong> each embedded parameter for the impact <strong>of</strong><strong>treatment</strong> and vertical transmission on the transmission <strong>of</strong> HIV/AIDS.For numerical analysis and validation <strong>of</strong> the model, estimated and heuristic data willbe used. Simulation <strong>of</strong> the model will be done <strong>with</strong> <strong>mathematical</strong> computer package(MATLAB).
12CHAPTER THREETHE MODEL DESCRIPTION AND ANALYSIS3.0 Historical BackgroundEpidemiology is the study <strong>of</strong> the distribution and determinants <strong>of</strong> diseases bothinfectious and non infectious. Originally the term was used to refer only to the study<strong>of</strong> epidemic infectious diseases but it is now applied more broadly to other diseasesas well (Johnson, 2004). Mathematical models have been used extensively inresearch into the epidemiology <strong>of</strong> HIV/AIDS, to help improve our understanding <strong>of</strong>major contributing factors in a giving epidemic (Naresh at. el., 2006).The goal <strong>of</strong> any <strong>modelling</strong> exercise is to extract as much information as possiblefrom available data and provide an accurate representation <strong>of</strong> both the knowledgeand uncertainty about the epidemic. A number <strong>of</strong> different models <strong>of</strong> HIV and AIDShave been developed, ranging from simple extrapolations <strong>of</strong> past curves to complextransmission models. A major tradition in <strong>modelling</strong> HIV/AIDS epidemics has beento use back calculation, or back projection, techniques. These techniques producestatistical solutions to convolution equations that relate the number <strong>of</strong> AIDSdiagnoses over time to past trends in HIV infection, and to the distribution <strong>of</strong> theHIV incubation period (Salomon and Murray, 2001).In this study we have, therefore, developed a model for transmission <strong>of</strong> HIV into apopulation <strong>of</strong> varying size <strong>with</strong> vertical transmission and other demographic sandepidemiological factors. Our purpose is to formulate a model for AIDS epidemic thatmay be transmuted either horizontally or vertically in populations.
14Model ParametercDescriptionRate <strong>of</strong> recruitment into susceptible population.Average number <strong>of</strong> sexual partners per unit timeSexual contact rateRate <strong>of</strong> movement from infectious classFraction <strong>of</strong> newborns infected <strong>with</strong> HIV who dies immediatelyafter birthRate <strong>of</strong> newborns infected <strong>with</strong> HIVNatural mortality rateInduced death rate due to AIDS1Fraction <strong>of</strong> joining the pre-AIDS classRate <strong>of</strong> movements <strong>of</strong> pre-AIDS class individuals into AIDSclass2Fraction <strong>of</strong> joining treated classmkRate at which AIDS group get <strong>treatment</strong>Fraction <strong>of</strong> who get <strong>treatment</strong>Rate at which treated group becomes full blown AIDSTable 3.2 Definitions <strong>of</strong> Parameters used frequently
153.1 Model FormulationConsider a population <strong>of</strong> sizeNtat time t <strong>with</strong> constant inflow <strong>of</strong> susceptible<strong>with</strong> rate N . The population size tsusceptibles S t, infectives tpatientsN is divided into fives subclasses which areI (also assumed to be infectious), pre-AIDSP t, treated class T t and AIDS patients tA <strong>with</strong> natural mortality rate in all classes. is the disease induced death rate in the AIDS patients class and the rate at which AIDS patients get <strong>treatment</strong>.In the model, it is assumed that the susceptibles become HIV infected via sexualcontacts <strong>with</strong> infective which may also lead to the birth <strong>of</strong> infected children. It isassumed that a fraction <strong>of</strong> new born children are infected during birth and hence aredirectly recruited into the infective class <strong>with</strong> a rate 1 and others dieeffectively at birth 0 1.We do not consider direct recruitment <strong>of</strong> the infected persons but by verticaltransmission only. It is assumed that some <strong>of</strong> the infectives join pre-AIDS class,depending on the viral counts, <strong>with</strong> a rate 1 and then proceed <strong>with</strong> a rate todevelop full blown AIDS, it is also assumed that some <strong>of</strong> the infectives move to jointreated class <strong>with</strong> a rate 2 and then proceed <strong>with</strong> a rate k to develop full blownAIDS while others <strong>with</strong> serious infection directly join the AIDS class <strong>with</strong> a rate1 .1 2The interaction between susceptibles and infectives is assumed to be <strong>of</strong> standardmass action type.
17dA 11 2 I 1 m P kT A,dt<strong>with</strong> the initial conditionsS S , I 0 I 0 ,P0 P 0 ,T 0 T 0 ,and A 000 A,To simplify the model, it is reasonable to assume that the AIDS patients and those inpre-AIDS class are isolated and sexually inactive and hence they are not capable <strong>of</strong>producing children i.e. P 1 1 A 0 and also they do not contribute toviral transmission horizontally i.e. 2and 4are taken negligible (Naresh et.al.,2006)..In view <strong>of</strong> the above assumptions, the system can now be written as follows:dSdtc11IS NNc33TSN SdIdtc11ISc33TS 1N N I IdPdt 1I P(3.2)dTdt 2 I mPAk TdAdt I mP kT A 111 2
18From the system (3.2), it is pointed out here that not all infected individuals take partin spreading the disease, as in the case <strong>of</strong> infected children, but they will all developtheir own AIDS. However, the model can be modified to include a delay to make theinfected children become adult to further spread the infection either vertically orhorizontally.The total population N can be calculated as:N S I P T A , thendNdtdS dI dP dT dA ,dt dt dt dt dtdN c11ISc33TS N Sdt N Nc ISNc TSN I 1 1 3 3 1 1 I P 2 I m P A k T I1 1 I m P kT A1 2Therefore,dN N NA 1 Idt
19S IThus, we normalize the model. Without loss <strong>of</strong> generality let s , i ,N Np PN,Th andNa ANTherefore, the normalized system can be calculated as followsS sNdSdtdNsdtdsNdtds 1dt NdS dtdN sdt dsdt c1 1is c33hs a 1 isI iNdIdtdNidtdiNdtdi 1dt NdI dtdN idt didt c11is c33hs 1 i a 1 iiP pNdPdtdNpdtdpNdt
20dp 1dt NdP dtdN pdt dpdt 1 i a 1 ipH hNdT dN dh h Ndt dt dtdh 1 dT dN hdt N dt dt dhdt 2 i m p a k a 1 ihA aNdAdtdNadtdaNdtda 1dt NdA dtdN adtdadt 1 1 11 2 i m p kh a ia
21Now, the system be written as followsdsdt c11is c33hs a 1 is,didt c11is c33hs 1 i a 1 ii,dp 1 i a 1 ip,dt (3.3)dh 2 i m p a k a 1 ih,dt da 1 1 2 i 1 m p kh a 1 ia,dt Such thats i p h a 1.3.2 Positivity <strong>of</strong> SolutionsFor the model (3.3) to be epidemiological meaningful and well posed, we need toprove that all state variables are non-negative t 0.Theorem 1 Let , , , , s i p h a s i p h a 5, , , , : 1, then the solutionss t i t p t h t a t <strong>of</strong> the system (3.1.3) are positive t 0.To prove the theorem, we will use differential equations <strong>of</strong> the system (3.3).Using the 1 st equation we have
22ds s(3.4)dtdss dtFinding the integrating factor, IF dt e etd setet dtIntegrating both sides we get 1s t ce tt 0, s t s o . s o 1cApplying initial conditions: When s t 1 s 0 1 e tWhen t , s t 1There fore, 0 s t 1Similarly, using the second equation <strong>of</strong> the system (3.3) we havedidt (3.5)didt 0
23 dtIF e e tddt ie 0Integrating both sides lead to t ce i tApplying initial conditions: at 0, 0 . 0t i t i i c 0 i t i e t , i t 0tTherefore,it 0.Also in the third equation <strong>of</strong> the system (3.3) we havedp p(3.6)dtdp dtpIntegrating both sides, we get 0 p t p e tApplying initial conditions; at t 0, pt p0
24When t , p t 0Similarly, using fourth equation <strong>of</strong> the system (3.3) we havedh k h(3.7)dtdh k dthIntegrating both sides, we get k t 0 h t h e Applying initial conditions; at t 0, ht h0When t , h t 0Finally, using fifth equation <strong>of</strong> the system (3.3) we haveda a(3.8)dtda dtaIntegrating both sides, we get 0 a t a e tApplying initial conditions; at t 0, at a0When t , a t 0
253.3 Stability Analysis <strong>of</strong> the Model.In this section, we present the results <strong>of</strong> stability analysis <strong>of</strong> the equilibrium points.3.4 Equilibrium Points <strong>of</strong> the ModelThe model (3.3) has two non negative equilibrium points which are; the disease freeequilibrium point E0, and endemic equilibrium point*Eds di dp dh daAt equilibrium point 0,dt dt dt dt dthence the following systems <strong>of</strong>equations is solved for equilibrium points.0 c1 1is c33hs a 1 is 0 c11is c33hs 1 i a 1 ii0 1 i a 1 ip0 2 i m p a k a 1 ih 0 11 2 i 1 m p kh a 1 iaFor the disease free equilibrium point i p h a 0,when substituted above, thesystem <strong>of</strong> equations is reduced to s 0 , hence s 1.There fore, the disease free equilibrium E0is 1,0,0,0,0,
26The linear stability <strong>of</strong> E0can be established by its basic reproduction number. It isdetermined by using next generation method on the equation (3.3) in the form <strong>of</strong>matrices F andV .Let Fibe the rate <strong>of</strong> appearance <strong>of</strong> new infection in compartmentVibe the transfer <strong>of</strong> individuals out <strong>of</strong> compartment by another meansx0be the disease free equilibriumR0is the largest eigenvalue <strong>of</strong>Fi x Vi x 0 0 x xj j 1(3.9)3.5 Computation <strong>of</strong> the Basic Reproduction Number, R0The basic reproduction number R0is defined as the effective number <strong>of</strong> secondaryinfectious caused by typical infected individual during his interred periods <strong>of</strong>infectiousness (Diekman et al., 1990). It is obtaining by taking the largest (dominant)Eigen value (spectral radius) <strong>of</strong>RFi x Vi x 0 00 x xj j 1Where;FFixx j0, and VVixx j0
27c110 c330 0 0 0 0F and 0 0 0 0 0 0 0 0V 1 011 m1120 m00 k k0 0 R0 F V1R0c11 2c3 32 2 2 2 1m 1m 1 2 k (3.10)Thus if R 1 0, the infection triggers an epidemic otherwise its prevalence is zero i.e.for R 01 . From the solution, it is noted that <strong>with</strong> an increase in R0, which can beviewed as a function <strong>of</strong> c , the number <strong>of</strong> sexual partners . the number <strong>of</strong> invectivesincreases which in turns increases the AIDS patient population. Thus in order to keepthe spread <strong>of</strong> the disease at minimum, the number <strong>of</strong> sexual partners should berestricted.
283.6 Local Stability <strong>of</strong> the EquilibriaTheorem 2.The disease free equilibrium <strong>of</strong> the system is locally asymptoticallystable if R 01 and unstable if R 1 0.Now to determine the local stability <strong>of</strong> E0, the following variational matrix iscomputed corresponding to equilibrium point E0dsdt c1 1is c33hs a 1 is D s, i, p, h,adidt c11is c33hs 1 i a 1 ii F s, i, p, h,adp 1 i a 1 ip G s, i, p, h,adt (3.1.1)dh 2 i m p a k a 1 i h L s, i, p, h,adt da 12 dt1 i 1 m p kh a 1 ia M s, i, p, h,aJacobean Matrix <strong>of</strong> the system (3.3) is given by
29J0 D E0 D E0 D E0 D E0 F E0 s i p h a F E0 F E0 F E0 F E0 F E0 s i p h aG E0 G E0 G E0 G E0 G E0 s i p h a L E0 L E0 L E0 L E0 L E0 s i p h aM E0 M E0 M E0 M E0 M E0 s i p h a V0 1c1 1 1 0 c3 3 c 2 m k m k 0 c11 1 0330 0 0 0 0 0 11 21The characteristic equation corresponding to V0is given byf4 3 2 a a a a 0, (3.1.2)1234Wherea 4 k c 1 1 1 a c k k k2 2 3 33 k c k k 3 2 1 1
302a3 k 2 k 2 2 2 k 3c k k k 3 22 2 2 21 12 2 c m k k3 3 2 2 2 1 1 2 2 2 k 3 2 3 2 2 2 k k 2 2 k 4 k k k k 2 2 3 2 22 2 2 3 2 3 4 3 3 .2 2 3 2 2 a k k k k 2 3 2 2c1 1k k k k c232 2 2 2 1m 1m13Thus by Routh-Hurwitz criteria, E0is locally asymptotically stable as it can be seenfora , a 0, a 0, a 0, a a a 0, and a a a a a a 0.102 3 4 1 2 32 22 2 3 3 1 4Thus, using a 40 , 2 2 k 3 k 2 k 2 k 2 3 2 2c1 1k k k k
31 c2 mm 0332 2 2 2 111This will lead to 2 2 k 3 k 2 k 2 k 2 2 3 2 2c1 1k k k k c232 2 2 2 1m 1m13Hence,2c1 c33 2 12 2 2 1m 1m 1 1 2 k k Therefore, R 1 0.This pro<strong>of</strong>s the Theorem above i.e. The disease free equilibrium <strong>of</strong> the system islocally asymptotically stable if R 01 and unstable if R 1 0.3.7 The Endemic Equilibrium and Local StabilityThe endemic equilibrium point <strong>of</strong> the model (3.3) is given by E * s, i * , p * , h * , aTo obtain an endemic equilibriumthe model. .*E <strong>of</strong> this model, we set to zero each equation in
32Then by solving the system <strong>of</strong> equations in (3.3) we express each equilibrium pointin terms <strong>of</strong> i **and a at steady state, we get c1 1is c33hs a 1 is...............................................i c1 1is c33hs 1 i a 1 ii..............................ii 1 i a 1 ip............................................................iii 2 i m p a k a 1 ih.........................................iv1 i 1 m p kh a 1 ia............v1 2Add equation s* i and ii to get the value <strong>of</strong>1 1* * a 1 i *s ,we get i a i i* * * **Using equation iiito get value <strong>of</strong> p ,p**1i ,* a*1 iSolve equation iv and v to get the value <strong>of</strong>* *h and a we get;*ha** * * *1 1 2 i 1 m1 i k 2 i m 1i k
33Where: a 1 i* * k a 1 i* * a* 1 i* and** * *1 12 i 1 m 1i k 2i m1i * * 2 i m 1i kThe values <strong>of</strong> i * are in the form <strong>of</strong> polynomiali A i A i A i A i Ai A (3.1.3)* *5 *4 *3 *2 *5 4 3 2 1 00After some algebraic calculation, the expression can be reduced as:Ai Bi 0(3.1.4)*2 *Where, * *A k a a , 3 c c a 2c a 2c a c k c ka3 * * 2 * *1 1 1 1 1 1 1 1 1 1 1 1c a c k c a c k 2c a c * 2 * *1 1 1 1 1 1 1 1 1 1 3 3 2
34c m c m a c c m c *3 3 1 3 3 1 3 3 2 3 3 1 3 3c a c c k a 2c ka c c * 2 2 * *3 3 2 3 3 2 1 1 1 1 3 3 2 3 3 2c 2c a c a c a c a* * * *3 3 1 3 3 2 3 3 1 3 3 3 3 22 2 c c 3c a c k c k a 3c a2 * 2 * *1 1 1 1 1 1 1 1 1 1 1 12 2 2 c c a c a c a c c 2 * * * 2 21 1 1 1 1 1 1 1 1 1 1 1 c2 *33 2 a .B k a* 4 3 * 3 3 3 2 * 3 2 2 * 3 k 4 a k 4 a 3 a 2 2 3 4 k 3 k a 6 a 6 a 4 a a2 2 2 * 2 * 2 * * *3 4 3 4 a a k a k ka* 4 4 4 * * 3 2 *3 3 4 a 2 a a a c 3 k a 3 * 2 * * * 4 2 * 51 13 2 4 2 ka 2 a k 4 a k a a* * * * *2 2 2 3k a k 3 a 3 a k a c * 2 2 * * * 31 1
352 3 c c 3c a 3c a c k c a3 3 3 * 2 * 3 *1 1 1 1 1 1 1 1 1 1 1 13 2 2 2 a 2 k a 3 k a 3 a 3 a 3 a* 2 * * * * 2 2 *2 2 3 a k 3 a 3 a k a2 * 2 2 2 2 * * * 6 *2*23 2 *233 3 2 3 3 1 a a c a c m c c k c k c a c a c a2 * *3 3 1 1 1 1 1 1 1 1 3 32 2 c a c a c a c a c a2 * * * * 2 *3 3 2 3 3 1 1 1 1 1 1 1 2c k c m a c c m c a2 * 2 2 *1 1 3 3 1 3 3 2 3 3 1 1 1c k a 2c a c a 2c a 2c ka* 2 * * 2 * *1 1 1 1 3 3 2 3 3 2 1 1 2c k a c a 2 ka c c * * * 2 21 1 3 3 2 3 3 2 3 3 1c 2c a 2c a c k c c 2 2 * 2 2 * 2 2 23 3 1 1 1 1 1 1 1 1 1 14 2 3 4 4* 3 * 2 * * * c33 2 a 10 a 10 a 5 a k a2 3 2 3 6 k a 5 a 4 a 6 a k a3 2 * 4 * * 2 * *3 2 5 3 k 4 3 ka * 4 k a * 4 3 a * 4 3 k a * a3 3 3 a a k a 3 a 3 ka* * * 2 2 *
363.8 Existence <strong>of</strong> Forward BifurcationWe will analyse the local asymptotic stability <strong>of</strong> endemic equilibrium by using thetheorem <strong>of</strong> Centre manifold (Gumel et al., 2008). The linearizion matrix has at leastone Eigen value <strong>with</strong> zero real part. Also we shall describe the possibility <strong>of</strong> forwardbifurcation from the non hyperbolic equilibrium. To describe it, consider a generalsystem <strong>of</strong> ODEs <strong>with</strong> F . This theory is convenient by changing variables.Consider s x1 , i x2, p x3, h x4,a x5. By using vector notation1 2 3 4 5TX x , x , x , x , x in the model (3.3) can be written in the formdXdtF X , where by F f , f , f , f , f 1 2 3 4 5Tas follows:dxdt1 f c x x c x x x 1 x x1 1 1 2 1 3 3 4 1 5 2 1dxdt21 1 f c x x c x x x x x x2 1 1 2 1 3 3 4 1 2 5 2 2dxdt3 f3 1 x2 x5 1 x2 x3(3.1.5)dxdt4 f x m x x k x 1 x x4 2 2 3 5 5 2 4dxdt51 1 1 f x m x kx x x x5 1 2 2 3 4 5 2 5The Jacobian <strong>of</strong> the system (3.15) at the DFE is given by,
37J E0 1c1 1 1 0 c3 3 c 2 m k m k 0 c11 1 0330 0 0 0 0 0 11 21(3.1.6)WhereR02c11c332 mm 1 22 2 2 11 kSupposesolve for*1 is the chosen bifurcation parameter and if we consider R0 1*1 givesand* 2 2c1 k k k k c 3 3(3.1.7)Where m m 22 2 2 2 1 1 1The system <strong>of</strong> the transformed equation <strong>with</strong>*1 has a simple zero eigen values.Hence the Center Manifold theory can be used to analyze the dynamic <strong>of</strong>dXdt , , , , 1 2 3 4 5T* F X F f f f f f near . It can be shown that the Jacobian1dXT 1 2 3 4 5atdt<strong>of</strong> F X F f , f , f , f , f 1* has right eigen vector associated<strong>with</strong> the zero eigen values by w w , w , w , w , w where1 2 3 4 5T
38 1 c33 c1 1 c33m 1 c33 2w w1 2c33w w13 2w c 1 1 14w2c33 c1 1 1 c33m 1 c33 2w w5 2c33w2 0,Where k 1 11 c The right eigenvector <strong>of</strong> J E 0 associated <strong>with</strong> the zero eigenvalues at*1 isgiven by u u u u u u , , , , , where1 2 3 4 5Tu1 0
39um 1 m 1 1 2 1 2 u2 4um 1m u3 4u u5 4u4 0,Theorem 3: (Castillo-Chavez and Song, 2004) Consider the following generalsystem <strong>of</strong> ordinary differential equations <strong>with</strong> a parameter such thatdxdtf ( x,),f:nn2 n and f c .Where 0 is an equilibrium point <strong>of</strong> the system (that is 0, 0f for all ) and f x x j 1. D f 0,0 i 0,0is the linearization matrix <strong>of</strong> the system aroundthe equilibrium 0 <strong>with</strong> evaluated at 0 .2. Zero is a simple eigenvalue <strong>of</strong> and all other eigenvalues <strong>of</strong> havenegative real parts.3. Matrix has a right eigenvectors and left eigenvector q correspondingto zero eigenvalues.
404. Let fkbe thethk component <strong>of</strong> f anda n2 fx xk ukij 0,0, (3.1.8)k, i, j1i jb n kukj 0,0. (3.1.9)k , j12 fxjThe local <strong>dynamics</strong> <strong>of</strong> the system around the equilibrium point is totally determinedby the signs <strong>of</strong> a and b particularly, if a 0 and b 0 then a backward bifurcationoccurs at 0 .1. a 0, b 0. When 0 <strong>with</strong> | |1,0 is locally asymptotically stable, and thereexist a positive unstable equilibrium; when 0 1,0is unstable and there exist anegative and locally asymptotically stable equilibrium;2. a 0, b 0 . When 0 <strong>with</strong> | |1,0 is unstable; when 0 1,0is locallyasymptotically stable, and there exist a positive unstable equilibrium;3. a 0, b 0. When 0 <strong>with</strong> | |1,0 is unstable and there exist a locallyasymptotically stable negative equilibrium; when 0 1,0is stable, and positiveunstable equilibrium appears;4. a 0, b 0. When changes from negative to positive, 0 changes its stabilityfrom stable to unstable. Correspondingly a negative unstable equilibrium becomespositive and locally asymptotically stable.
41Calculation <strong>of</strong> Bifurcation Parameters a and bFrom model (3.15), the associated none zero partial derivatives <strong>of</strong> F at the diseasefree equilibrium are given by, f f f f f f f f 0, 2 2 2 2 2 22 22 2 3 3 4 45 52 2x2 x2 x5 x2 x3 x3 x5 x2 x4 x4 x5 x2 x5 x5 f f f f 2 1 , , 1 , , 2 22 22 23 32 x2 x2 x5 x2 x3 x3 x5 f f f f 1 , , 1 , 2 ,x x x x x x x2 22 24 45 5 22 4 4 5 2 5 5It follows from above expressions that f f fa u w w u w w u w w u w w2 2 222 3 452 i j 3 i j 4 i j 5 i jxix jxix jxi x jxi xj (3.2.0)f2 u 2 w2 w5 2 1 w 2 u3 w3 w5 1 w2w31 2 21u4 w4w5 w2w4 u5 w5 w2w5 There fore a 0, ifq w3w5 2 3u11 w w 3Where q1 u w w 2 1 w u w w 1 w w u 2 w 1 w w2 22 2 5 2 4 4 5 2 4 5 5 2 5
42Hence, a 0, if1 c3 3m 1 c33 2 c33 11 c33 m 1mWhere c33m 1 c3 3 2 2 c33m 1 c33 2 c3 3 c33 c3321 m m 1 1 1 2 1 2 c331 c m c 33 1 33 2 c 3 3 c m c c333 3 1 3 3 2 2 1 For the sign <strong>of</strong> b it can be shown that the associated non vanishing partial derivatives<strong>of</strong> f is2 f2x1 2 c1So thatf 2221x(3.2.1)ib u wi u2w2c1
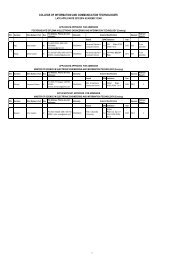
43m 1 m 1 1 2 1 2 c1 0,Therefore, b 0Hence, we have established the following result. Since b 0 and a 0 if theinequality satisfies, then there exists a forward bifurcation.Figure 3.2 Forward Bifurcation <strong>of</strong> the model (3.3).3.9 Global Stability <strong>of</strong> the Endemic EquilibriumTheorem 4. If the endemic equilibrium*E exist, then it is globally asymptoticallystable provided that R0 1.Consider the following positive definite definite function about*E
44* * ** * * * ** s * i * p V s , i , p , h , a s s slog i i i log p p p log s i p * ** h * a h h hlog a a a log h a (3.2.2)By direct calculation <strong>of</strong> the derivative <strong>of</strong> V along the solution <strong>of</strong> (3.3) can be writtenas dt s dt i dt p dt h dt a dt* * * * *dV s s ds i i di p p dp h h dh a a daBut from the model (3.3).dsdt c is c hs a 1 is1133didt1 i a c is c hs 11133 iidpdt i a 1 ip1dh 2i mpa k a 1 ihdtdadt i 1 mp kh a 111 2iaIt can now be written as*dV s s c1 1is c33hs a 1 isdt s
45* i i c1 1is c33hs 1 i a 1 iii * p p 1 i a 1 ipp * h h 2i m p a k a 1 ihh a a a*1 1 1 i m p kh a i a1 2Therefore,* * * * *substitute s s s , i i i , p p p , h h h and a a a , aftersome algebraic calculations we get2 2* *s s i i* *11 33 11 dV c i c h a i i c s adt s i2* p p h h2* * a i i a i i p * 2a a i i p h h i i c h i i mpa i i p h h*3 * * * ** * * * *3 3 1 2hh a a a a a a a i i i p m p kh iih a a a a a a* * * * * * ** * * *1 23i 3 i c h i i m p a a 3 a i2 *2 2 *23 3 1 2 i i p mp kh* * *1 2
46* *s s i i 2 2* * * c11i c3 3h a i i c1 1s as * * p p h h 2 2* * * * a i i k a i ip * 2a a s i p h a s i p h* * * **i i c3 3h 1i2ihih h i a a a am p a i i ih h i a a a a* * * *3 * * ** *31 2a a a p m p kh ii aa i i c h ia a a* * ** * * * * * *3 3 33 3 1 i m p a i i i p mp kh* * * * *2 1 2Hence, the sufficient condition for dVdtto be negative definite is that 0.Where, 2 2* *s s i i* *11 33 11 c i c h a i ic s asi2* p p h h2* * a i i a i i p * 2a a i i p h h i i c h i i mpa i i p h h*3 * * * ** * * * *3 3 1 2hh a a a a a a a i i i p m p kh iih a a a a a a* * * * * * ** * * *1 23
47i 3 i c h i i m p a a 3 a i2 *2 2 *23 3 1 2 i i p mp kh* * *1 2And * *s s i i 2 2* * * c11i c33h a i i c1 1s as i* * p p h h 2 2* * * * a i i k a i ip * 2a a s i p h a s i p h* * * **i i c3 3h 1i2ihh h i a a a am p a i i ih h i a a a a* * * *3 * * ** *31 2a a a p m p kh ii aa i i c h ia a a* * ** * * * * * *3 3 33 3 1 i m p a i i i p mp kh* * * * *2 1 2dVdVTherefore, 0, if and 0, ifdtdts s i i p p h h* * * * , , , anda* a . * * * * * dV Therefore, the largest compact invariant set in s , i , p , h , a : 0is thedt singleton E* ,where*E is endemic equilibrium <strong>of</strong> the normalized model system
48(3.3). By LaSalle’s invariant principle, then it implies that*E is globallyasymptotically stable in if . This completes the pro<strong>of</strong> <strong>of</strong> theorem ( 4).
49CHAPTER FOURTHE NUMERICAL SIMULATIONS OF THE MODEL4.1 Model SimulationTo study the dynamical behaviour <strong>of</strong> the model (3.3) numerically, the system isintegrated by using Runge-Kutta method using the following set <strong>of</strong> parameter values: 0.3, 0.2, 0.1, 1 0.4, 3 0.05, 1 0.2, 2 0.01, k 0.08, 0.9,c1 3, c3 1,m 0.4 , 0.4, 0.6, 1With initial valuess 0 0.5, i0 0.3, p0 0.12, h0 0.07 , a 0 0.01.The endemic equilibrium values are computed as shown graphically in figure 4.1(a) -4.1(d). It is shown thatsusceptible population s * .* * *i , p , h and*a is plotted against the proportion <strong>of</strong>
50Figure 4.1(a). Endemic equilibrium <strong>of</strong> proportion <strong>of</strong> infectives <strong>with</strong> Susceptible.Figure 4.1(b). Endemic equilibrium <strong>of</strong> proportion <strong>of</strong> Pre-AIDS population
51Figure 4.1(c). Endemic equilibrium <strong>of</strong> proportion <strong>of</strong> treated classProrportion <strong>of</strong> Aids patients0.20.180.160.140.120.10.080.060.040.021234Equilibrium point00.45 0.5 0.55 0.6 0.65 0.7 0.75Proportion <strong>of</strong> SusceptiblesFigure 4.1(d). Endemic equilibrium <strong>of</strong> proportion <strong>of</strong> AIDS populationWe see from the figures that for any initial start, the solution curve tend toequilibrium E * . Hence, we infer that the system (3.3) may be globally stable about*this endemic equilibrium point E . The computed values are:*s 0.6028, i * 0.2433,*p 0.2284,*h 0.04236,*a 0.08929 .
52The results <strong>of</strong> numerical simulation are shown graphically in Figures 4.2. In figure4.2(a) the distribution <strong>of</strong> proportion <strong>of</strong> population <strong>with</strong> time is shown in differentclasses <strong>with</strong> neither new infected children into the population nor recruitments i.e. 0 and 0.It is seen that in the absence <strong>of</strong> vertical transmission into thecommunity, the proportion <strong>of</strong> susceptible population decreases continuously as thepopulation is closed which results in an increase in proportion <strong>of</strong> infective populationfirst and then it decreases as all infectives subsequently develop full blown AIDS andthe die out by natural or disease-induced death rate. The proportion <strong>of</strong> treated class isincrease continuously since the total population being constant in this case.Figure 4.2(b) shows the variation <strong>of</strong> proportion <strong>of</strong> population in all classes <strong>with</strong> bothrecruitment <strong>of</strong> susceptibles and fraction <strong>of</strong> new born children which are infected atbirth. It is found that susceptible first decrease <strong>with</strong> time after using ARVs theyprolong life time they increase and then reaches its equilibrium position. Since due tovertical transmission from infectives, susceptible population increase continuouslytherefore infection becomes more endemic, following that R0 1.
53Figure 4.2(a) Variation <strong>of</strong> population in different classes for 0 and 0.Figure 4.2(b) Variation <strong>of</strong> population in different classes for 0.1and 0.2.
54The role <strong>of</strong> vertical transmission in the model i.e. the rate <strong>of</strong> recruitment <strong>of</strong> infectedchildren directly into infective class is explicitly shown in figures 4.3(a) - 4.3(c). It isseen that in figure 4.3(a) as the rate <strong>of</strong> infected children born increase, theproportion infective population also increases. It may be noted here that the birth <strong>of</strong>infected children make the infective population increase. In figure 4.3(b) if weincrease the value <strong>of</strong> the proportion <strong>of</strong> AIDS population decreases <strong>with</strong> time thenit increases until reaches its equilibrium position. Thus, if the birth <strong>of</strong> infectedchildren is controlled by <strong>treatment</strong>, the overall infective population will remain undercontrol. This will help in reducing the AIDS population. In 4.3(c) it is found that asthe rate <strong>of</strong> infected children born increases, the treated population decreases.Figure 4.3(a) Variation <strong>of</strong> infected population for different values <strong>of</strong> .
55Figure 4.3(b) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> .Figure 4.3(c) Variation <strong>of</strong> Treated class for different values <strong>of</strong> .Figure 4.4(a) – 4.4(c) shows the impact <strong>of</strong> recruitment rate for Susceptibles, Treatedclass and AIDS patients for different values <strong>of</strong> . It is seen that as recruitment rate
56increase the susceptible population increase compared rather than decrease the rate .Since the inflow <strong>of</strong> susceptible increase, but the treated population and AIDSpopulation are decreases <strong>with</strong> time till it reach equilibrium and then decreasecontinuously due to <strong>treatment</strong> in the dynamic <strong>of</strong> HIVFigure 4.4(a) Variation <strong>of</strong> Susceptible for different values <strong>of</strong> .
57Figure 4.4(b) Variation <strong>of</strong> Treated population for different values <strong>of</strong> .Figure 4.4(c) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> .
58Figures 4.5(a) – 4.5(d) depict the variation <strong>of</strong> infectives, pre-AIDS, Treatment andAIDS population respectively <strong>with</strong> time for different values <strong>of</strong> movement rate <strong>of</strong>individuals from infective class to pre-AIDS, Treatment or AIDS depending uponviral counts. It is seen that <strong>with</strong> increase in the value <strong>of</strong> movement rate , theinfected population decreases which intern increase the Treated population. Also ifwe increases movement rate , the Pre-AIDS and AIDS population decreases <strong>with</strong>time until it reach the equilibrium stabilise the model.Figure 4.5(a) Variation <strong>of</strong> Infective population for different values <strong>of</strong> .
59Figure 4.5(b) Variation <strong>of</strong> pre-AIDS population for different values <strong>of</strong> .Figure 4.5(c) Variation <strong>of</strong> Treated class for different values <strong>of</strong> .
60Figure 4.5(d) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> .Figure 4.6(a) – 4.6(b) shows the Variation <strong>of</strong> population in the classes <strong>with</strong> fraction<strong>of</strong> movement rate from infectious class . It is seen that from the figures when 1increases, the pre-AIDS population also decreases continuously it might be <strong>of</strong><strong>treatment</strong> which is provided to the patients, but for the AIDS class this is different, itis found that as 1increases, the AIDS population decreases <strong>with</strong> time then reachesits equilibrium and start to increase. This is caused by ARVs it prolonging the lifespan, then the patient join full blown AIDS, therefore disease persist. Also it is foundfrom the graph that as 2increases Treated population initially increase, as timegone then it decreases, but in AIDS patients they decreases continuously up toequilibrium then they increase because disease still exist.
61Figure 4.6(a) Variation <strong>of</strong> pre-AIDS population for different values <strong>of</strong> 1.Figure 4.6(b) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> 1.
62Figure 4.6(c) Variation <strong>of</strong> Treated population for different values <strong>of</strong> 2.Figure 4.6(d) Variation <strong>of</strong> AIDS population for different values <strong>of</strong> 2.Figure 4.7(a) – 4.7(d) predict the Variation <strong>of</strong> the contact rates <strong>of</strong> susceptibles <strong>with</strong>infectives 1and susceptibles <strong>with</strong> treated class 3in the susceptibles andinfectives population. The figures shows that as the contact rate 1increase the
63susceptibles decrease, infectives class decrease and <strong>treatment</strong> increase. Also as thecontact rates <strong>of</strong> susceptible <strong>with</strong> treated population 3increase the susceptibleinitially increase <strong>with</strong> time and then it reach its equilibrium position, but this differ toinfectives as 3increases, the infectives decreases <strong>with</strong> time than reach itsequilibrium and increases.Figure 4.7(a) Variation <strong>of</strong> Susceptibles population for different values <strong>of</strong> 1
64Figure 4.7(b) Variation <strong>of</strong> Infectives population for different values <strong>of</strong> 1Figure 4.7(c) Variation <strong>of</strong> Susceptibles population for different values <strong>of</strong> 3
65Figure 4.7(d) Variation <strong>of</strong> Infectives population for different values <strong>of</strong> 3Figure 4.8(a) – 4.8(b) shows the variation <strong>of</strong> susceptibles and infectives populationfor different values <strong>of</strong> number <strong>of</strong> sexual partners <strong>of</strong> susceptibles <strong>with</strong> infectives c 1,and between susceptibles <strong>with</strong> treated population c 3. It is seen that as the number <strong>of</strong>sexual partners <strong>of</strong> susceptibles <strong>with</strong> infectives c1increases <strong>with</strong> time, susceptiblesdecreases continuously and infectives increases continuously. Also it is seen that ifthe number <strong>of</strong> sexual partners <strong>of</strong> susceptibles <strong>with</strong> treated population c3increases<strong>with</strong> time, susceptibles first increase than decreases <strong>with</strong> time as shown in fig. 4.8(c)due to loss <strong>of</strong> immune. But for infectives it seen that as c3increases also infectivesincreases, thus in order to reduce the spread <strong>of</strong> the disease, the number <strong>of</strong> sexualpartners as well as unsafe sexual interaction <strong>with</strong> an infective is to be restricted.
66Figure 4.8(a) Variation <strong>of</strong> Susceptibles population for different values <strong>of</strong> c 1Figure 4.8(b) Variation <strong>of</strong> Infectives population for different values <strong>of</strong> c1
67Figure 4.8(c) Variation <strong>of</strong> Susceptibles population for different values <strong>of</strong> c3Figure 4.8(d) Variation <strong>of</strong> Infectives population for different values <strong>of</strong> c3Figure 4.9(a) and 4.9(b) shows the variation <strong>of</strong> <strong>treatment</strong> rates in treated class andAIDS population. It is found that if <strong>treatment</strong> rates is zero the disease increase <strong>with</strong>
68time whereas <strong>treatment</strong> population decreases. Also the graphs shows that as the rates<strong>of</strong> <strong>treatment</strong> increases, the AIDS patients decreases due to <strong>treatment</strong> measures whichincreases the immune system and prolong life <strong>of</strong> AIDS population, therefore thisincreases the treated class.Figure 4.9(a) Variation <strong>of</strong> AIDS patients for different values <strong>of</strong> k and .Figure 4.9(a) Variation <strong>of</strong> AIDS patients for different values <strong>of</strong> k and .
69In figure 4.10 the effect <strong>of</strong> disease induced death rate is shown and it is found thatas increases, the population <strong>of</strong> AIDS patient’s decreases. It is found that the AIDSinduced death rate , can be controlled by provide antiretroviral drugs (ARVs) toAIDS patients or by advising AIDS patients to follow healthy regulation about theAIDS disease. From the figures, it can also be seen that the respective populationsare tending to the equilibrium level. This has also been observed for different initialvalues <strong>of</strong> the variables. Hence the endemic equilibrium*E is globallyasymptotically stable for the above set <strong>of</strong> parameter value.Figure 4.10 Variation <strong>of</strong> AIDS populations for different values <strong>of</strong> .
70CHAPTER FIVEDISCUSSION, CONCLUSION AND FUTURE WORK5.1 DiscussionIn this study, a non linear model has been proposed and analyzed to study thedynamic <strong>of</strong> HIV/AIDS model <strong>with</strong> <strong>treatment</strong> and vertical transmission. The diseasefree and endemic equilibria are obtained and their stability are investigated. Anumerical study <strong>of</strong> the model has been conducted to see the impact <strong>of</strong> certain keyparameters on the spread <strong>of</strong> HIV disease.It is observed that an increased ininfectives through vertical transmission would lead to increase the population <strong>of</strong>infectives which in turn increase the pre-AIDS, treated class and AIDS population.AIDS can be eradicated after some fixed years if we can reduce the value <strong>of</strong> R0toless than unity i.e. R0 1. In the case R0 1 all the infected classes which areinfectives, pre-AIDS and AIDS populations decrease <strong>with</strong> time. When this attained,immediately the treated class increases since the infective class start decreasing, andthen follows the pre-AIDS class and finally the AIDS can be eradicated.The following measures can be exercised in order to decrease the value <strong>of</strong> R0to beless than one so as to decrease the infections, which can lead on eradication <strong>of</strong> theHIV/AIDS disease.
71Use <strong>of</strong> Antiretroviral DrugsIn many cases, an HIV-infected individual may be invaded by a host <strong>of</strong> commondiseases ranging from very strong bacterial and viral infections to mild sicknesses.Since the infected person may be invaded by many infections simultaneously, it isnoted that a single drug may not be sufficient to clear such an attack. As a result, acouple <strong>of</strong> drugs recombinants that are particularly made to treat the HIV/AIDSpatients <strong>of</strong> combinations <strong>of</strong> attacks have been developed.Women who have reached the advanced stages <strong>of</strong> HIV disease require combinations<strong>of</strong> antiretroviral drugs for their own health. This <strong>treatment</strong>, which must be takenevery day for the rest <strong>of</strong> women’s life, is also highly effective at preventing motherto-childtransmission (PMTCT).The most effective PMTCT therapy involves a combination <strong>of</strong> three antiretroviraldrugs taken during the later stages <strong>of</strong> pregnancy and during labour. This therapy isessentially identical to the <strong>treatment</strong> taken by HIV positive people for their ownhealth; except that it is taken only for a few months and the choice <strong>of</strong> drugs may beslightly different. Triple therapy is usually recommended to women in developedcountries, and is becoming more widespread in the rest <strong>of</strong> the world; this is reflectedby WHO 2009 Guidelines.Effective Prevention <strong>of</strong> Vertical transmissionEffective prevention <strong>of</strong> mother-to-child transmission (PMTCT) requires a three-foldstrategy (UNAIDS/WHO, 2005).
72Preventing HIV infection among prospective parent making HIV testing and otherprevention interventions available in services related to sexual health such asantenatal and postpartum care.Avoid unwanted pregnancies among HIV positive women-providing appropriatecounselling and support to women living <strong>with</strong> HIV to enable them to make informeddecisions about their reproductive lives.Preventing the transmission <strong>of</strong> HIV from HIV positive mothers to their infantsduring pregnancy, labour, delivery and breastfeeding.Integration <strong>of</strong> HIV care, <strong>treatment</strong> and support for women found to be positive andtheir families.Also it is needed to control the vertical transmission <strong>of</strong> HIV by suppressinghorizontal transmission; including condom use and other safer sexual contact. Fromnumerical simulation it is found that an increase in the number <strong>of</strong> sexual partnersfurther reduces the susceptible population by way <strong>of</strong> spreading the disease. Thus inorder to reduce the spread <strong>of</strong> the disease, the number <strong>of</strong> sexual partners should berestricted as well, and consequently the equilibrium values <strong>of</strong> infective, treated andAIDS population can be maintained at desired levels.Cesarean SectionsA cesarean section is an operation to deliver a baby through its mother’s abdominalwall. When a mother is HIV positive a cesarean section may be done to protect thebaby from direct contact <strong>with</strong> her blood and other bodily fluids. There are indicationsthat cesarean birth decreases the risk <strong>of</strong> mother-to-child transmission (Newell, 1998).
73If the mother is taking combination antiretroviral therapy then a cesarean section will<strong>of</strong>ten not be recommended because the risk <strong>of</strong> HIV transmission will be very low.Cesarean delivery may be recommended if the mother has a high level <strong>of</strong> HIV in herblood, but the procedure is seldom available and/or safe in resource poor settings(Dabis, F., 2002).Safer Infant Feeding to HIV Positive MothersA number <strong>of</strong> studies have shown that the protective benefit <strong>of</strong> drugs is diminishedwhen babies continue to be exposed to HIV through breastfeeding (Lu L. etal.,2009). Mother <strong>with</strong> HIV are advised not to breastfeed whenever the use <strong>of</strong> breastmilk substitutes (formula) is acceptable, feasible, affordable sustainable and safe.For HIV positive women who choose to breastfeed, exclusive breastfeeding isrecommended for the first months <strong>of</strong> an infant’s life and should be discontinued oncean alternative form <strong>of</strong> feeding becomes feasible (UNAIDS, 2005). Mixed feeding isnot recommended because studies suggest it carries a higher risk than exclusivebreastfeeding. This is because mixed feeding damages the lining <strong>of</strong> the baby’sstomach and intestines and thus makes it easier for HIV in breast milk to infect thebaby. However, since ARVs have been more available, the risk from mixed feedingis reduced. Indirect evidence suggest that keeping the period <strong>of</strong> transmission fromexclusive breastfeeding to alternative feeding as short as possible may reduce the risk<strong>of</strong> transmission. Unfortunately, the best duration for this is not yet known and mayvary according to the infant’s age and/or the environment (UNAIDS 2005).
745.2 ConclusionsIn this research, a non-linear <strong>mathematical</strong> model is proposed and analyzed to studythe transmission <strong>of</strong> HIV/AIDS in a population <strong>of</strong> varying size <strong>with</strong> <strong>treatment</strong>s andvertical transmission under the assumption that due to sexual interaction <strong>of</strong>susceptibles <strong>with</strong> infectives, the infected babies are born to increase the growth <strong>of</strong>infective population directly. It is assumed that people in pre-AIDS and AIDS classesare exposed and incapable <strong>of</strong> producing children. By analyzing the model, we havefound a threshold parameter R . It is noted that when 0R0 1 then the disease dies outand when R0 1 the disease becomes endemic. The model has two non-negativeequilibrium namely the disease-free equilibrium, * * * * * *equilibrium E 1,0,0,0,00and the endemicE s , i , p , h , a . It is found that the disease-free equilibrium E0islocally asymptotically stable if R0 1 and for R0 1 it is unstable and the infectionis maintained in the population. The endemic equilibrium E * , which exist only whenR0 1 , is always locally asymptotically stable. The equilibrium is also shown to beglobally asymptotically stable under certain conditions. It is found that an increase inthe rate <strong>of</strong> vertical transmission leads to increase the population <strong>of</strong> infectives whichin turn increases the pre-AIDS and AIDS population. Thus, the vertical spread <strong>of</strong> thedisease should be controlled by effective <strong>treatment</strong> or promoting the condom use tokeep the overall infective population under the control. This will help in reducing theAIDS population as well. Also by simulation it is shown that by controlling the rate<strong>of</strong> vertical transmission, the spread <strong>of</strong> the disease can be reduced significantlyconsequently the equilibrium values <strong>of</strong> infective, <strong>treatment</strong> and AIDS population canbe maintained at desired levels. It is also found that the increase in the number <strong>of</strong>
75sexual partners further reduces the total population by way <strong>of</strong> spreading the disease.Thus, in order to reduce the spread <strong>of</strong> the disease, the number <strong>of</strong> sexual partners aswell as unsafe sexual interaction <strong>with</strong> an infective is to be restricted. The effect <strong>of</strong> anincrease in disease-induced death rate is, however, to decrease the AIDS patientspopulation. From the analysis, it may also be speculated that if the HIV infection issuppressed at an early stage by effectively treating the infectives, the progression tothe AIDS can be slowed down and the life span <strong>of</strong> HIV infectives can be prolonged.5.3 Future WorkHIV/AIDS at present has no cure and no vaccine as yet. As the number <strong>of</strong> reportedcases <strong>of</strong> AIDS continues to swell, the magnitude and severity <strong>of</strong> the problembecomes increasingly evident and the need to develop effective strategies to preventand control HIV infection is becoming even more urgent. In this study it is pointedout here that not all infected individuals take part in spreading the disease, as in thecase <strong>of</strong> infected children, but they will all develop their own AIDS.From the base <strong>of</strong> this study, it is proposed that future work should consider that allinfected individuals to take part in spreading the disease, as in the case <strong>of</strong> infectedchildren and develop to AIDS.Also the model can be modified to include a delay to make the infected childrenbecome adult to further spread the infection either vertically or horizontally.
76REFFERENCESAgarwala, B.D (2002), “On two ODE models for HIV/AIDS development inCanada and a logistic SEIR model”, Far East J, Appl. Math. 6 (1) (2002)25–70..Anderson, R.M., Medly G.F., May R.M., Johnson, A.M (1998), “A preliminarystudy <strong>of</strong> the transmission <strong>dynamics</strong> <strong>of</strong> the human immunodeficiencyvirus (HIV), the causative agent <strong>of</strong> AIDS”, IMA J. Math. Appl. Med. Biol.3 (1986) 229–263.Anderson, R.M (1998),“The role <strong>of</strong> <strong>mathematical</strong> models in the study <strong>of</strong> HIVtransmission and the epidemiology <strong>of</strong> AIDS”, J. AIDS 1 (1988) 241–256.Anndelman, R (2001), Mother to child HIV transmission in Africa. Policy Fact.AVERT (2010), HIV <strong>treatment</strong>. http://www.avert.org/<strong>treatment</strong>.htm.Retrieved on 24 th December 2010.Busenberg and Cooke K.L (1995),“Vertically transmitted diseases modelsand<strong>dynamics</strong>”. Biomathematics, vol. 23 springer-Verlag.Castillo-Chavez, C. and Song, B (2004),Dynamical models <strong>of</strong> Tuberculosis andtheir application. Math. Biosci. Eng. 1, 361404.Coovadia, H (2004), “Antiretroviral agents—how best to protect infants fromHIV and save their mothers from AIDS”, N. Engl. J. Med. 351 (3): 289–292.
77Cochrane Systematic Review on interventions for prevention <strong>of</strong> late postnatalmother-to-child transmission <strong>of</strong> HIVhttp://www.cochrane.org/reviews/en/ab006734.html. Retrieved on 4 thJanuary 2011Csete. Joanne. Pearshouse. Richard. Symington. Alison.,(2009), Vertical HIVtransmission should be excluded from criminal prosecution. ReproductiveHealth Matters.Department <strong>of</strong> Health and Human Services (2005), A Pocket Guide to AdultHIV/AIDSTreatment.(http://www.hab.hrsa.gov/tools/<strong>hiv</strong>pocketguide05/PktGARTtables.htm).Retrieved on 15 th October 2010.Fred, B (1994), Models for Diseases <strong>with</strong> Vertical Transmission and NonlinearPopulation Dynamics.Johnson, L (2004),An Introduction to the mathematics <strong>of</strong> HIV/AIDS <strong>modelling</strong>,Center for Actuarial Research.May, R.M., Anderson, R.M (1998),Transmission dynamic <strong>of</strong> humanimmunodeficiency virus (HIV). Phil. Trans. Roy. Soc.321, 565-607.Mbabaz, D (2008), Population Dynamic Type Models in HIV Infection. AfricanInstitute for Mathematical Science.Morgan D., Mahe C., Mayanja B., Okongo J.M., Lubega R., Whitworth J.A., (2002),“HIV-1 infection in rural Africa: is there a difference in median time to
78AIDS and survival compared <strong>with</strong> that in industrialized countries?”,AIDS 16 (4): 597–632.NACP (2009),”HIV/AIDS/STI Surveillance Report”, Ministry <strong>of</strong> Health and SocialWelfare. Report Number 21Naresh R., Tripathi A., Omar S.,(2006),“Modelling the spread <strong>of</strong> AIDS epidemic<strong>with</strong> vertical transmission”. Applied Mathematics and Computation 178:262-272.Newell M, L (1998), “Mechanism and timing <strong>of</strong> mother to child transmission <strong>of</strong>HIV-1”. AIDS 12: 832-837.Palella F. J., Delaney K. M., Moorman A. C., Loveless M. O., Fuhrer J., Satten G.A., Aschman D. J. and Holmberg S. D. (1998), “Declining morbidity andmortality among patients <strong>with</strong> advanced human immunodeficiency virusinfection”, N. Engl. J. Med. 338 (13): 853–860.Royce R.A., Sena A., Cates W., Cohen M.S., (1997), “Sexual transmission <strong>of</strong> HIV”,New Eng J Med 336 (15): 1072-1078.Schneider MF, Gange SJ, Williams CM, Anastos K, Greenblatt RM, Kingsley L,Detels R, Munoz A (2005), “Patterns <strong>of</strong> the hazard <strong>of</strong> death after AIDSthrough the evolution <strong>of</strong> antiretroviral therapy”, AIDS 19 (17): 2009–18.Simwa R., Pokhariyal G.P., (2003).A dynamical model for stage-specific HIVincidences <strong>with</strong> application to sub-Saharan Africa. Department <strong>of</strong>Mathematics, University <strong>of</strong> Nairobi.
79WHO and AIDS (2009) Toward Universal Access Scaling up priority HIV/AIDSinterventions in the health sectorhttp://www.who.who.int/entity/<strong>hiv</strong>/mediacentre/who .Retrieved on 28 thNovember2010.UNAIDS/WHO (2005), Question and Answers III – Selected issues; Preventionand Care, http://www.un<strong>aids</strong>.org/. Retrieved on 10 th October, 2010.(http://data.un<strong>aids</strong>.org/pub/GlobalReport/2008). Retrieved on 4 th December, 2010.