About Brain Injury: A Guide to Brain Anatomy
About Brain Injury: A Guide to Brain Anatomy
About Brain Injury: A Guide to Brain Anatomy

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
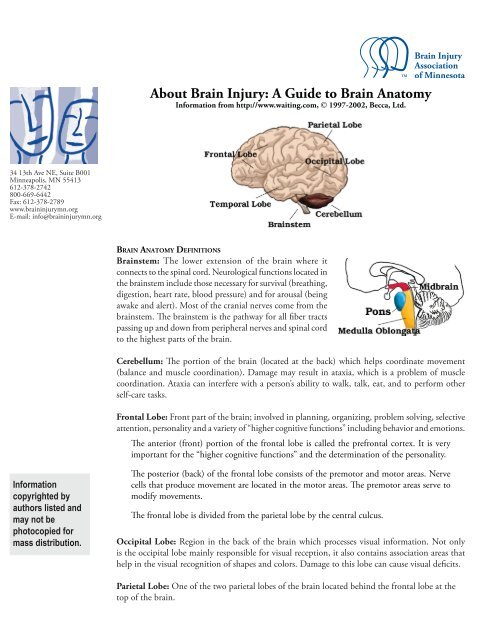
<strong>About</strong> <strong>Brain</strong> <strong>Injury</strong>: A <strong>Guide</strong> <strong>to</strong> <strong>Brain</strong> Ana<strong>to</strong>myInformation from http://www.waiting.com, © 1997-2002, Becca, Ltd.34 13th Ave NE, Suite B001Minneapolis, MN 55413612-378-2742800-669-6442Fax: 612-378-2789www.braininjurymn.orgE-mail: info@braininjurymn.org<strong>Brain</strong> Ana<strong>to</strong>my Definitions<strong>Brain</strong>stem: The lower extension of the brain where itconnects <strong>to</strong> the spinal cord. Neurological functions located inthe brainstem include those necessary for survival (breathing,digestion, heart rate, blood pressure) and for arousal (beingawake and alert). Most of the cranial nerves come from thebrainstem. The brainstem is the pathway for all fiber tractspassing up and down from peripheral nerves and spinal cord<strong>to</strong> the highest parts of the brain.Cerebellum: The portion of the brain (located at the back) which helps coordinate movement(balance and muscle coordination). Damage may result in ataxia, which is a problem of musclecoordination. Ataxia can interfere with a person’s ability <strong>to</strong> walk, talk, eat, and <strong>to</strong> perform otherself-care tasks.Frontal Lobe: Front part of the brain; involved in planning, organizing, problem solving, selectiveattention, personality and a variety of “higher cognitive functions” including behavior and emotions.The anterior (front) portion of the frontal lobe is called the prefrontal cortex. It is veryimportant for the “higher cognitive functions” and the determination of the personality.Informationcopyrighted byauthors listed andmay not bepho<strong>to</strong>copied formass distribution.The posterior (back) of the frontal lobe consists of the premo<strong>to</strong>r and mo<strong>to</strong>r areas. Nervecells that produce movement are located in the mo<strong>to</strong>r areas. The premo<strong>to</strong>r areas serve <strong>to</strong>modify movements.The frontal lobe is divided from the parietal lobe by the central culcus.Occipital Lobe: Region in the back of the brain which processes visual information. Not onlyis the occipital lobe mainly responsible for visual reception, it also contains association areas thathelp in the visual recognition of shapes and colors. Damage <strong>to</strong> this lobe can cause visual deficits.Parietal Lobe: One of the two parietal lobes of the brain located behind the frontal lobe at the<strong>to</strong>p of the brain.
Parietal Lobe, Right - Damage <strong>to</strong> this area can cause visuo-spatial deficits (e.g., the patientmay have difficulty finding their way around new, or even familiar, places).Parietal Lobe, Left - Damage <strong>to</strong> this area may disrupt a person’s ability <strong>to</strong> understand spokenand/or written language.34 13th Ave NE, Suite B001Minneapolis, MN 55413612-378-2742800-669-6442Fax: 612-378-2789www.braininjurymn.orgE-mail: info@braininjurymn.orgThe parietal lobes contain the primary sensory cortex which controls sensation (<strong>to</strong>uch,pressure). Behind the primary sensory cortex is a large association area that controls finesensation (judgment of texture, weight, size, and shape).Temporal Lobe: There are two temporal lobes, one on each side of the brain located at about the levelof the ears. These lobes allow a person <strong>to</strong> tell one smell from another and one sound from another.They also help in sorting new information and are believed <strong>to</strong> be responsible for short-term memory.Right Lobe - Mainly involved in visual memory (i.e., memory for pictures and faces).Left Lobe - Mainly involved in verbal memory (i.e., memory for words and names).<strong>About</strong> <strong>Brain</strong> <strong>Injury</strong>:The Areas of the <strong>Brain</strong>, Their Function, & Associated Signs & Symp<strong>to</strong>msInformationcopyrighted byauthors listed andmay not bepho<strong>to</strong>copied formass distribution.<strong>Brain</strong> StructureCerebral CortexLeft HemisphereFunctionThe outermost layer of the cerebralhemisphere which is composed of graymatter. Cortices are asymmetrical.Both hemispheres are able <strong>to</strong> analyzesensory data, perform memoryfunctions, learn new information,form thoughts and make decisions.Sequential Analysis: systematic,logical interpretation of information.Interpretation and production ofsymbolic information: language,mathematics, abstraction and reasoning.Memory s<strong>to</strong>red in a language format.Associated Signs andSymp<strong>to</strong>ms
34 13th Ave NE, Suite B001Minneapolis, MN 55413612-378-2742800-669-6442Fax: 612-378-2789www.braininjurymn.orgE-mail: info@braininjurymn.orgH o l i s t i c F u n c t i o n i n g :processing multi-sensory inputsimultaneously <strong>to</strong> provide“holistic” picture of one’senvironment. Visual spatial skills.Holistic functions such as dancingand gymnastics are coordinatedby the right hemisphere. Memoryis s<strong>to</strong>red in audi<strong>to</strong>ry, visual andspatial modalities.Corpus CallosumConnects right and left hemisphere<strong>to</strong> allow for communicationbetween the hemispheres. Formsroof of the lateral and thirdventricles.Damage <strong>to</strong> the CorpusCallosum may result in “Split<strong>Brain</strong>” syndrome.Frontal LobeCognition and memory. Prefrontalarea: The ability <strong>to</strong> concentrateand attend, elaboration ofthought. The “Gatekeeper”;( j u d g m e n t , i n h i b i t i o n ) .Personality and emotionaltraits.Movement:Mo<strong>to</strong>r Cortex(Brodman’s): voluntary mo<strong>to</strong>ractivity.Premo<strong>to</strong>r Cortex: s<strong>to</strong>rageof mo<strong>to</strong>r patterns and voluntaryactivities. Language: mo<strong>to</strong>rspeech.• Impairment of recentmemory, inattentiveness,inability <strong>to</strong> concentrate,behavior disorders, difficultyin learning new information.L a c k o f i n h i b i t i o n(inappropriate social and/orsexual behavior). Emotionallability. “Flat” affect.• Contralateral plegia, paresis.• Expressive/mo<strong>to</strong>r aphasia.Informationcopyrighted byauthors listed andmay not bepho<strong>to</strong>copied formass distribution.Parietal LobeProcessing of sensory input,sensory discrimination.Body orientation.Primary/ secondary somaticarea.• Inability <strong>to</strong> discriminatebetween sensory stimuli.• Inability <strong>to</strong> locate andrecognize parts of the body(Neglect).• Severe <strong>Injury</strong>: Inability <strong>to</strong>recognize self.• D i s o r i e n t a t i o n o fenvironment space.• Inability <strong>to</strong> write.
Occipital LobePrimary visual reception area.Primary visual association area:Allows for visual interpretation.• Primary Visual Cortex: loss ofvision opposite field.• Visual Association Cortex:loss of ability <strong>to</strong> recognizeobject seen in opposite field ofvision, “flash of light”, “stars”.34 13th Ave NE, Suite B001Minneapolis, MN 55413612-378-2742800-669-6442Fax: 612-378-2789www.braininjurymn.orgE-mail: info@braininjurymn.orgTemporal LobeAudi<strong>to</strong>ry receptive area andassociation areas.Expressed behavior.• Hearing deficits.• Agitation, irritability, childishbehavior.• Receptive/ sensory aphasia.Language: Receptive speech.Memory: Information retrieval.Limbic SystemOlfac<strong>to</strong>ry pathways:Amygdala and their differentpathways.• Loss of sense of smell.• Agitation, loss of controlof emotion. Loss of recentmemory.Hippocampi and their differentpathways.Limbic lobes: Sex, rage, fear, andemotions. Integration of recentmemory, biological rhythms.Hypothalamus.Basal GangliaSubcortical gray matter nuclei.Processing link between thalamusand mo<strong>to</strong>r cortex. Initiation anddirection of voluntary movement.Balance (inhibi<strong>to</strong>ry), Posturalreflexes.• Movement disorders:chorea, tremors at rest andwith initiation of movement,abnormal increase in muscle<strong>to</strong>ne, difficulty initiatingmovement.Informationcopyrighted byauthors listed andmay not bepho<strong>to</strong>copied formass distribution.ThalamusPart of extrapyramidal system:regulation of au<strong>to</strong>matic movement.Processing center of the cerebralcortex. Coordinates and regulates allfunctional activity of the cortex viathe integration of the afferent input<strong>to</strong> the cortex (except olfaction).Contributes <strong>to</strong> affectual expression.• Parkinson’s.• A l t e r e d l e v e l o fconsciousness.• Loss of perception.• Thalamic syndrome -spontaneous pain oppositeside of body.
34 13th Ave NE, Suite B001Minneapolis, MN 55413612-378-2742800-669-6442Fax: 612-378-2789www.braininjurymn.orgE-mail: info@braininjurymn.orgHypothalamusIntegration center of Au<strong>to</strong>nomicNervous System (ANS): Regulationof body temperature and endocrinefunction.A n t e r i o r H y p o t h a l a m u s :parasympathetic activity (maintenancefunction).Posterior Hypothalamus: sympatheticactivity (“Fight” or “Flight”, stressresponse.• Hormonal imbalances.• Malignant hypothermia.Inability <strong>to</strong> controltemperature.• Diabetes Insipidus (DI).Inappropriate ADH• (SIADH). Diencephalicdysfunction: “neurogenics<strong>to</strong>rms”.Behavioral patterns: Physical expressionof behavior.Appestat: Feeding center.Pleasure center.Internal Capsule Mo<strong>to</strong>r tracts. Contralateral plegia (Paralysisof the opposite side of thebody).Reticular ActivatingSystem (RAS)Responsible for arousal fromsleep, wakefulness, attention.Altered level ofconsciousness.CerebellumCoordination and control ofvoluntary movement.• Tremors.• Nystagmus (Involuntarymovement of the eye).• Ataxia, lack of coordination.Informationcopyrighted byauthors listed andmay not bepho<strong>to</strong>copied formass distribution.<strong>Brain</strong> Stem:Ne r ve p a t h w a y o f c e rebralhemispheres.Audi<strong>to</strong>ry and Visual reflex centers.Cranial Nerves:• CN III - Oculomo<strong>to</strong>r (Related <strong>to</strong>eye movement), [mo<strong>to</strong>r].• CN IV - Trochlear (Superior obliquemuscle of the eye which rotates theeye down and out), [mo<strong>to</strong>r].• Weber’s: CN III palsy andp<strong>to</strong>sis (drooping) ipsalateral(same side of body).• Pupils: Size: Midposition <strong>to</strong>dilated. Reactivity: Sluggish <strong>to</strong>fixed.• LOC (Loss of consciousness):Varies • Movement: Abnormalextensor ( muscle that extendsa part).• Respira<strong>to</strong>ry: Hyperventilating.• CN (Cranial Nerve) Deficits:CN III, CN IV.
34 13th Ave NE, Suite B001Minneapolis, MN 55413612-378-2742800-669-6442Fax: 612-378-2789www.braininjurymn.orgE-mail: info@braininjurymn.orgPonsRespira<strong>to</strong>ry Center.Cranial Nerves:• CN V - Trigeminal (Skinof face, <strong>to</strong>ngue, teeth;muscle of mastication),[mo<strong>to</strong>r and sensory].• CN VI - Abducens (Lateralrectus muscle of eye whichrotates eye outward),[mo<strong>to</strong>r].• CN VII - Facial (Muscles ofexpression), [mo<strong>to</strong>r andsensory].• CN VIII - Acoustic (Internala u d i t o r y p a s s a g e ) ,[sensory].• Pupils: Size: Pinpoint• LOC:Semi-coma“Akinetic Mute”“Locked In” Syndrome.• Movement:Abnormal extensor.Withdrawal.• Respira<strong>to</strong>ry:Ap n e u s t i c ( Ab n o r m a lrespiration marked bysustained inhalation).• Hyperventilation.• CN Deficits: CN VI, CNVII.Informationcopyrighted byauthors listed andmay not bepho<strong>to</strong>copied formass distribution.Medulla OblongataCrossing of mo<strong>to</strong>r tracts.Cardiac Center.Respira<strong>to</strong>ry Center.Vasomo<strong>to</strong>r (nerves havingmuscular control of the bloodvessel walls) Center Centers forcough, gag, swallow, and vomit.Cranial Nerves:• CN IX - Glossopharyneal( Mu s c l e s a n d m u c o u smembranes of pharynx, theconstricted openings from themouth and the oral pharynxand the posterior third of<strong>to</strong>ngue.), [mixed].• CN X - Vagus (Pharynx,larynx, heart, lungs, s<strong>to</strong>mach),[mixed].• CN XI – Accessory (Rotationof the head and shoulder),[mo<strong>to</strong>r].• Movement: Ipsilateral(same side) plegia (paralysis).• Pupils:Size: DilatedReactivity: Fixed.•LOC: Coma<strong>to</strong>se.• Respira<strong>to</strong>ry:Abnormal breathingpatterns.Ataxic.Clustered.Hiccups.• CN Palsies (Inability <strong>to</strong>control movement):• Absent Cough.• Gag.• CN XII – Hypoglossal(Intrinsic muscles of the<strong>to</strong>ngue), [mo<strong>to</strong>r].
<strong>About</strong> <strong>Brain</strong> <strong>Injury</strong>: Intracraniel PressureDoes the brain always swell? How do you know if the brain is swelling? Doesn’t the CT scanshow swelling? Is it possible that the person’s brain did not swell because of the use of the drugmani<strong>to</strong>l (pro<strong>to</strong>col treatment in all ICU’s)? Is the chemical released if there is no swelling? If aperson didn’t need a shunt, can we assume there was no swelling?34 13th Ave NE, Suite B001Minneapolis, MN 55413612-378-2742800-669-6442Fax: 612-378-2789www.braininjurymn.orgE-mail: info@braininjurymn.orgPretty much all tissues in the body swell when traumatized. They also require more oxygen <strong>to</strong>heal. The brain is unique in that it rests inside a bone case, so when it swells, it experiencesmore trauma.The more damage the brain receives, the more it swells. This is caused by leakage from bloodvessels. When the brain swells, because it is housed inside the skull, it has no room <strong>to</strong> expand.This leads <strong>to</strong> a rise in pressure within the brain. This rise in pressure rapidly equals the arterialpressure thereby affecting the blood flow <strong>to</strong> the brain. This diffuse pressure which decreasesblood flow affects the ability of the cells within the brain <strong>to</strong> metabolize properly; the cells areunable <strong>to</strong> eliminate <strong>to</strong>xins which then accumulate.This phenomenon leads <strong>to</strong> a spiral effect which is what kills brain injured people who don’tget prompt attention. One of the big breakthroughs that lead <strong>to</strong> the survival rate we have nowfor brain injury <strong>to</strong>day was learning <strong>to</strong> break this cycle. We are still very much in the stage oflearning <strong>to</strong> break this cycle. The most significant fac<strong>to</strong>r has been the use of moni<strong>to</strong>ringdevices <strong>to</strong> inform treatments <strong>to</strong> prevent further damage.The brain requires both oxygen and glucose. In response <strong>to</strong> the trauma, changes occurin the brain which require moni<strong>to</strong>ring <strong>to</strong> prevent further damage. The brain’s sizefrequently increases after a severe head injury. This is called brain swelling and occurswhen there is an increase in the amount of blood <strong>to</strong> the brain.Informationcopyrighted byauthors listed andmay not bepho<strong>to</strong>copied formass distribution.Water may collect in the brain which is called <strong>Brain</strong> Edema. Both <strong>Brain</strong> swelling and <strong>Brain</strong>Edema result in excessive pressure in the brain called Intracranial Pressure (ICP). Aroundthe-clockmoni<strong>to</strong>ring during this time is essential in order that ICP can be immediatelytreated. Treatment of brain swelling can be difficult. Very strong medications are administered.Medications which help <strong>to</strong> draw fluid back out of the brain and in<strong>to</strong> blood vessels may beuseful. Some medications help by decreasing the metabolic requirements of the brain. Othermedications increase blood flow in<strong>to</strong> the brain which can help diminish the spiral effect causedby brain swelling.In some cases, removal of small amounts of fluids or from the brain or surgery may be beneficial.And in some cases, removal of damaged tissue may prevent further damage.