Waiting to work - Minnesota Brain Injury Alliance
Waiting to work - Minnesota Brain Injury Alliance
Waiting to work - Minnesota Brain Injury Alliance

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
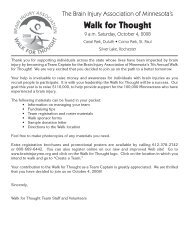
A state affliate of the <strong>Brain</strong> <strong>Injury</strong> Association of AmericaHEADLINESWINTER 2004/05IN THIS ISSUE:Check out the NewsBriefs sectioninside on page 4The Associationadds case management<strong>to</strong> its servicesin side on page 5Learn about medicationsused in the treatment ofbrain injuryinside on page 6Creative article onaphasia and poetryinside on page 12New blood test for TBIdiagnosis!inside on page 13Estate Planninginside on page 16UPCOMING EVENTS:<strong>Brain</strong> <strong>Injury</strong> BasicsFebruary 15Walk for Thought draws a thousand participantsStaff ReportMINNEAPOLIS - The 2004Walk for Thought was the largestfundraising event ever in the20 years of the <strong>Brain</strong> <strong>Injury</strong>Association of <strong>Minnesota</strong>’shis<strong>to</strong>ry. The walks in the TwinCities and Blackduck drewnearly 1,000 people for a day ofcelebration, commemoration, andcommunity involvement.Nearly 1,000 people <strong>to</strong>oktheir time, energy, and resources<strong>to</strong> promote the Association andthe important issue of braininjury. In the course of this event,1,000 people knocked on theirneighbors’ doors, made telephonecalls, sent emails and letters,and <strong>to</strong>ld their personal s<strong>to</strong>riesabout brain injury <strong>to</strong> countless<strong>Minnesota</strong>ns. As with other <strong>Brain</strong><strong>Injury</strong> Association of <strong>Minnesota</strong>activities, this was a tremendousgrassroots effort of which we canall be very proud. <strong>Brain</strong> injury isconsidered the “silent epidemic”due <strong>to</strong> the low public awarenesson this issue, but because of thepho<strong>to</strong> by Sharon RolencIn 2003, the Dragonfly Clan pledged <strong>to</strong> be this year’s <strong>to</strong>p fundraisers. Keepingtheir promise, they raised over $5,100 for the 2004 Walk for Thought. Picturedfrom left <strong>to</strong> right: Jim and Sue Winkel, Team Captain Tracy Winkel-Johnson, andChad Johnson.efforts of a growing number ofindividuals, we are making adifference.This year, over 50 teamcaptains, 23 corporate sponsors,and 14 volunteers went over andabove the call of duty. This levelof support is impressive andexciting as it demonstrates theWALK FOR THOUGHTon page 10<strong>Waiting</strong> <strong>to</strong> <strong>work</strong>Vocational Rehabilitation waiting list felt statewideNew in 2005:<strong>Brain</strong> <strong>Injury</strong> Basics 2March 15Save the Date:3rd Annual Xtreme SafetyFest at the Mall of AmericaApril 23The 20th AnnualStatewide Conferenceon <strong>Brain</strong> <strong>Injury</strong>May 20 & 21Check page 2 for moredetails on these events<strong>Brain</strong> <strong>Injury</strong>Association of<strong>Minnesota</strong> helpline:1-800-669-6442www.braininjurymn.orgBy Sharon RolencAfter six years of a rigorouscollege course load, MatthewBalken was well on his way <strong>to</strong>establishing his career as a physicsand science teacher. On April24, 2004, the Erhard, <strong>Minnesota</strong>resident fell from a roof, landingon the back of his head. Balkenfell so hard that he flipped overand hit the front, causing injury <strong>to</strong>multiple parts of his brain.“I was in intensive care for11 days, unconscious for 10 days,on life support for four days, inacute care for a month and then arehabilitation hospital for anothermonth,” he said.Balken sustained a brain injurythat effected hearing in his leftear, nerve damage, coordinationand balance, short term memory,problem solving, multitasking andother executive functioning skills.“Those are the skills I reallyrely on as a teacher,” he said.The neuropsychologicaltests that he <strong>to</strong>ok put him in theaverage range for math. “That’snowhere near what I used <strong>to</strong> be.The problem with those tests isthat they are designed for a broadrange of people and the averagescores are based on that broadrange,” said Balken.Concerned that he may notbe able <strong>to</strong> teach at the samelevel as before, Balken turned <strong>to</strong>Vocational Rehabilitation (VR)<strong>to</strong> help him figure out his careeroptions. VR is a governmentprogram designed for personswith disabilities who need support34 13th Ave NE, Suite B001Minneapolis, MN 55413Time Dated MaterialAddress Service Requestedservices <strong>to</strong> prepare for <strong>work</strong>, or <strong>to</strong>find or keep a job. Services canrange from minimal job coaching<strong>to</strong> proving a four year degree.“One of the beauties of theVR program is that our servicesare tailored <strong>to</strong> the specific needsof the individual. The plans reallyrun the gamut. There are someWAITINGon page 8Non-profit OrganizationU.S. PostagePAIDMinneapolis, MNPermit #163
HEADLINES WINTER 2004/05CALENDAR of EVENTSFebruary 15: <strong>Brain</strong> <strong>Injury</strong> Basics1Confusion. Frustration. Sorrow.Anger. Fear. Isolation. Theseare some emotions a person withbrain injury may feel after injury.Families, friends & loved onesmay feel this way, <strong>to</strong>o.Learn about the impact ofbrain injuries caused by concussion,traumas such as crashes orfalls, stroke, aneurysm & coma.Learn about what brain injuryis; the common side effects ofbrain injury; compensation techniques;and tips about how <strong>to</strong> relate<strong>to</strong> people who have sustainedbrain injury.These classes are offered fourtimes a year. Class begins at 6:00p.m. and runs until 8:30 p.m.Remaining dates for 2005 are May17, August 16 and November 15.To register, call 612-378-2742 or1-800-669-6442 in greater <strong>Minnesota</strong>.May 20 & 21: 20th Annual StatewideConference on <strong>Brain</strong> injurySave the date! The 20th AnnualConference on <strong>Brain</strong> <strong>Injury</strong>will be held at the St. Cloud CivicCenter in St. Cloud, Minn. Turn <strong>to</strong>page 7 for complete details!March 15: <strong>Brain</strong> <strong>Injury</strong> Basics 2This new class at the Associationaddresses the life change tha<strong>to</strong>ccurs with brain injury: majorstages of adjustment, emotionalaspects of the change and adjustmentdifficulties.These classes are offered fourtimes a year. Class begins at 6:00p.m. and runs until 8:30 p.m.Remaining dates for 2005 are June21, September 20 and December20.Support GroupsApril 23: 3rd Annual Xtreme SafetyFest at the Mall of AmericaSave the date! The 3rd AnnualXtreme Safety Fest is an excitingfamily activity with live BMX &Skateboard demonstrations, safetyinformation and free helmets.Send the message <strong>to</strong> your childrenthat they can play it safe whileplaying hard! The event takesplace from 1:00 - 4:30 pm.New this year - the Associationwill be taking its safety and injuryprevention program on the road.You organization has the opportunity<strong>to</strong> have the Association bringfree helmets and safety information<strong>to</strong> your community event.Watch the Association website forRFP information.<strong>Brain</strong> injury support groups can help you find others with similarexperiences, useful information about brain injury and solutions <strong>to</strong>problems. The following results are just some of the key benefits ofsupport groups:• Emotional healing comes when people interact with otherpeople.• Sharing of similar experiences helps members feel lessalone and more ready <strong>to</strong> deal with day <strong>to</strong> day issues.• Education results from the exposure <strong>to</strong> information andpersonal experiences in a group.• Socialization occurs when connections with people aremade and confidence in social skills develops when appropriateinteraction occurs in support groups.• Safety, in the environment of a confidential, supportive,non-judgmental group, allows for honest disclosure and sharing ofcommon difficulties.• Self-expression, as emotions are experienced and released,creates a greater understanding of oneself.• A sense of growth occurs as long-term members see newparticipants and reminisce about where they began and how farthey have come in their personal journey.The <strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong> makes referrals <strong>to</strong>support groups throughout the state, including for persons with braininjury, their families and friends and for young persons.These groups are au<strong>to</strong>nomous, self-determined peer groups andare independent of the Association.For meeting times, location, and a contact person for a specificsupport group, or for information about how <strong>to</strong> start your own group,call the <strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong> at 612-378-2742 or1-800.669.6442.Letter <strong>to</strong> the Edi<strong>to</strong>rDear TBI Advocate,34 13th Ave NE, Suite B001Minneapolis, MN 55413612.378.2742 or 800.669.6442fax: 612.378.2789www.braininjurymn.orgEmail: info@braininjurymn.orgMissionThe mission of the <strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong> is <strong>to</strong> create a betterfuture through brain injury prevention, research, education and advocacy.Board of Direc<strong>to</strong>rsNancy Carlson, ChairOt<strong>to</strong> Bang Richard Bloom Ken Brit<strong>to</strong>nBarb Ful<strong>to</strong>n Tom Gode Robin LandyGwyn Leder Sue Lepore Craig MartinsonSue Meserow Sarah Moeller Russ PhilstromDave Scott Kate Shannon Elizabeth Skinner SandraSmith Mike Strand Terri TraudtPat WinickAssociation StaffMichelle Brandes, Case ManagerBrad Donaldson, Direc<strong>to</strong>r of OperationsKimberly Ferencik, Volunteer Coordina<strong>to</strong>rTom Gode, Executive Direc<strong>to</strong>rMark Hahn, Administrative AssistantWillis Johnson, Data Entry SpecialistEllen Kuschke, Communications InternKaty O’Brien, Resource Facilita<strong>to</strong>r Team LeaderIvy Peterson, Resource Facilita<strong>to</strong>rShannon Robins, Public Policy Direc<strong>to</strong>rSharon Rolenc, Public Awareness Direc<strong>to</strong>rChristina Saby, Resource Facilita<strong>to</strong>rArdis Sandstrom, Associate Direc<strong>to</strong>rOttar Schmitz, Development Coordina<strong>to</strong>rAnne Schuller, Education Coorina<strong>to</strong>rpage 2The results are in and they are good! Overall, the TBI Actreceived a modest increase in funding. All TBI Act programswere level-funded (received the same amount of money as fiscalyear 2004) with an increase of $515,000 for TBI programs in theCenters for Disease Control and Prevention (CDC).Our letter asked Congress <strong>to</strong> pass the House recommended $1million increase for CDC TBI programs. They compromisedand approved $515,000. That is doing well in the current budgetenvironment!We have no doubt that the thousands of emails and letters thatflooded Capi<strong>to</strong>l Hill in the past month had an impact!With the budget for fiscal year 2005 set, we now shift our sights<strong>to</strong> the Reauthorization of the TBI Act itself in 2005.We will need your continued support <strong>to</strong> make sure this importantlaw does not disappear! Stay tuned and congratulations on a jobwell done.Geoffrey M. LauerNational Direc<strong>to</strong>r of Affiliate Relations<strong>Brain</strong> <strong>Injury</strong> Association of AmericaEdi<strong>to</strong>rial PolicyHeadlines is published quarterly by the <strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong>.The Edi<strong>to</strong>r reserves the right <strong>to</strong> edit submitted materials for style and space.The Association does not endorse, support, or recommend any specific method,facility, treatment, program, or support group for persons with brain injury andtheir families. Please call for advertising rates.Letters <strong>to</strong> the Edi<strong>to</strong>r PolicyLetters <strong>to</strong> the Edi<strong>to</strong>r should be limited <strong>to</strong> 300 words. Letters may be editedfor spelling, grammar and length. In order for letters <strong>to</strong> be considered, pleaseinclude your name, address and the daytime phone number of the author. TheAssociation reserves the right <strong>to</strong> refuse letters for publication., and submissionof material does not guarantee publication. Opinions expressed in Letters <strong>to</strong> theEdi<strong>to</strong>r are solely those of the author and do not represent the opinions or positionsof the Association.
HEADLINES WINTER 2004/05page 4NEWS BRIEFSResourceFacilitationMore and more hospitalsthroughout the state arediscovering that the ResourceFacilitation Program is a useful<strong>to</strong>ol for their discharge staff. Byproviding this free resource <strong>to</strong>your patients, it can help: Save time and providesupport <strong>to</strong> your discharge planners,nurses, social <strong>work</strong>ers and othersinvolved with the dischargeprocess. Provide quality cus<strong>to</strong>merservice <strong>to</strong> your patients and serveas a positive indica<strong>to</strong>r of patientexperience. Support your patients afterthey leave the hospital <strong>to</strong> copewith the issues of living with abrain injury.The Resource FacilitationProgram is a free follow-upservice through the <strong>Brain</strong> <strong>Injury</strong>Association of <strong>Minnesota</strong>. Itprovides support for <strong>Minnesota</strong>ns<strong>to</strong> cope with the issues of livingwith a traumatic brain injury andhelp them transition back <strong>to</strong> <strong>work</strong>,school and their communities.This service does not replaceany medical or rehabilitationfollow-up that may be needed.It is intended <strong>to</strong> support patientsand their families, as well ashelp ease the minds of healthcareprofessionals, knowing theirpatients are getting follow-upsupport on a regular basis. Theprogram is funded through acontract with the <strong>Minnesota</strong>Department of Health, making itpossible for every hospital in thestate <strong>to</strong> offer the program as a freeservice <strong>to</strong> their patients.For persons with braininjury, Resource Facilitationcan help: answer questions, problem-solve issues, identify resources withinyour community, and educate family members,employers, and educa<strong>to</strong>rsabout what it means <strong>to</strong> livewith a brain injury.For persons with brain injury,or family members who missedthis opportunity through theirhospitals, it is still possible <strong>to</strong> selfrefer<strong>to</strong> the Resource Facilitationprogram.For more information, contactthe Association at 612-378-2742or 1-800-669-6442.Courage CenterCloses DayProgramsOn November 12, CourageCenter closed their Adult Day andStructured Day programs. Thedecision <strong>to</strong> close the programsresulted from a number ofeconomic fac<strong>to</strong>rs including a softeconomy following 9/11. Theseincluded cuts in federal, state andlocal funding for social serviceorganizations such as Courage;lower levels of donations <strong>to</strong>support programs and services;and significant increases inmedical insurance and basicoperating costs.The Courage Center expresseda commitment <strong>to</strong> <strong>work</strong>ing withconsumers, their families, casemanagers or others <strong>to</strong> help throughthe transition. For more specificprogram or transition questionsor concerns contact one of thesepeople:Adult Day participants:Nancy Huizenga, Vocationaland Community-Based ServicesDirec<strong>to</strong>r, 763-520-0313Brigid Alseth, Adult Day ProgramDirec<strong>to</strong>r, 763-520-0420Structured Day participants:Karen Larson-Hahn, clinicaldirec<strong>to</strong>r, Mental Health & FamilySupport Services,763-520-0354Sharon Rendack, supervisor,Behavior Services, 763-520-0441For more information abou<strong>to</strong>ther resources for Adult Day andStructured Day programs in yourcommunity, contact a ResourceFacilita<strong>to</strong>r at the <strong>Brain</strong> <strong>Injury</strong>Association of <strong>Minnesota</strong> at 612-378-2742.Bethesda NowAdmitting TeensBethesda RehabilitationHospital will now accept patientsas young as sixteen, whichincludes the <strong>Brain</strong> <strong>Injury</strong> CareUnit on the St. Paul campus.Within <strong>Brain</strong> <strong>Injury</strong> Carethere are three inpatient programs:<strong>Brain</strong> <strong>Injury</strong> Rehabilitation,Neurobehavioral Crisis andAssessment and Neurobehavioral<strong>Brain</strong> <strong>Injury</strong>.What’s new at the Association and in the brain injury communityThe <strong>Brain</strong> <strong>Injury</strong>Rehabilitation is meant for patientswho need intense physical andcognitive rehabilitation, while theother two programs focus more onthe behavioral aspects of BI.Neurobehavioral Crisisand Assessment is a short-termprogram designed for people withsevere behavioral problems orconsumers with brain injuries whoneed an assessment. They offerboth assessment services and crisisstabilization plans. The intent ofthe Neurobehavioral <strong>Brain</strong> <strong>Injury</strong>program is <strong>to</strong> treat behavioralproblems on a long-term basis:people with good rehabilitationpotential but with behaviors thatinhibit the rehabilitation process.Dr. Robert Karol is both theProgram Direc<strong>to</strong>r of <strong>Brain</strong> <strong>Injury</strong>Services and the Direc<strong>to</strong>r ofNeuropsychology and Psychology.“A few months ago we startedtaking adolescents in<strong>to</strong> theprogram,” said Karol. “We haddecided there was enough of acommunity there that we should.”For more information, or <strong>to</strong>contact Bethesda’s <strong>Brain</strong> <strong>Injury</strong>Care Admissions office, call 651-232-2760 or 1-800-566-2720.Association Offers<strong>Brain</strong> <strong>Injury</strong> Basics,part 2New for 2005! Your commentson the BIB feedback forms havemade a difference! In response<strong>to</strong> the concerns and needs ofour consumers, the Associationhas added a Part 2 class <strong>to</strong> itscorners<strong>to</strong>ne <strong>Brain</strong> <strong>Injury</strong> Basics(BIB). This free intermediate<strong>work</strong>shop will address the lifechange of having a brain injury:major stages of adjustment,emotional aspects of the changeand adjustment difficulties.Adjustment <strong>to</strong> disability may bedescribed as a series of stages ormajor tasks, which may not alwaysbe neat and orderly. Individualsprogress through stages at differentrates, and adjustment is a life-longprocess. Emotional aspects ofdisability may be a major fac<strong>to</strong>rin outcomes. The schedule for2005 is as follows: Third Tuesdayof March, June, September andDecember, from 6:00 PM-8:30 PMAssociation OffersFamily RetreatThe <strong>Brain</strong> <strong>Injury</strong> Associationof <strong>Minnesota</strong> will offer a familyretreat at Camp Courage onMay 6 - 7, 2005. The campingexperience begins Friday eveningand concludes mid-afternoonon Saturday. Three meals areincluded in the retreat.Families needn’t worry about“roughing it” – the retreat doesn’trequire sleeping in tents. CampCourage has lovely cabins,situated in a rustic environment.If you have a school aged childwith a brain injury, this retreat isdesigned just for you. Families arewelcomeCamp Courage is a completelyaccessible facility. The retreatprovides a structured, enrichingpersonal and recreationalexperience. Watch Enews, theAssociation website and the nextedition of HEADLINES for moredetails. For more information,contact Anne Schuller, EducationCoordina<strong>to</strong>r at annes@braininjurymn.org, or by phone at612-378-2742; or Deb Williamson,State TBI Specialist via email atdcwilliamson@int287.k12.mn.usor by phone at 612-638-1532.Special thanks <strong>to</strong>MedtronicOn Oc<strong>to</strong>ber 29, 2004,Medtronic hosted a supportgroup leader training day. Theygenerously provided a room, breakfoods, and lunch for 28 current andfuture support group facilita<strong>to</strong>rs.The training was planned bythe <strong>Brain</strong> <strong>Injury</strong> Association, theEpilepsy Foundation, AmericanParkinson’s Disease, and the<strong>Minnesota</strong> Stroke Association.A special thanks <strong>to</strong> JerryHartlaub (retired Medtronicemployee and board member ofthe Epilepsy Foundation) andKathleen Lynch (Medtronicemployee) for their contributions.Jerry Hromatka led the groupthrough facilitation skills training,and Adine S<strong>to</strong>kes led a session on<strong>work</strong>ing with caregivers.Thanks again <strong>to</strong> Medtronic fortheir generosity and support.
WINTER 2004/05page 5HEADLINES<strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong> Adds Case Management <strong>to</strong> its ServicesBy Ellen KuschkeThis September, the <strong>Brain</strong><strong>Injury</strong> Association of <strong>Minnesota</strong>added Case Manager MichelleBrandes <strong>to</strong> its Minneapolisstaff. “Case management wasjust a natural next step for us,”said Associate Direc<strong>to</strong>r ArdisSandstrom. “The response fromthe resource facilitation programhas been very positive, so casemanagement is just taking it a stepfurther. We’re really looking at[providing] a full continuum ofservices; addressing the needs ofall people with brain injury.”A case manager’s mainfunction is <strong>to</strong> coordinate servicesand assist individuals <strong>to</strong> live atthe highest level of independencepossible as they adjust <strong>to</strong> theissues related <strong>to</strong> their traumaticbrain injury (TBI).Most TBI consumers andfamily members quickly learn theneed <strong>to</strong> explain traumatic braininjury <strong>to</strong> everyone, sometimeseven case managers. However,when consumers get referred <strong>to</strong>Michelle Brandes at the <strong>Brain</strong><strong>Injury</strong> Association, this isn’tnecessary. Brandes has <strong>work</strong>edwith people with TBI as a social<strong>work</strong>er with Courage Center.She has an established his<strong>to</strong>ryproviding case management forpersons with brain injury.“When the consumers arereferred <strong>to</strong> me, a lot of times it’sa big relief for them. The familymembers don’t have <strong>to</strong> explainanything,” said Brandes. “Theyfeel much better, <strong>work</strong>ing withthe <strong>Brain</strong> <strong>Injury</strong> Association andsomeone with experience [dealingwith TBI]. It really raises theconsumer’s comfort level, <strong>to</strong>o.”According <strong>to</strong> Brandes, one ofthe most vital (and lesser known)aspects of case management isre-socialization. After sustaininga brain injury, many consumersendure a long hospital stay,personality changes, memorylosses and mood disturbances.These demanding changes create adifferent lifestyle, often an isolatedone. The aftermath of a braininjury can cause a definite lack ofsocial involvement.There are many availableservices <strong>to</strong> address this problem:individual living skills classes,community day programs,support groups and sports andrecreation sessions. Services likethese help people with TBI <strong>to</strong>adjust <strong>to</strong> life with a disability andcreate a socially healthy lifestyle.Unfortunately, many people withTBI and their families are oftenunaware of these resources. A casemanager notifies consumers ofthe services available <strong>to</strong> them andcoordinates these services.Since case managerscoordinate care with thegovernment and the healthcareindustry, the job demands attention<strong>to</strong> detail and a lot of paper<strong>work</strong>.However, <strong>to</strong> Michelle Brandes, thefocus of the <strong>work</strong> remains clear:“Putting the person first. We makesure their safety and health needsare met within their community.”For more information aboutcase management, contactMichelle Brandes at 612-378-2742.pho<strong>to</strong> by Sharon RolencFormer board of direc<strong>to</strong>rs and staffers gather at the 20th Anniversary Party.From left <strong>to</strong> right: Baba Finch, Chris Duff, Fran Conklin and Vicky VogelsComprehensive<strong>Brain</strong> <strong>Injury</strong>Care andRehabilitation• Family Involvement• Prevention Services• Emergency Services• Inpatient Trauma ServicesCoordination• Acute Inpatient Stabilization• <strong>Brain</strong> <strong>Injury</strong> Rehabilitation• Knapp Rahabilitation Center• Mild <strong>to</strong> Moderate TBI Clinic• Pediatric and Adult• Community ReintegrationReferrals/Follow-up• Interdisciplinary Teams• Survivors Group• Statewide PhysiciansReferral Net<strong>work</strong>• Community Education(612) 873-3950 www.hcmc.org
HEADLINES WINTER 2004/05Medications Used in the Treatment of <strong>Brain</strong> <strong>Injury</strong>By Kenneth R. Brit<strong>to</strong>n, DO<strong>Brain</strong> injury, whether acquiredthrough trauma, vascular injury,lack of oxygen, or tumors, canhave a serious negative impac<strong>to</strong>n our ability <strong>to</strong> think, remember,move, care for our personal needsand <strong>work</strong>. Physicians who treatbrain injury often use medications<strong>to</strong> help promote brain recovery,treat symp<strong>to</strong>ms related <strong>to</strong> thebrain injury, or improve function.Depending on what problem thephysician is trying <strong>to</strong> address,they can prescribe a number ofdifferent types of medicationand also make a choice betweendifferent medications of the sameor similar type. It is common<strong>to</strong> use medications that <strong>work</strong> indifferent ways <strong>to</strong>gether at the sametime <strong>to</strong> improve the results and <strong>to</strong>minimize any side effects.This article will address thedifferent types of medications,how and why they are used, what<strong>to</strong> expect from them. Every braininjury is unique so the medicationplan must be individualized, butthere are some common guidingprinciples that can be followed.Essentially every medicationhas good points and bad points.The good points are called thetherapeutic effects or benefits. Thebad points are called side effects.Generally, medication is used forthe therapeutic effect, but once in awhile one will be used for the sideeffects. One example is Trazodone,a fairly weak antidepressant that isoften used <strong>to</strong> help with relaxationand sleep at night. Side effectscan develop right away or aftertime. With some side effects theyget better in a few days after thebody gets used <strong>to</strong> the medication.In other cases they stay the sameor get worse with time.Some medications can behelpful in the short term, butcause more problems in the longterm. An example is many ofthe calming medicines (Ativanand Haldol <strong>to</strong> name the mostcommon). They <strong>work</strong> very well <strong>to</strong>control agitation or aggression, butgenerally make people sleepy andmentally slow, which is a problemfor a survivor who is <strong>work</strong>ing hard<strong>to</strong> stay awake and stay focused.Every medication choice hasthe potential <strong>to</strong> be helpful andalso <strong>to</strong> be not helpful or at timesharmful. Physicians generally willnot know how a specific individualwill respond <strong>to</strong> a medicationuntil it is tried. For this reason,physicians tend <strong>to</strong> start at alower dose and slowly increaseit while moni<strong>to</strong>ring the survivorfor positive as well as negativeresponses. If this is done throughthe clinic it may mean that morefrequent visits are required untileveryone is satisfied that the rightmedication at the right dose isbeing prescribed. If there is ever aquestion or concern about possibleside effects from a medication theclinic or doc<strong>to</strong>r should be notifiedas soon as possible.For most persons with braininjury there is a period of up <strong>to</strong>two years after their injury wherethe brain is healing. This healingpage 6is most dramatic in the first fewmonths and generally slows downafter 3-6 months, but it can stillmean a significant change in thesurvivor’s ability and need formedication. As a result of thischanging condition, the medicationstrategy may also change as timeprogresses. Generally, this meansthat medications that were helpfulearlier in the recovery may be able<strong>to</strong> be reduced or eliminated as timeprogresses. However, at timesthe medication will be used on anongoing basis. Again, if in doubtthis should be discussed with thephysician.The table below lists some ofthe common medications used thatseem <strong>to</strong> be most helpful in braininjury treatment.This list does not include all ofthe medications that can be usedin the treatment of brain injuryrelated problems, but it does haveMEDICINEon page 16Medication TypeExamplesBenefitsAlerting Ritalin, Provigil, Stratera General alertness and focused attentionAntidepressantsEffexor, Celexa, Lexapro, Prozac,ZoloftIncreases sero<strong>to</strong>nin, and sometimesnorepinephrine levels in thebrain <strong>to</strong> let the brain <strong>work</strong> better.Increased responsiveness andfaster mental processing. Alsoprevents or treats depression related<strong>to</strong> the injury.Dopaminergic agents Bromocriptine, Amantadine Increases dopamine levels in thebrain. Improved alertness andprocessing. May also help withlanguage function.Atypical antipsychotics Seroquel, Zyprexa, Risperdol Calming effect and improves restlessnessand agitation generallywithout excessive sedation.Non-narcotic pain medication Tylenol, Ibuprofen, Celebrex Treat pain, especially if headache ortrauma. May be used on a scheduledbasis <strong>to</strong> control and prevent pain, oras needed.Narcotic pain medicationPercocet, Vicodan, Morphine,Tylenol #3Good for acute pain, especially iftrauma is present. Control of painlikely <strong>to</strong> improve overall function,including cognition.Seizure medicines Dilantin, Keppra, Depakote Control seizures. For most personswith TBI this is mainly usedearly in recovery. If no seizureshave occurred, the medication maybe able <strong>to</strong> be s<strong>to</strong>pped.Anti-spasticity medicines Baclofen, Zanaflex, Dantrium Control spasticity and spasms thatcause pain, limit function, or limitpositioning.Side EffectsExcessive stimulation, fast heartbeat, high blood pressureExcessive stimulation, changes inappetite, restlessness. Can causeincreased irritability at times.Nausea and sometimes excessivestimulationMay cause sedation and mentalslowing.Watch for s<strong>to</strong>mach problems, butgenerally well <strong>to</strong>lerated and shouldnot cause sedation.Can cause sedation, mentalslowing, and decrease inhibitionsleading <strong>to</strong> more behaviorproblems. A non-narcotic ispreferable over narcotic painmedication if at all possible.Sedation and mental slowing.Generally cause sedation andmental slowing in brain injury.Use with caution, but may alsowant <strong>to</strong> consider other treatmentslike Bo<strong>to</strong>x or Intrathecal Baclofen(ITB).
WINTER 2004/05page 7HEADLINESDate set for 20 th Annual Statewide Conference on <strong>Brain</strong> <strong>Injury</strong>Staff ReportMINNEAPOLIS - The <strong>Brain</strong><strong>Injury</strong> Association AnnualConference is now set for May20-21, 2005 at the St. CloudCivic Center. The conferenceplanning committee decided on“Bridging Islands” as this year’stheme. Keynote speakers for theevent include Dr. Al Condeluciand playwright/s<strong>to</strong>ryteller KevinKling.Dr. Al Condeluci is one ofAmerica’s leading consultants onhuman services and communityissues. He’s campaigned fora number of policy changesregarding people with disabilities,including the Americans withDisabilities Act of 1990.He speaks <strong>to</strong> national andinternational audiences reachingover 10,000 people each year.As United Cerebral Palsy (UCP)of Pittsburgh’s current executivedirec<strong>to</strong>r, Dr. Al Condeluci has28 years of service at UCP ofPittsburgh and is internationallyrecognized as a leader in humanservices.Condeluci is also a professorat the University of Pittsburgh’sSchool of Social Work and aMasters professor in NonprofitManagement at Robert MorrisUniversity. Three of his books,Interdependence (1991), BeyondDifferences (1995), and CulturalDr. Al CondeluciShifting (2001) are being usedin more than 100 colleges anduniversities. Dr. Condeluci’s latestbook, Advocacy for Change: AManual for Action, serves as ahands-on guide for communityactivists.Kevin Kling is a localplaywright, humorist, s<strong>to</strong>rytellerand stage performer. When hewrites, the details are usuallyspecific <strong>to</strong> the upper Midwest, buthis <strong>work</strong> is more of a universalexperience: full of childhoods<strong>to</strong>ries and <strong>to</strong>pical observations.Kling has the ability <strong>to</strong> capturethe many details of a moment injust a few words. As he explainsit, “I have a small command of theEnglish language so I try <strong>to</strong> makeeach word a hero.”A <strong>Minnesota</strong> native andgraduate of Gustavus AdolphusCollege’s Theatre Program,Kling has been awarded manyprestigious arts grants andfellowships including TheNational Endowment for the Arts,The McKnight Foundation, The<strong>Minnesota</strong> State Arts Board, TheBush Foundation and The JeromeFoundation. A central figure in theMinneapolis Theatre community,Kling has written over a dozenplays and adaptations. Kling is afrequent s<strong>to</strong>ryteller on NationalPublic Radio’s “All ThingsConsidered,” and has addressedKevin Klingdisability issues in many of hiscreative endeavors.The 2005 annual conferenceplanning is underway. Sponsorshipmaterials will be mailed in earlyJanuary. For more informationabout conference sponsorship andexhibit opportunities, call Ottarat 612-238-3235. To volunteer atthis event, contact the VolunteerCoordina<strong>to</strong>r, Kimberly Ferencik at612-378-2742.Helpingpatients rebuildtheir livesMayo Clinic Physical Medicine and Rehabilitationprovides comprehensive rehabilitation and medical servicesfor people with traumatic brain injury and other types ofacquired brain disordersWhy Mayo Clinic?• Level 1 Trauma Center• Only Midwest NIDRR* designated Traumatic<strong>Brain</strong> <strong>Injury</strong> Model System• Comprehensive outpatient and inpatientevaluation and treatment programs• Accredited by Commission Accreditation of RehabilitationFacilities (CARF) and Joint Commission on Accreditationof Healthcare Organizations (JCAHO)Mayo Clinic200 First Street SWRochester, MN 55905For more information contact:Program Secretary 507-255-3116*National Institute on Disability and Rehabilitation Research
HEADLINES WINTER 2004/05WAITINGfrom page 1people who come <strong>to</strong> us who havemarketable skills, but becauseof limitations associated withtheir disability, they are havingdifficulty accessing the job market.They might be involved withVR for less than a year. Thereare others who come who don’thave marketable skills and basedon their aptitudes and abilitiesand interests, they may involvethemselves in a four year collegeprogram,” said Paul Bridges,interim direc<strong>to</strong>r for rehabilitationservices for the Department ofEmployment and EconomicDevelopment (DEED), thedivision of the government tha<strong>to</strong>versees VR.In cases like Balken’s, personswith disabilities turn <strong>to</strong> VR <strong>to</strong>help determine if they can return<strong>to</strong> their profession at the samelevel as they were pre-injury, whataccommodations they would need<strong>to</strong> return <strong>to</strong> <strong>work</strong>, or if they can’treturn <strong>to</strong> the same job, what otheremployment or training optionsexist.To Balken’s surprise, hedidn’t qualify as a “priority one”candidate, and was <strong>to</strong>ld he mostlikely would not be served by VRat all.“We determine who is in whatpriority category based on howthe person gets along relative <strong>to</strong>seven areas of functioning. Anindividual has <strong>to</strong> have seriousfunctional limitations in terms ofemployment in three or more areasin order <strong>to</strong> be considered in thefirst priority group,” said RobertaPisa, direc<strong>to</strong>r of consumer andstaff services for DEED.The seven areas of functioningare mobility, self-direction,self-care, interpersonal skills,communication, <strong>work</strong> <strong>to</strong>leranceand <strong>work</strong> skills.“[Vocational Rehabilitation]seems like a great program foreveryone but me. I was <strong>to</strong>ld atmy last doc<strong>to</strong>r’s appointmentthat for the outside observer, I’mrecovering quite well. I can talkwell, I can move around okay. Butit’s the things that people can’t seethat are my main deficits. That’sthe hardest thing <strong>to</strong> cope with,” hesaid.Balken admits that he couldprobably land a low-skilled retailposition. “But I didn’t go <strong>to</strong>college for six years <strong>to</strong> do thatbecause I fell off a roof. It’s likeyou’re supposed <strong>to</strong> accept a lesserjob or lesser career, when youwouldn’t have <strong>to</strong> if you had a littlehelp, and it’s impossible <strong>to</strong> getback in<strong>to</strong> the swing of things allby yourself. That’s very hard <strong>to</strong>accept when all you want <strong>to</strong> dois return <strong>to</strong> being a productive,<strong>work</strong>ing person again.”Vocational Rehabilitation hasa long his<strong>to</strong>ry of successfullyassisting persons with disabilitiesin their return <strong>to</strong> <strong>work</strong>, and forthe first time, has been facedwith difficult decisions <strong>to</strong> makeabout their budget. VR instituteda waiting list for priority oneconsumers on January 15, 2004.Currently 2,600 priority oneconsumers and another 2,896consumers in priority two, threeand four are waiting for services.“It would be a bit of amisnomer <strong>to</strong> say that [prioritytwo/three/four consumers] areon the VR waiting list, becauseit is highly unlikely that we willbe able <strong>to</strong> provide them withtraditional, full VR services,” saidBridges.According <strong>to</strong> Bridges, thewaiting list is due <strong>to</strong> several yearsof flat funding from the federalgovernment, coupled with risingcosts in post-secondary educationand healthcare for staff.His<strong>to</strong>rically, a waiting listfor VR services goes back as faras 1993 (fiscal year 1994) whenthe priority categories were firstestablished. “Under federalregulations, we were instructed<strong>to</strong> establish a priority for serviceand a waiting list when we findourselves in a situation of notbeing able <strong>to</strong> serve all eligibleconsumers,” said Bridges.Between 1994 and <strong>to</strong>day,categories were progressivelyclosed for services, starting withcategory four, and put on a waitinglist. When fiscal year 2004 startedin Oc<strong>to</strong>ber 2003, VR continued <strong>to</strong>bring in priority one consumersuntil January 15 when the waitinglist was implemented. FromJanuary 15 through August 15, noone was taken off the list. SinceAugust, 300-600 consumers havebeen taken off monthly.The effects of the waiting listhave made a significant impact onpeople with disabilities and serviceproviders throughout the state.An office of empty chairsFive years ago when he openedOpportunity Partner’s office at theBlooming<strong>to</strong>n Workforce Center,Ray White described the office as“bustling” with a steady stream ofconsumers referred by VR. As asupportive employment vendor forVR, Opportunity Partners providesthe employment counseling andjob coaching necessary <strong>to</strong> getconsumers back in the <strong>work</strong> force.When the waiting list wasimplemented for VR services,White witnessed a dramatic dropin activity. “It was a slow processand it just continued throughoutthe year until finally, when Iwould walk in<strong>to</strong> the office in themorning, the chairs where clientsused <strong>to</strong> wait <strong>to</strong> see counselorswere vacant,” he said.White is very concerned aboutthe lasting ramifications causedby the waiting list. “The waitinglist discourages applicants. Theconcern is there are individualsout there that are not accounted forwho will not receive assistance.When they hear that there is awaiting list, and that they mightnot even get served, they think,why even apply?”The gap in employment his<strong>to</strong>ryis a typical barrier <strong>to</strong> employment,said White. The waiting listincreases that gap. “As clientswait, their job his<strong>to</strong>ry becomesextremely damaged. This is reallygoing <strong>to</strong> hinder serving clients,” hesaid.The waiting list alsoexacerbates emotional barriers <strong>to</strong>employment. “[It] depletes thepositive energy and motivationneeded for a successful job-hunt.Those with mental illness likedepression can be affected in avery negative way. A lot of thefolks coming <strong>to</strong> us for assistancehave a motivation problem, andwe have <strong>to</strong> fire them up and reallycreate an interest in where theywant <strong>to</strong> go, where they want <strong>to</strong>be. Without that help, this reallydoubles the [negative] effect,” saidWhite.White says that the waitinglist has forced his organization<strong>to</strong> think creatively on how it canmeet the needs of the persons withdisabilitie. One of the servicesOpportunity Partners now offers isa private pay option for supportiveemployment. Five families haveopted for this service and twojob placements were made fairlyquickly.“[The waiting list] is going <strong>to</strong>make agencies like ours shuffle,reorganize and maybe come upwith some different programs,”said White.Mayo Makes AdjustmentsRachel Scanlan hasalso reshuffled the way shedoes her job. As VocationalCase Coordina<strong>to</strong>r for MayoMedical Center’s <strong>Brain</strong> <strong>Injury</strong>Rehabilitation and ResearchPrograms, Scanlan’s <strong>work</strong> hasalways been tied closely with VRservices.Typically, Scanlan getsinvolved with consumers early intheir rehabilitation process, longbefore they are ready <strong>to</strong> go back<strong>to</strong> <strong>work</strong>. By getting involvedearly, she helps shape the therapyprocess <strong>to</strong> meet the employmentneeds of the consumer.Many of Scanlan’s consumersdo not have a job <strong>to</strong> go back <strong>to</strong>, orthe job they had was filled due <strong>to</strong>the length of their absence. Thispage 8is where community supports arecritical. One of the most importantservices Mayo accesses throughVR are the <strong>work</strong> trials or “job tryouts.”“It’s an opportunity for people<strong>to</strong> go out and <strong>work</strong> a job for ashort period of time with theassistance of a job coach. It maybe an area of interest, or it may besimilar <strong>to</strong> a former job that theyonce held and they wanted <strong>to</strong> seeif they did indeed still have theskills. It’s part of the evaluationphase, so an employer is no<strong>to</strong>bligated <strong>to</strong> hire them, so there isno pressure there. If the persondoesn’t do well, it’s okay becausethey didn’t actually go out in<strong>to</strong>the real world of <strong>work</strong> and burna bridge by being terminated orhaving other problems,” saidScanlan.Because of the closeconnection <strong>to</strong> VR, Scanlan’s <strong>work</strong>has been dramatically affectedby the waiting list. “We havepeople that have gone throughour program and are all geared up<strong>to</strong> <strong>work</strong>, but need more support.They need some evaluation or<strong>work</strong> trials or they might needsome training. But when thatresource isn’t there, there is a hugegap. So it’s changed the way I domy job. As soon as I’m seeingpeople, even as early as the initialconsultation, I’m getting them setup with VR. I have <strong>to</strong> explain,well, you’re not ready <strong>to</strong> <strong>work</strong>,you’re not really ready <strong>to</strong> do thesevocational things, but because ofthe waiting list, I need you <strong>to</strong> setup a meeting [with VR] and we’llgo through the intake <strong>to</strong>gether,”she said.Scanlan has also relied moreheavily on county servicesas a result of the waiting list.However, <strong>Minnesota</strong> counties arelimited in what they can fund, andwaiver programs aren’t of help<strong>to</strong> people that are not eligible forMedicaid or public assistance.“It is very confusing for folksand cause us a great deal of stressas well, partly because the waiverprogram is supposed <strong>to</strong> be thepayer of last resort. VocationalRehabilitation is supposed <strong>to</strong> payfor the evaluation, and you can’tuse waiver dollars until that’shappened. If you can’t get that <strong>to</strong>happen, people are going withoutservices and that’s been frustratingfor a lot of folks,” said CharityFloen, home and community careprogram manager for OlmstedCounty, where the Mayo MedicalCenter is located.The importance of advocacyScanlan, White and Balken allstress the importance of speakingWAITINGon page 9
WINTER 2004/05page 9WAITINGfrom page 8up.“This is important stuff. Theseare people that want <strong>to</strong> go back<strong>to</strong> <strong>work</strong>, people who need <strong>to</strong> goback <strong>to</strong> <strong>work</strong>. These are youngpeople – people who should not besitting for the next several yearsnot <strong>work</strong>ing,” said Scanlan. Shepractices what she preaches, andhas been involved in advocacyfor VR services at the local andfederal level.Scanlan is thrilled with theincreased level of responsefrom her consumers. “I’ve seenpeople that probably never wouldhave been active in voicingtheir concerns, talking <strong>to</strong> theirlegisla<strong>to</strong>rs. We encourage people<strong>to</strong> do that. I think it often carriesso much more weight than me asa professional saying ‘you need <strong>to</strong>fund this, we need more money.’There’s more power when a personsays ‘hey, I want <strong>to</strong> <strong>work</strong>, I’mready <strong>to</strong> go, I need this service, butit’s not there.’”White encourages involvementby urging consumers <strong>to</strong> get on thewaiting list. “Whenever I get aphone call about services, I ask[the consumer] <strong>to</strong> please, pleaseput their name on the list, becausethey never know when somethingmight come along. Do whateveryou can, keep stirring the pot, keepthings in motion and don’t quit.”Balken has gotten involvedby attending the <strong>Brain</strong> <strong>Injury</strong>Association of <strong>Minnesota</strong>’Legislative Home Visit inhis district. “I sat next <strong>to</strong> myrepresentative during the meeting.He couldn’t believe what I wasgoing through,” he said.White worries about the longtermeffects the VR waiting listwill have on society. “I can’t helpbut believe that if these peoplearen’t being served somehow,someway through the state of<strong>Minnesota</strong>, it’s going <strong>to</strong> comeout some other way. Either theywill end up on the streets, in thehospital, in mental institutions orin prison. I just see the costs beingincurred elsewhere. We all havelimitations and assets and skills.If we’re not going <strong>to</strong> be protected,what does this mean for society asa whole?”“If you don’t say something,funding for VR and services like itwill go away,” said Scanlan.HEADLINESTips for Conquering the <strong>Waiting</strong> List Woes1. Get on the List! Don’t let the thought of a waiting list discourageyou from applying for vocational rehabilitation services. Makesure that you document any deficits or barriers <strong>to</strong> employmentbefore attending the intake meeting, so that you can clearlyarticulate your needs.2. Help create a demand for service. If you don’t qualify forpriority one, make sure that you are categorized as two, three orfour and put on the appropriate list. Your presence on the waitinglist demonstrates a demand for services.3. Become a Citizen Advocate. Contact your state and federallegisla<strong>to</strong>rs and share your s<strong>to</strong>ry. Write letters, make phonecalls, send emails, and if possible, arrange in-person meetings.Hearing from professionals in the brain injury field will nevercarry the same power with lawmakers as hearing a personals<strong>to</strong>ry from their constituents. Contact Shannon Robins at the<strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong> for more information atshannonr@braininjurymn.org or by phone at 612-378-2742, or1-800-669-6442 in greater <strong>Minnesota</strong>.4. Contact a Resource Facilita<strong>to</strong>r at the <strong>Brain</strong> <strong>Injury</strong> Associationof <strong>Minnesota</strong> for assistance. They can help problem-solve andconnect you <strong>to</strong> other resources in your community. Call thephone numbers listed above and ask for the Resource Facilita<strong>to</strong>rthat serves your area of the state.5. Volunteer. Volunteering can help you build up marketableskills, provides a valuable source of feedback about your jobperformance, and allows you <strong>to</strong> “test the waters” for returning <strong>to</strong><strong>work</strong>. Check out Volunteer Match at www.volunteermatch.org.Don’t want <strong>to</strong> hassle with a volunteer search over the internet?If you live in the Twin Cities Metro area, contact the VolunteerResource Center at 612-379-4900. For volunteer opportunitiesat the <strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong>, contact KimberlyFerencik at kimberyf@braininjurymn.org or at the phonenumbers listed above.
HEADLINES WINTER 2004/05WALK FOR THOUGHTfrom page 1Association’s growing capabilities<strong>to</strong> reach a broader audience.The Dragonfly Clan, leadby Team Captain Tracy Winkel-Johnson, held <strong>to</strong> her promise <strong>to</strong>become the <strong>to</strong>p fundraising teamfor 2004. The Dragonfly Clanraised over $5,100.“My inspiration for fundraisingfor the Walk for Thought wouldhave <strong>to</strong> be my brother, Steve,who we lost <strong>to</strong> a brain injury.Participating in the Walk, reallythrowing myself in<strong>to</strong> it, seems likea good way for me <strong>to</strong> positivelyhonor my brother’s memory andkeep his spirit alive while alsodoing something <strong>to</strong> help others,”said Winkel-JohnsonTwo teams raised over $3,000:Region’s Hospital and KeepingAhead. Craig’s Cracked Cranium,the Mindful Mayo Walkers, Spin<strong>to</strong> Win, Stampeding Turtles, TeamEclectic, Team Nichole, TeamOttar and the Montes are teamsthat raised over $1,000.Top fundraising individualswith over $500 a piece includeKristi Buschke, Byron Wills,Deborah Wagner, Craig Martinson,Sue Winkel, Tracy Winkel-Johnson, Tom Bang, Mike Carter,Sue Larsen, Denny Anderson,Judy Vallancourt-Yerhot, TerrySandstrom, Shannon Robins,Connie Schmitz, Tawnya Panek,Kathy Puetz, Sharon Christensenand Amy McVary.All proceeds from the walkwill directly benefit the <strong>Brain</strong><strong>Injury</strong> Association of <strong>Minnesota</strong>’smultiple services and programsthat serve persons with braininjury.Picture galleries from thisyear’s walks in Phalen andBlackduck, including teampictures from the Phalen walkare available on the Associationwebsite.Thanks <strong>to</strong> our participants,sponsors, volunteers, staff, WalkCommittee and board of direc<strong>to</strong>rsfor their support and commitment<strong>to</strong> bring hope, help and a voice<strong>to</strong> the 94,000 <strong>Minnesota</strong>ns wholive with a disability due <strong>to</strong> braininjury. The Walk would nothave been as successful withouteveryone’s involvement. Thesteps we <strong>to</strong>ok during the Walkfor Thought will help thousandsof <strong>Minnesota</strong>ns affected by braininjury achieve even greater stridesof their own.Watch the Association website, www.braininjurymn.org, inthe coming months for details onnext year’s walk.page 10picture by Sharon RolencAlicia Warden, senior at Blackduck Highschool, organized the Blackduck Walkfor Thought, under the guidance of retired Blackduck High school teacher ShirleyDeno.picture by Carrie StewartVolunteers of all ages turned out at the walk <strong>to</strong> help with set-up, registration,pictures and the water station.Special Thanks <strong>to</strong> Our Sponsors!pictures by Sharon RolencWalkers take a break from the 2004 Walk for Thought <strong>to</strong> pose for a scenic pictureWith Additional support from:American Family InsuranceIntegrity LivingMiller-Dwan Rehabilitation CenterMeshbesher & SpenceFaribault FoodsBlaine Chiropractic CenterBerger AlliedRSAHauer, Farigone, Love, Landy & McEllistrem,PATBI Metro Services (a service of OpportunityPartners)Regions Hospital/Health Partners
WINTER 2004/05page 11HEADLINESLEGISLATIVE CORNERKeeping up <strong>to</strong> date with public policyThank you <strong>to</strong> all who participated in Legislative Home Visits!By Shannon RobinsThe <strong>Brain</strong> <strong>Injury</strong> Associationof <strong>Minnesota</strong> would like <strong>to</strong> extenda special thank you <strong>to</strong> those verydedicated people who helped <strong>to</strong>coordinate and host LegislativeHome Visits in their communities.Thank you also <strong>to</strong> those who<strong>to</strong>ok the time <strong>to</strong> participate andcourageously share their s<strong>to</strong>ries atthe Legislative Home Visits.The information gathered fromparticipants at Legislative HomeVisits creates the foundation forthe <strong>Brain</strong> <strong>Injury</strong> Association of<strong>Minnesota</strong>’s Legislative agendafor the upcoming session while thecoalition <strong>work</strong> that the Associationis involved in helps <strong>to</strong> focus andshape the policy initiatives.The people who came <strong>to</strong>the Legislative Home Visits(952) 985-0672and shared their s<strong>to</strong>ries andperspectives were repeatedly <strong>to</strong>ldby legisla<strong>to</strong>rs across the state thatthe input they received at the Visitswill greatly impact the legisla<strong>to</strong>rs’ability <strong>to</strong> protect the servicesand supports that are important<strong>to</strong> their constituents whose livesare impacted by brain injury.However, the elected officials alsowarned participants that they need<strong>to</strong> consistently and continuallyspeak-up about the decisions beingmade at the Capi<strong>to</strong>l during session.Based off of the informationgathered at the Legislative HomeVisits and through coalitioninvolvement, the <strong>Brain</strong> <strong>Injury</strong>Association of <strong>Minnesota</strong>’slegislative initiatives will addressconcerns raised about a broadspectrum of issues.These issues include thingslike: Vocational RehabilitationIf your family currently receivesPCA (Personal Care Assistant) or nursing services,now your staff can start <strong>work</strong>ing for better pay.Our home care company offers the highest pay forPCAs, RNs and LPNs in <strong>Minnesota</strong>.and job supports, MedicalAssistance (MA) Home andCommunity Based Waivers(Traumatic <strong>Brain</strong> <strong>Injury</strong> (TBI)and Community Alternatives forDisabled Individuals (CADI)Waivers), passage of a primaryseatbelt law, res<strong>to</strong>ring the SpecialEducation funding, limiting theuse of Aversive and DeprivationProcedures and the use of lawenforcement in schools, repealingthe co-payments for MedicalAssistance prescription drugs andmedical visits, and repealing the$500 limit on Dental Servicescovered under MA.As <strong>Minnesota</strong> enters anotherlegislative session with a projectedbudget deficit of over $700 millionbefore inflation (about $1.4 billionwith inflation), the disabilitycommunity will be targeted forfurther cuts and restrictions ineligibility for the services andsupports that are needed. Morethan ever, we need <strong>to</strong> be vigilant inour efforts <strong>to</strong> protect those servicesand supports that are state fundedand continually educate ourelected officials about the benefitsthat these services provide.As our elected officials arefaced with the daunting task ofbalancing a continually decreasingbudget with steadily increasingdemands, we need <strong>to</strong> rememberthat they are humans and canonly protect what they are able<strong>to</strong> make the case for <strong>to</strong> otherlegisla<strong>to</strong>rs and the Governor. Theother thing <strong>to</strong> keep in mind is thatthe Association, along with otherdisability advocates, will have <strong>to</strong>concentrate on highlighting andsupporting the programs that helpthe state save money.The Association is dedicated<strong>to</strong> keeping its Citizen Advocatesinformed of what issues are beingdiscussed, as well as when andhow <strong>to</strong> make an impact at crucialtimes during this session. If youhave not already done so, pleasesign-up <strong>to</strong> be a Citizen Advocate<strong>to</strong>day so that we can keep youinformed.Communication with CitizenAdvocates is primarily donethrough email, so if you do nothave email access, we will stillkeep you posted during ActionAlerts, but will not be able<strong>to</strong> update you weekly. Pleasecontact Shannon Robins <strong>to</strong>day atshannonr@braininjurymn.org or612-378-2742 <strong>to</strong> learn more aboutbeing a Citizen Advocate.Member ofWE PAY$11/hr for PCAsRN up <strong>to</strong> $26/hrLPN up <strong>to</strong> $19/hrWe offer: $100 sign-up bonuses for the families $100 referral bonusWe have experienced PCAs, RNs and LPNs availablefor a variety of your staffing needs!For additional information, please contact our offi ce at:(952) 985-0672Myrna Yenter, MS, LICSWMental Health Services1719 Kathleen DriveNorth Manka<strong>to</strong>, MN 56003Phone and fax: 507-345-5281Myrna has had extensive experiencewith survivors of traumatic brain injury andtheir families. She has experienced TBIin her immediate family.Myrna does complete mental health servicessuch as counseling for couples, families,for anxiety and depression.
HEADLINES WINTER 2004/05Make Room for Creative Errors:Aphasia, Poetry and Making Sense of it Allpage 12By Elizabeth Sowden“Why this distracted talk?It’s not my fault I rave.You did this.Do you approve of my lovemadness?”—from The Essential Rumi,translated by Coleman BarksThis stanza comes from Rumi,a legendary Sufi poet who livedand wrote in the thirteenth century.Rumi addresses God in this stanza,but for persons with aphasia andtheir family members, these wordscan be all <strong>to</strong>o familiar. The wordscoming out of an aphasic person’smouth may be long strings ofmeaningless sentences, or theymay be short clipped phrases thatcan signify any variety of actions,statements, commands or desires.Caring for a person with aphasiacan seem like a surreal nightmare.Can he understand a word I say? Ihave no idea what she wants; doesshe even know? It’s critical forfamily members of a person withaphasia <strong>to</strong> remember one thing:though the words may not comeout right, having aphasia does notentail madness.Aphasia is a condition thatresults from brain injury, usuallyin the aftermath of a stroke.The portions of the brain wherelanguage and linguistic abilityare s<strong>to</strong>red are injured, creatingdifficulty with language, includingspeech, comprehension, and theability <strong>to</strong> read and write. DonMacLennan, Speech Pathologistat the Minneapolis VA MedicalCenter, defines aphasia as “adisorder of language.” Injuries thatcause aphasia usually leave thefrontal lobe intact. “The frontallobe is like a ‘conduc<strong>to</strong>r,’ on atrain. It interacts with memoryand controls attention. [Peoplewith aphasia] can understandfunctionally,” said MacLennan.There are three main typesof aphasia—fluent, non-fluent,and global. Fluent, or Wernicke’s,aphasia is exactly what it soundslike: a person with fluent aphasiacan speak in long, flowingsentences that have correctgrammatical structure, but thewords the person uses mightbe made up, nonsense words.Persons with fluent aphasia areoften completely unaware of theirdifficulties.Non-fluent, or Broca’s,aphasia, is the exact oppositeof fluent aphasia. Persons withnon-fluent aphasia speak in twoword phrases, such as “walk dog,”which can mean “I am going <strong>to</strong>take the dog for a walk,” “You gotake the dog for a walk,” or “thedog is walking.” Persons with nonfluentaphasia are often very awareof their difficulties, which can bevery frustrating for them.Persons with globalaphasia have severe difficultieswith communication, and arevery limited in their ability <strong>to</strong>comprehend and speak. There isalso what is called anomic aphasia,which means that the individualhas difficulty remembering certainwords, particularly the names ofthings.Additionally, there is Landau-Kleffner Syndrome, which is achildhood disorder that includesthe gradual or sudden loss ofthe ability <strong>to</strong> understand anduse spoken language. Eightypercent of children with Landau-Kleffner Sydrome (LKS)experience epileptic seizures,occurring mostly at night. Manybehavioral disorders accompanyLKS, including hyperactivity,aggressiveness, and depression.LKS may also be referred <strong>to</strong>as Infantile Acquired Aphasia,Acquired Epileptic Aphasia, orAphasia with Convulsive Disorder.It’s overwhelming, right? Nomatter which one of these types ofaphasia your loved one has, youwill find it extremely challenging<strong>to</strong> care for him or her. The loss oflinguistic ability is a devastatingone. We all <strong>to</strong>o often judge theintelligence of others based ontheir language skills, which, asyou may be discovering now, isinaccurate.“Language is a <strong>to</strong>ol. It’snot absolutely required. Peoplewith aphasia usually have goodmemory and reasoning…aphasicpeople know what the point is,”said MacLennan.Language is one of thosethings we take for granted—oneof those things we hurt badly foronce it’s gone, one of those thingsthat causes us <strong>to</strong> grapple withmeaning as we recover from theshock of losing something so vital,something so inherent within us.We may not realize all the thingswe do with language until we can’tdo them any more: the comedianloses his ability <strong>to</strong> tell jokes,the cynic her ability <strong>to</strong> processsarcasm, or the writer his ability <strong>to</strong>turn the blank page in<strong>to</strong> a s<strong>to</strong>ry orpoem with a life of its own.We may not realize all the things we do with language until wecan’t do them any more: the comedian loses his ability <strong>to</strong> tell jokes,the cynic her ability <strong>to</strong> process sarcasm, or the writer his ability <strong>to</strong>turn the blank page in<strong>to</strong> a s<strong>to</strong>ry or poem with a life of its own.You have lost somethinghere <strong>to</strong>o: your loved one’saccomplishments you once <strong>to</strong>okpride in are no longer possible. Apart of the way you interacted witheach other, such as humor, is nowgone. Perhaps this change placesa strain on your relationship. Youmight be thinking, “What do wedo now?”Perhaps the most positive stepyou can take is <strong>to</strong> view your lovedone’s aphasia as a gift. In heressay, “Celebrating Aphasia PoetryPower,” Chris Ireland, a poetwho has aphasia, writes “BeforeI published [my poetry] in thejournal, I discussed with the edi<strong>to</strong>r.She was correcting. I explainedthat these are not spelling errors,but ‘creative errors’ <strong>to</strong> showaphasia.”Here’s an example of oneIreland’s creative errors: ‘insidemy own rhymns/internal rhymn.’In the word ‘rhymn,’ there’sa clear fusion of the words‘rhyme’ and ‘hymn,’ whichcan be interpreted in indicate acelebration of poetry, of words,and of ‘creative errors’ that comefrom aphasia. The aphasic mind isstill a creative mind, a mind stillcapable of profound meaning.Also, just because somethingdoesn’t make sense doesn’tmean it’s not beautiful. In “TheCreative Process: Reflectionson the Invention of Art,” thepoet AE Housman wrote: “EvenShakespeare, who had so much<strong>to</strong> say, would sometimes pourout his loveliest poetry in sayingnothing…[it] is nonsense, but itis ravishing poetry.” Learn <strong>to</strong> findbeauty in the nonsensical and thedisorderly. Make room for creativeerrors in your life.According <strong>to</strong> MacLennan, theone of the best things you can doif you feel you’re having difficultyaccepting and understanding thechanges that come with aphasiais education. Learn all you canabout aphasia, be creative withcommunication techniques, andremember that when your lovedone makes an error in speech, donot correct him, for if he has nonfluentaphasia, it will only frustratehim, and if he has fluent aphasia,he may not understand why youare correcting him.For more information,check out the National AphasiaAssociation’s website, www.aphasia.org. This website hasarticles, information on research,and contains information inSpanish, Haitian-Creole, Russian,and Chinese. “Aphasia Inside Out:Reflections on CommunicationDisability” has essays written byindividuals with aphasia, includingthe one by Chris Ireland. It’s anenjoyable read, and it’s full ofinformation that will provide youwith very useful insight.“Take language out of theequation,” said MacLennan, andyou’ll see the same smart, funny,caring person you’ve alwaysknown.The Write Aid Encourage persons withaphasia <strong>to</strong> write. Thoughwriting may be difficult now,encourage them <strong>to</strong> view it ina new way—allow them <strong>to</strong> letpoetry show them what theyare capable of. (According <strong>to</strong>MacLennan, “It can’t hurt. Itmight not be therapeutic …butit can’t hurt.”) Children with Landau KleffnerSyndrome who learned <strong>to</strong>write before the onset of LKSmay still be able <strong>to</strong> write, soencourage your child <strong>to</strong> writeas much as possible <strong>to</strong> alleviatesome of the frustration yourchild may have with oralcommunication. Keep a journal of your ownfeelings, frustrations anddesires. It’s your privatewriting so don’t hold back.Your feelings are valid <strong>to</strong>o—once you get them out, you’llbe able <strong>to</strong> deal with them and itwill be better for you and yourloved one. Try writing your own“aphasia” poetry with creativeerrors—write down any wordthat comes <strong>to</strong> mind, even ifit’s a nonsense word. Do thisnot only for the satisfaction ofcreating but also <strong>to</strong> help youget used <strong>to</strong> the idea that notmaking sense isn’t a bad thing.
WINTER 2004/05page 13HEADLINESBlood test being developed for TBI diagnosisBy Kelly ParadisAny fan of science fictionknows that in the future, doc<strong>to</strong>rswill be able <strong>to</strong> quickly scan theirpatients with a handheld <strong>to</strong>ol anddetermine instantly what is wrong.In the case of traumatic braininjury, the future may be rightaround the corner. Researchershave been developing a simpleblood test <strong>to</strong> confirm that someonehas sustained a traumatic braininjury (TBI) and even the degreeof injury.When the brain is injured,scientists are discovering that thereare distinct protein patterns thatemerge around the injured tissue.Researchers at the University ofNorth Carolina at Chapel Hillfound that the scar tissue thatforms on the brain or spinal cordafter an injury prevented healingand regeneration of cells.This scar tissue contains aprotein called palladin, whichUNC researchers first identified in2000. Palladin seems <strong>to</strong> controlthe way that cells regenerate in aninjured area of the brain and alsoserves as a marker pinpointingthe injured area, with more cellsshowing up around the damagedarea.One challenge of TBI isidentifying it quickly so thatthe injured person is given theappropriate treatment. Currenttests using computed <strong>to</strong>mography(CT) scans and magneticresonance imaging (MRI) can beexpensive and inaccurate. Plus,they may not be readily available<strong>to</strong> some patients, depending wherethey live.While testing for brain injurythrough protein markers wouldbe a welcome addition <strong>to</strong> anytraditional medical practice, itbecomes a lifesaving <strong>to</strong>ol in thehands of a field medic in themilitary. <strong>Brain</strong> injuries are anunfortunate reality in military lifeand being able <strong>to</strong> quickly identifyand treat wounded soldiers andcivilians can mean the differencebetween life and death. This isespecially true in triage situationswhen limited resources meanschoosing who will get medicalhelp immediately.Banyan Biomarkers (www.banyanbio.com) is one group thatis focusing on developing fieldtesting for the military. According<strong>to</strong> Banyan’s website, nearly half ofall combat deaths are the result ofhead injuries. The improvementsin soldier body armor and medicaltreatment, while increasing thesurvival rate of the soldier, hasalso led <strong>to</strong> an increase in TBIamong the wounded. Injuriesthat would have been fatal in thepast no longer are, but many areleft struggling with the lingeringeffects of brain injuries.According <strong>to</strong> the Center forDisease Control, at least 5.3million Americans are living witha disability from a TBI. Over300,000 sports-related braininjuries occur each year. Many ofthe symp<strong>to</strong>ms are subtle or don’tappear right away. Often theeffects of the injury make it hardfor the person <strong>to</strong> realize or admitthat they are having a problem thatmight be brain-related.Some common symp<strong>to</strong>ms,like feeling tired, unmotivated andhaving a hard time sleeping arealso seen in people experiencingdepression or other illnesses.Tools like the protein-detectingblood test should quickly clearup any confusion by identifyingwhether it is a brain injury at faultand giving persons with braininjury the diagnoses they need <strong>to</strong>manage their recovery.Interesting inBecoming aVOLUNTEER?CallKimberlyFerencik at612-378-2742 Call us at 763-427-8888 www.soucielaw.com
HEADLINES WINTER 2004/05page 14Association Volunteers contribute over 3,000 hours in 2004The <strong>Brain</strong> <strong>Injury</strong> Associationof <strong>Minnesota</strong> is the only nonprofi<strong>to</strong>rganization in the state dedicatedsolely <strong>to</strong> serving the needs of the94,000 <strong>Minnesota</strong>ns who livewith a disability due <strong>to</strong> braininjury. Our mission is <strong>to</strong> create abetter future though brain injuryprevention, research, educationand advocacy.In order <strong>to</strong> fulfill its mission,the Association relies on a greatgroup of volunteers who <strong>work</strong> ina variety of roles, from transla<strong>to</strong>rs<strong>to</strong> receptionists, event set up <strong>to</strong>data entry. Volunteers contributedmore than 3,000 hours in 2004!The following people havewarmly contributed their timeand talent <strong>to</strong> support persons withbrain injury and their families in2004. For their continued support,the <strong>Brain</strong> <strong>Injury</strong> Association of<strong>Minnesota</strong> sincerely thanks ALLof them:Kathy AndersonSheldon AndersonMary Jo AvendañoJessica AwaiganeJudi AzarOt<strong>to</strong> BangHeather BarberThe Beck FamilyPatricia BergstromWyatt BienfangRichard BloomAnnemarie Bolat<strong>to</strong>Dave BrackettKristi BrackettClaire BrandesSydney BrandesKen Brit<strong>to</strong>nDavid BulfordEmily CarlsonNancy CarlsonErwin ConcepcionNeal CrispDART TransitNicholas DennenShirley DenoDenise DillonJeanne DirksonCharles DugganSherry DvorakChar ElioffGale ErdmannCaroline EstradaSusan ForsythRosemary FroehleBarbara Ful<strong>to</strong>nJennifer GeisenSarah GillTina GjerstadAmy GodeKim Gulbransen HearstJob GuzmánFloyd HaleJulie HartungJohn HelmersLaurie HelmersGretchen HelvorsonLeah HolmesNicole HolzworthBecky HooperDawn HoschetteJulie HudallaLyndsay HuntKim JahnkeLindsay JarombekBill JeronimusScott JohnsonWillis JohnsonAneisa JonesKim KangRobert KarolJoann KenersonJanis KeyesTodd KimlingerKathryn KohnertHolly KostrzewskiAmanda KrieselJulie KrieselRob KrieselSusan KujawaHelp Persons with <strong>Brain</strong> <strong>Injury</strong>and Their Loved OnesVolunteer <strong>to</strong> help with <strong>Brain</strong> <strong>Injury</strong> Basics ClassesThe <strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong> is looking for a friendlyoutgoing person <strong>to</strong> assist with “<strong>Brain</strong> <strong>Injury</strong> Basics” (BIB) classesby preparing refreshments, helping with room set up and greetingparticipants as they arrive at our office. This volunteer is key <strong>to</strong>providing a welcoming, helpful environment for class participants,many of whom are persons with brain injury and their familymembers. We need a volunteer from 4 pm – 6:30 pm the thirdTuesday of every month and ask for a six month commitment.This is a great opportunity for youth 14 or older or for a parent andchild (age 7+) <strong>to</strong> volunteer <strong>to</strong>gether. There is free parking and weare near a bus route. The <strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong>is committed <strong>to</strong> providing a friendly, supportive, professionalexperience for its volunteers. If interested, contact the VolunteerCoordina<strong>to</strong>r at 612-378-2742 or kimberlyf@braininjurymn.org.For a listing of other volunteer opportunities, visit the Associationwebsite at www.braininjurymn.org.Ellen KuschkeJim LandRobin LandySusan LarsenGwyn LederToni Lee-JohnsonSue LeporeRichard LordJohn LuciaGail LundeenCarrie MacNabbJacqueline MartinCraig MartinsonMary MeesterSue MeserowMargo MilletteMargaret MossAdau<strong>to</strong> MouraoRicardo MouraoJennifer MundlGreg MurreyJoe MyersDianne NausCarrie NelsonNikki NelsonJoan NickellsStanley NickellsShalonda NickensLaurie OlivierLori OlsonMark OrlandoJennifer OschwaldKelly ParadisAnnette PearsonCheryel PerezIvy PetersonRuss PhilstromAlan PorcielloRADD BMX & Skate TeamJordan RaneyRobert ReedySandra RobertsonJon RoeslerKeegan RolencTimothy RosePatricia RudolphWISH LISTAngela RutgersonSalwa SalahBrian SammonLaVonta SandersTerry SandstromNatalie SchmitDave ScottTerri ScottKate ShannonJudy SiemsSingle Volunteers Twin CitiesElizabeth SkinnerLinda SlatteryRich SlatterySandra SmithJulia SochaDarshan SoskeElizabeth SowdenJayne SpainKris Staple<strong>to</strong>nCarrie StewartMike StrandTBI Metro ServicesJulie TestaTim TiniusTerri TraudtMalai TurnbullRobert Ver StraetenVET SchoolMerrie VisteAlicia WardenPatty WhiteHeidi WilcoxTanika WilliamsDeb WilliamsonAndrea WingetCaroline WingetDavid WingetPat WinickBen WolfeJudy YerhotJeff ZinnOur sincerest apologies <strong>to</strong> anyonewhose name we accidentallyomitted.We welcome a variety of in-kind donations at the <strong>Brain</strong><strong>Injury</strong> Association of <strong>Minnesota</strong>. The following are afew of our immediate needs: IBM compatible computers – 500mhz or better,256RAM or better, 6 gig hard drive or better Computer accessories including anti-glare screens,keyboard trays, wrist rests and power strips Scanners Laser printers Copier Tickets <strong>to</strong> local events (sports, theater, music, etc.)<strong>to</strong> use as volunteer thank you giftsIf you would like <strong>to</strong> donate these or other items, pleasecontact Mark or Kimberly at 612-387-2742. Thanks!
WINTER 2004/05page 15HEADLINESSPONSORSAcknowledgement of Donations: August 16 - November 15, 2004MEMBERSDONORSProWorks, Inc.Mr. Martin AllenMr. James AshleyMs. Deborah AurianivarMs. Linda BeaucheneMs. Kellie ConlanMr. Steven GrohoskiMrs. Donna JohnsonMs. Judy KlevenMr. Mark OlsonMr. Mica SchaffranMs. Melanie SchroederMr. Dave Scott, TBI MetroServicesMrs. Elizabeth ShippeeMs. Kristina TierneyMr. Glenn TridgellDr. Gale Valtinson Bethesda RehabilitationHospitalDr. Nancy Wagner, Gillette Children’sSpecialty HealthcareMs. Marlys WagnerMs. Julie WruckCORPORATIONSWestern Insurance Agency, Inc.FOUNDATIONSUPS FoundationMedtronic FoundationDONATEYOUR CAR!Mr. Jim BeckerMr. & Mrs. William CampbellMs. Sherrie Fischer-WestMr. & Mrs. William FoxMrs. Marjorie GoldbergDr. Eric GoullaudMs. Jan HansonMr. & Mrs. Richard HowellMr. Howell JohnsonMr. Leroy MatherMr. Jim McArdellMs. Susan MencelMs. Sarah MoellerDr. & Mrs. John NilsenMs. Anne OtteMr. & Mrs. Frank PlantMr. & Mrs. Steven SchachtmanDr. Tim TiniusUnknownMs. Mary Ellen VetterMr. & Mrs. Fred WeinerORGANIZATIONSCommunity Solutions FundUniversity of IllinoisTRIBUTESIn honor of the 50th Anniversaryof June & Pete MedernachMr. Matthew MorelliTurn your used car in<strong>to</strong> cashfor the Association.For more information,visit www.donateacar.comor call Mark at 612-378-2742.Name:Address:City:State, Zip Code:Telephone:Email: Individual: $35 Limited income: $5-15 Professional: $50 Benefac<strong>to</strong>r: $250I am (please check one): A person with brain injury Family member/friend ProfessionalSign me up for: Headlines Online, a freeelectronic newsletterpublished bi-weekly.Payment Method Check payable <strong>to</strong> <strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong> Credit Card: Visa MastercardCard Number:Expiration Date:Signature of Cardholder: Non-profi t organization: $250 Corporation: $500 Individual Lifetime: $1,000 Other: $Please note that the process takes up <strong>to</strong>two weeks and the Association cannots<strong>to</strong>re your car.Complete form and send <strong>to</strong>:<strong>Brain</strong> <strong>Injury</strong> Association of <strong>Minnesota</strong>34 13th Ave NE, Suite BOO1, Minneapolis, MN 55413
HEADLINES WINTER 2004/05Judging by Matt’s strides, there's no telling. Physical therapy gave him the power <strong>to</strong> takethe first step beyond a severe brain injury. But it's extraordinary devotion that res<strong>to</strong>red hisultimate source of strength – his faith. And on the road <strong>to</strong> recovery, that’s a force wedraw from every step of the way.page16MEDICINEfrom page 6the most common. Youshould speak with yourtreating doc<strong>to</strong>r about anyconcerns related <strong>to</strong> themedication routine currentlybeing used. If there is stilla concern your doc<strong>to</strong>r canrefer you <strong>to</strong> a physicianknowledgeable in braininjury treatment and the useof these medications.Dr. Kenneth R. Brit<strong>to</strong>n,DO, is the president andfounder of Brit<strong>to</strong>n Centerfor Spine, Sport, andNeurologic Rehabilitation.He is board certifi ed inphysical medicine andrehabilitation, and his areasof specialty include physicalmedicine and rehabilitationand geriatrics. Dr. Brit<strong>to</strong>nserves as medical direc<strong>to</strong>rfor Bethesda RehabilitationHospital/RehabilitationCare, Red Wing HealthCenter, Brit<strong>to</strong>n Center,and is the interim medicaldirec<strong>to</strong>r for Courage Center.Dr. Brit<strong>to</strong>n currentlyserves on the <strong>Brain</strong> <strong>Injury</strong>Association of <strong>Minnesota</strong>Board of Direc<strong>to</strong>rs.Estate planning provides long-term sustainability for societyBy Ottar SchmitzMy wife and I are expectingour first child, which is veryexciting. We are entering a strangeand foreign new world of changingtables, bassinets, car seats, and astrange clothing article called a“onesie,” which is essentially alarge sock with arms.My wife is enthralled withmany of these accoutrements whileI, true <strong>to</strong> the cliché, have beenthinking primarily about money.How are we going <strong>to</strong> pay for allthese things? Day care costs howmuch?!? Per day?!? If you arelooking for an adrenaline rushakin <strong>to</strong> bungee jumping, check outthe financial cost calcula<strong>to</strong>rs thatgive future predictions for collegetuition.Luckily I am still filled withendless optimism for our futurechild and feel quite confidentin the academic and athleticscholarships that will undoubtedlycome our way. Why wouldn’t ourchild be exceptional in every way?And so forth.Hidden among all of thesenew responsibilities <strong>to</strong> consideris the matter of our estate. Onemust think of such things whenbecoming a parent, right? Mywife and I are modest folks,but nevertheless we want <strong>to</strong>be responsible parents even inthe event of our very untimelypassing.Furthermore, despite all ofour newfound desire <strong>to</strong> provideour new child with every possiblecomfort and opportunity, we alsowant <strong>to</strong> pass along an importantvalue that we share: the suppor<strong>to</strong>f non-profit organizations thateffectively meet our paradigmfor a caring society, a healthyenvironment, and a peacefulworld.So in our estate planning(such as it is), we are directing apercentage of our net worth (suchas it is) <strong>to</strong> several organizationsthat we feel are important <strong>to</strong> usand the long-term sustainability ofour society.Despite the above loftyaspirations, estate planning feelsa bit like mowing the lawn orwashing windows: you knowyou should do it one of thesedays, but it’s not much fun <strong>to</strong>consider doing right this minute,especially since it involves <strong>to</strong>uchysubjects including that of yourown mortality. However, just withmany other chores, it feels betteronce it’s done!Lastly, please consider the<strong>Brain</strong> <strong>Injury</strong> Association of<strong>Minnesota</strong> when doing your estateplanning. We have establishedourselves as one of <strong>Minnesota</strong>’smost effective non-profi<strong>to</strong>rganizations and the services andeducation we provide are having apositive effect on our communityby increasing the quality of lifefor those living with disabilitiesand increasing the awareness andpreventive measures that will helpavoid brain injuries in the future.We are making a difference!Ottar Schmitz is the DevelopmentCoordina<strong>to</strong>r for the <strong>Brain</strong> <strong>Injury</strong>Association of <strong>Minnesota</strong>.