ACC/AHA/SCAI 2005 Guidelines Update
ACC/AHA/SCAI 2005 Guidelines Update
ACC/AHA/SCAI 2005 Guidelines Update
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Learn and Live SM<strong>ACC</strong>/<strong>AHA</strong> Pocket GuidelineBased on the <strong>ACC</strong>/<strong>AHA</strong>/<strong>SCAI</strong> <strong>2005</strong>Guideline <strong>Update</strong>PercutaneousCoronaryInterventionNovember <strong>2005</strong>
Special thanks toEli Lilly and Companysupported thispocket guidelinethrough aneducational grant.Eli Lilly and Companywas not involved in thedevelopment of thispublication and in noway influencedits contents.
PercutaneousCoronaryInterventionNovember <strong>2005</strong>Writing CommitteeSidney C. Smith, Jr, MD, F<strong>ACC</strong>, F<strong>AHA</strong>, ChairTed. E. Feldman, MD, F<strong>ACC</strong>, F<strong>SCAI</strong>John W. Hirshfeld, Jr, MD, F<strong>ACC</strong>, F<strong>SCAI</strong>Alice K. Jacobs, MD, F<strong>ACC</strong>, F<strong>AHA</strong>, F<strong>SCAI</strong>Morton J. Kern, MD, F<strong>ACC</strong>, F<strong>AHA</strong>, F<strong>SCAI</strong>Spencer B. King, III, MD, M<strong>ACC</strong>, F<strong>SCAI</strong>Douglass A. Morrison, MD, PhD, F<strong>ACC</strong>, F<strong>SCAI</strong>William W. O’Neill, MD, F<strong>ACC</strong>, F<strong>SCAI</strong>Hartzell V. Schaff, MD, F<strong>ACC</strong>, F<strong>AHA</strong>Patrick L. Whitlow, MD, F<strong>ACC</strong>, F<strong>AHA</strong>David O. Williams, MD, F<strong>ACC</strong>, F<strong>AHA</strong>, F<strong>SCAI</strong>
I. IntroductionThe American College of Cardiology (<strong>ACC</strong>)/AmericanHeart Association (<strong>AHA</strong>) practice guidelines areintended to assist healthcare providers in clinicaldecision making by describing a range of generallyacceptable approaches for the diagnosis, management,or prevention of specific diseases or conditions.These percutaneous coronary intervention(PCI) guidelines attempt to define practices thatmeet the needs of most patients in most circumstances.The guideline recommendations reflect aconsensus of expert opinion after a thorough reviewof the available, current scientific evidence and areintended to improve patient care. If these guidelinesare used as the basis for regulatory/payer decisions,the ultimate goal is quality of care and serving thepatient’s best interests. The ultimate judgmentregarding care of a particular patient must be madeby the healthcare provider and patient in light ofall of the circumstances presented by that patient.Although initially limited to balloon angioplastyand termed percutaneous transluminal coronaryangioplasty (PTCA), PCI now includes other newtechniques capable of relieving coronary narrowing.Accordingly, in this document, implantation ofintracoronary stents and other catheter-based interventionsfor treating coronary atherosclerosis areconsidered components of PCI. In this context,2
Table 1. Applying Classification of Recommendationsand Level of Evidence in <strong>ACC</strong>/<strong>AHA</strong> FormatSIZE OF TREATMENT EFFECTCLASS ICLASS IIaBenefit >>> RiskProcedure/TreatmentSHOULD be performed/administeredBenefit >> RiskAdditional studies withfocused objectives neededIT IS REASONABLE to performprocedure/administertreatmentESTIMATE OF CERTAINTY (PRECISION) OF TREATMENT EFFECTLEVEL AMultiple (3-5) populationrisk strata evaluated*General consistency ofdirection and magnitudeof effectLEVEL BLimited (2-3) populationrisk strata evaluated*LEVEL CVery limited (1-2)population risk strataevaluated*■ Recommendation thatprocedure or treatmentis useful/effective■ Sufficient evidence frommultiple randomized trialsor meta-analyses■ Recommendation thatprocedure or treatmentis useful/effective■ Limited evidence fromsingle randomized trial ornonrandomized studies■ Recommendation thatprocedure or treatment isuseful/effective■ Only expert opinion, casestudies, or standard-of-care■ Recommendation in favorof treatment or procedurebeing useful/effective■ Some conflicting evidencefrom multiple randomizedtrials or meta-analyses■ Recommendation in favorof treatment or procedurebeing useful/effective■ Some conflictingevidence from singlerandomized trial ornonrandomized studies■ Recommendation in favorof treatment or procedurebeing useful/effective■ Only diverging expertopinion, case studies,or standard-of-careSuggested phrases forwriting recommendationsshouldis recommendedis indicatedis useful/effective/beneficialis reasonablecan be useful/effective/beneficialis probably recommendedor indicated4*Data available from clinical trials or registries about the usefulness/efficacy in different subpopulations,such as gender, age, history of diabetes, history of prior MI, history of heart failure, and prior aspirin use.
▼CLASS IIbBenefit > RiskAdditional studies with broadobjectives needed; additionalregistry data would be helpfulProcedure/Treatment MAYBE CONSIDERED■ Recommendation’susefulness/efficacy lesswell established■ Greater conflictingevidence from multiplerandomized trials ormeta-analyses■ Recommendation’susefulness/efficacy lesswell established■ Greater conflictingevidence from singlerandomized trial ornonrandomized studies■ Recommendation’susefulness/efficacy lesswell established■ Only diverging expertopinion, case studies, orstandard-of-careCLASS IIIRisk > BenefitNo additional studies neededProcedure/Treatment shouldNOT be performed/administeredSINCE IT IS NOT HELP-FUL AND MAY BE HARMFUL■ Recommendation thatprocedure or treatment isnot useful/effective andmay be harmful■ Sufficient evidence frommultiple randomized trialsor meta-analyses■ Recommendation thatprocedure or treatment isnot useful/effective andmay be harmful■ Limited evidence fromsingle randomized trial ornonrandomized studies■ Recommendation thatprocedure or treatment isnot useful/effective andmay be harmful■ Only expert opinion, casestudies, or standard-of-caremay/might be consideredmay/might be reasonableusefulness/effectiveness isunknown/unclear/uncertainor not well establishedis not recommendedis not indicatedshould notis not useful/effective/beneficialmay be harmful5
II. OutcomesOutcomesThe outcomes of PCI are measured in terms ofsuccess and complications and are related to themechanisms of the employed devices, as well asthe clinical and anatomic patient-related factors(Table 2). The committee recommends the use ofsuch standards as the <strong>ACC</strong>-National CardiovascularData Registry ® whenever feasible to accommodatethe common database for the assessment ofoutcomes.A. Definitions of PCI Success1. Angiographic SuccessWith the advent of advanced adjunct technology,including coronary stents, a minimum stenosisdiameter reduction to less than 20% has been theclinical benchmark of an optimal angiographicresult.2. Procedural SuccessAlthough the occurrence of emergency coronaryartery bypass surgery and death are easily identifiedend points, the definition of procedure-relatedmyocardial infarction (MI) has been debated. Thedevelopment of Q waves in addition to a threshold6
value of creatine kinase (CK) elevation has beencommonly used. The clinical significance of cardiacbiomarker elevations in the absence of Q wavesremains a subject of investigation and debate. Anincrease in CK-MB greater than 5 times is associatedwith worsened outcome. Thus, this degree ofincrease in CK-MB without Q waves is consideredby most to qualify as an associated complicationof PCI. Troponin T or I elevation occurs frequentlyafter PCI. Minor elevations do not appear to haveprognostic value, whereas marked (greater than5 times) elevations are associated with worsened1-year outcome (Table 3).Outcomes7
Table 2. Unadjusted In-Hospital Outcome Trends After PCIOutcomesRegistry Years nNHLBI (I) ‡ 1977–1981 3079*NHLBI (II) § 1985–1986 2311*BARI Registry || 1988–1991 1189*Northern New England 1990–1993 13 014 †SCA&I # 1990–1994 4366 †NACI ** 1990–1994 4079*New York State Database 1991–1994 62 670*Northern New England 1994–1995 7248 †NCN 1994–1997 76 904 †Northern New England 1995–1997 14 490 †NHLBI Dynamic Registry ‡‡ 1997–1998 1559*NHLBI Dynamic 1997–1999 857<strong>ACC</strong>-NCDR 1998–2000 100 292NY State Database 1997–2000 22 102B. Acute Outcome:Procedural ComplicationsClass I1. All patients who have signs or symptoms suggestiveof MI during or after PCI and those with complicatedprocedures should have CK-MB and troponin Ior T measured after the procedure. (Level of Evidence: B)Class IIa1. Routine measurement of cardiac biomarkers (CK-MB and/or troponin I or T) in all patients undergoingPCI is reasonable 8 to 12 hours after the procedure.(Level of Evidence: C)8
Clinical In-Hospital EmergencySuccess, % Mortality, % Q-Wave MI, % CABG, %61 1.2 NR 5.878 1.0 4.8 5.8NR 0.7 2.8 4.188.8 1.0 2.4 2.291.5 2.5 NR 3.4NR 1.6 1.6 1.9NR 0.9 NR 3.489.2 1.1 2.1 2.3NR 1.3 NR 1.791.5 1.2 2.0 1.392 1.9 2.8 0.491 0.9 0.8 1.996.5 1.4 0.4 1.9NR 0.68 NR NROutcomesBARI = Bypass Angioplasty RevascularizationInvestigation; CABG = coronary artery bypass graft;MI = myocardial infarction; NACI = New Approachesin Coronary Interventions; NCDR ® = NationalCardiovascular Data Registry; NCN = NationalCardiovascular Network; NHLBI = National Heart,Lung, and Blood Institute; NR = not reported;<strong>SCAI</strong> = Society for Cardiovascular Angiographyand Interventions.* n = patients.† n = procedures.‡ NHLBI (I), emergency CABG was defined asin-hospital CABG.§ NHLBI (II), MI was defined as the presence of atleast 2 of the 3 criteria: clinical symptoms, Q waveson electrocardiogram (Minnesota code), or elevatedcardiac enzyme level (double the normal levelsfor CK or its MB fraction without Q waves).Emergency CABG was defined as in-hospital CABG.|| BARI, MI was defined as the appearance of electrocardiogramchanges (new pathologic Q waves)supported by abnormal CK-MB elevations. Northern New England, A new MI was defined asa clinical event, electrocardiogram changes, anda creatinine phosphokinase (CPK) rise greater than orequal to 2 times normal levels with positive isozymes.Emergency CABG was defined as surgery performedto treat acute closure, unstable angina, or heart failurerequiring intravenous nitroglycerin or ABP, or tamponaderesulting from the intervention.# <strong>SCAI</strong>, A new MI was defined as any significant infarction(greater than 3 times normal) rise in MB fraction.** NACI, MI was defined as a Q-wave MI.†† MI was defined as 2 or more of the following:1) typical chest pain greater than 20 min not relievedby nitroglycerin; 2) serial electrocardiogram recordingsshowing changes from baseline or serially in ST-Tand/or Q waves in at least 2 contiguous leads; or3) serum enzyme elevation of CK-MB greaterthan 5% of total CK (total CK greater than 2 timesnormal; lactic dehydrogenase (LDH) subtype 1greater than LDH subtype 2).9
Table 3. Incidence of Troponin ElevationsAfter PCI in the Published LiteratureStudy No. of Positive(First Author) Patients Marker Percent Positive DefinitionOutcomesHunt 22 Troponin I 0 > 6 ng/mlRavkilde 23 Troponin T 13 > 0.12 ng/mlKarim 25 Troponin T 44 > 0.2 ng/mlLa Vecchia 19 (Stent), Troponin T and 37% cTnI, 21% cTnT; N/A25 (balloon PCI) troponin I 14% cTnI, 0% cTnTJohansen 75 Troponin T 28 > 0.1 ng/mlShyu 59 (Stent), Troponin T 29; 13 > 0.1 ng/ml61 (balloon PCI)Bertichant 105 Troponin I 22 > 0.1 ng/mlGarbarz 109 Troponin I 27 > 0.3 ng/mlFuchs 1129 Troponin I 31 > 0.15 ng/mlCantor 481 Troponin I 48% Overall; > 1.5 ng/ml26% after excludingpositive or unknownpre-PCI cTnIWu 98 Troponin T 26 > 0.1 ng/mlKizer 212 Troponin T 40% Positive before PCI; ≥ 0.1 ng/ml18% of baseline-negativecTnT were positive after PCIRicciardi 286 Troponin I 13.6 > 2.3 ng/mlKini 2873 Troponin I 38.9 > 2 ng/mlcTnI = cardiac troponin I; cTnT = cardiac troponin T; N/A = not applicable; RR = repeat revascularization.10
Prognostic InformationN/AN/AN/AN/AN/ASignificantly higher incidence of elevated cTnT in patients undergoing stenting thanangioplasty alone.No difference in incidence of recurrent angina, MI, cardiac death, or RR after 12 monthsbetween patients positive or negative for cTnI. Stenting not associated with more minormyocardial damage than angioplasty.No association between post-PCI cTnI and adverse ischemic events.cTnT levels greater than 3x normal limit associated with increased risk of major in-hospitalcomplications, but no association with adverse intermediate-term (8 months) clinical outcomes.Significantly higher 90-day rates of MI and the composite of MI or death in patients withpositive cTnI.At a mean of 77 months of follow-up, no increase in risk of major adverse events detected inrelation to post-PCI cTnT elevation.Pre-PCI cTnT elevation was significantly related to event-free survival during 6-year follow-up;in baseline-negative patients, positive cTnT was the only independent predictor of majoradverse events at 1 year; post-PCI elevation of cTnT greater than or equal to 5x normalwas the strongest long-term predictor of major adverse events at 6 years.cTnI elevations greater than 3-fold are predictive of future major adverse cardiac events.Increased incidence of such events is accounted for by the higher rate of early RR andnot by late cardiac events.Neither cTnI peak elevations nor any subgroup predicted mid-term mortality inlow-to-medium risk patients.11Outcomes Special Considerations
C. Lesion Morphology and ClassificationOutcomesThe Committee has revised the previous <strong>ACC</strong>/<strong>AHA</strong>lesion classification system to reflect high-risk(at least 1 type C lesion characteristic) and non–high-risk (no type C lesion characteristic) lesions(Table 4) in accordance with the PCI Clinical DataStandards from the <strong>ACC</strong>-National CardiovascularData Registry ® .Table 4. Lesion Classification SystemDescriptions of a High-Risk Lesion (Type C Lesion)■ Diffuse (length greater than 2 cm)■ Excessive tortuosity of proximal segment■ Extremely angulated segments greater than 90 degrees■ Total occlusions more than 3 months old and/orbridging collaterals*■ Inability to protect major side branches■ Degenerated vein grafts with friable lesions* The high risk with these criteria is for technical failure and increased restenosis,not for acute complications.12
D. WomenCompared with men, women undergoing PCI areolder and have a higher incidence of hypertension,diabetes mellitus, hypercholesterolemia, and comorbiddisease. The hope that stents wouldeliminate the difference in outcomes betweenwomen and men has not been realized. Genderdifferences in mortality have persisted for patientstreated with stents both in the setting of acute MIand in non-acute settings.OutcomesIn general, the risks and benefits of adjunctive pharmacotherapyin women are similar to those in men,although an increased rate of minor bleeding hasbeen reported in women treated with abciximab.When glycoprotein IIb/IIIa platelet receptor antagonistsare used with unfractionated heparin, a lowerdose of the latter should be considered to decreasethe risk of bleeding in women.E. The Elderly PatientWith rare exception (primary PCI for cardiogenicshock in patients greater than 75 years old), aseparate category has not been created in these<strong>Guidelines</strong> for the elderly. However, their higherincidence of comorbidities and risk for bleedingcomplications should be taken into account whenconsidering the need for PCI.13
F. Comparison With Bypass SurgeryOutcomesOverall, 6 trials have been published comparing PCI using stentswith coronary artery bypass grafting (CABG) in single-vesselor multivessel disease. Both revascularization techniquesrelieve angina. In aggregate, these trials have not shown adifference between CABG and PCI in terms of mortality or proceduralMI among the populations studied, which have includedmostly low-risk patients. Stents appear to have narrowed thelate repeat revascularization difference that favored CABG inthe balloon era. Some risk-adjusted registries have shown thesuperiority of surgery for multivessel disease patients, especiallythose with diabetes. Randomized trials, meta-analysis of trials,and epidemiological studies have shown the superiority of drugelutingstents (DES) over bare-metal stents (BMS) in terms ofreducing late repeat revascularization.G. Comparison With MedicineGiven the limited data available from randomized trials comparingmedical therapy with PCI, it seems prudent to considermedical therapy for the initial management of most patientswith Canadian Cardiovascular Society (CCS) classificationclass I and II stable angina (Table 9, pg. 27) and reserve PCIand CABG for those patients with more severe symptoms andischemia. The symptomatic patient who wishes to remainphysically active, regardless of age, will usually require PCIor CABG to remain physically active.14
III. Institutional and Operator CompetencyA. Quality AssuranceClass I1. An institution that performs PCI should establishan ongoing mechanism for valid peer review ofits quality and outcomes. Review should be conductedboth at the level of the entire program andat the level of the individual practitioner. Qualityassessmentreviews should take risk adjustment,statistical power, and national benchmark statisticsinto consideration. Quality-assessment reviewsshould include both tabulation of adverse eventrates for comparison with benchmark values andcase review of complicated procedures and someuncomplicated procedures. (Level of Evidence: C)2. An institution that performs PCI should participatein a recognized PCI data registry for thepurpose of benchmarking its outcomes againstcurrent national norms. (Level of Evidence: C)CompetencyEach institution that performs PCI must establishan ongoing mechanism for valid peer review of itsquality and outcomes. The program should providean opportunity for interventionalists and physicianswho do not perform angioplasty but are knowledgeableabout it to review its overall results on aregular basis. The review process should tabulate15
the results achieved both by individual physicianoperators and by the overall program and comparethem with national benchmark standards withappropriate risk adjustment. Valid quality assessmentrequires that the institution maintain meticulousrecords that include the patient demographicand clinical characteristics necessary to assessappropriateness and to conduct risk adjustment.CompetencyQuality assessment is a complex process thatincludes more than mere tabulation of successand complication rates. Components of quality incoronary interventional procedures include appropriatenessof case selection, quality of procedureexecution, proper response to intraprocedural problems,accurate assessment of procedure outcome,and appropriateness of postprocedure management.It is important that each of these parameters beconsidered when a quality-assessment review isconducted (Table 5).It is recommended that an interventional cardiologyoperator be certified by the American Board ofInternal Medicine in interventional cardiology.Ideally, board certification in interventional cardiologyshould be required for credentialing (Table 6).16
Table 5. Key Componentsof a Quality Assurance ProgramClinical proficiencyEquipmentmaintenanceand management■ General indications/contraindications■ Institutional and individual operatorcomplication rates, mortality, andemergency CABG■ Institutional and operator procedurevolumes■ Training and qualifications ofsupport staff■ Quality of laboratory facilityCompetencyQualityimprovementprocess■ Establishment of an active concurrentdatabase to track clinical and proceduralinformation as well as patient outcomesfor individual operators and the institution.The <strong>ACC</strong>-National Cardiovascular DataRegistry ® or other databases are stronglyrecommended for this purpose.Radiation safety■ Educational program in the diagnosticuse of X-ray■ Patient and operator exposure<strong>ACC</strong> = American College of Cardiology; CABG = coronary artery bypass graft surgery.17
B. Operator and Institutional VolumeClass I1. Elective PCI should be performed by operatorswith acceptable annual volume (at least 75procedures) at high-volume centers (more than400 procedures) with on-site cardiac surgery.(Level of Evidence: B)Competency2. Elective PCI should be performed by operatorsand institutions whose historical and currentrisk-adjusted outcomes statistics are comparableto those reported in contemporary national dataregistries. (Level of Evidence: C)3. Primary PCI for ST-segment elevation MI (STEMI)should be performed by experienced operators whoperform more than 75 elective PCI procedures peryear and, ideally, at least 11 PCI procedures forSTEMI per year. Ideally, these procedures should beperformed in institutions that perform more than400 elective PCIs per year and more than 36 primaryPCIs for STEMI per year. (Level of Evidence B)Class IIa1. It is reasonable that operators with acceptablevolume (at least 75 PCI procedures per year) performPCI at low-volume centers (200 to 400 PCIprocedures per year) with on-site cardiac surgery.(Level of Evidence: B)18
2. It is reasonable that low-volume operators (fewerthan 75 PCI procedures per year) perform PCI athigh-volume centers (more than 400 PCI proceduresper year) with on-site cardiac surgery. Ideally,operators with an annual procedure volume lessthan 75 should only work at institutions with anactivity level of more than 600 procedures per year.Operators who perform fewer than 75 proceduresper year should develop a defined mentoring relationshipwith a highly experienced operator whohas an annual procedural volume of at least 150procedures per year. (Level of Evidence: B)CompetencyClass IIb1. The benefit of primary PCI for STEMI patientseligible for fibrinolysis when performed by an operatorwho performs fewer than 75 procedures peryear (or fewer than 11 PCIs for STEMI per year) isnot well established. (Level of Evidence: C)Class III1. It is not recommended that elective PCI beperformed by low-volume operators (fewer than75 procedures per year) at low-volume centers(200 to 400) with or without on-site cardiac surgery.An institution with a volume of fewer than 200procedures per year, unless in a region that isunderserved because of geography, should carefullyconsider whether it should continue to offerthis service. (Level of Evidence: B)19
Table 6. Considerations for the Assessmentand Maintenance of Proficiency in CoronaryInterventional ProceduresInstitutions■ Quality-assessment monitoring of privileges and risk-stratified outcomes■ Provide support for a quality assurance staff person (e.g., nurse)to monitor complicationsCompetency■ Minimal institutional performance activity of 200 interventions per year,with the ideal minimum of 400 interventions per year■ Interventional program director who has a career experience of more than500 PCI procedures and is board certified by the ABIM in interventional cardiology■ Facility and equipment requirements to provide high-resolution fluoroscopyand digital video processing■ Experienced support staff to respond to emergencies (see Section III-C, Roleof On-Site Cardiac Surgical Backup for discussion)■ Establishment of a mentoring program for operators who perform fewer than 75procedures per year by individuals who perform at least 150 procedures per yearPhysicians■ Procedural volume of 75 per year or more■ Continuation of privileges based on outcome benchmark rates, with considerationof not granting privileges to operators who exceed adjusted case mix benchmarkcomplication rates for a 2-year period■ Ongoing quality assessment comparing results with current benchmarks, with riskstratification of complication rates■ Board certification by ABIM in interventional cardiologyABIM = American Board of Internal Medicine; PCI = percutaneous coronary intervention.20
C. Role of On-Site Cardiac Surgical BackupClass I1. Elective PCI should be performed by operatorswith acceptable annual volume (at least 75 proceduresper year) at high-volume centers (more than400 procedures annually) that provide immediatelyavailable on-site emergency cardiac surgicalservices. (Level of Evidence: B)2. Primary PCI for patients with STEMI should beperformed in facilities with on-site cardiac surgery.(Level of Evidence: B)CompetencyClass IIIElective PCI should not be performed at institutionsthat do not provide on-site cardiac surgery.(Level of Evidence: C)Several centers have reported satisfactory results based on careful case selectionwith well-defined arrangements for immediate transfer to a surgical program. A small,but real fraction of patients undergoing elective PCI will experience a life-threateningcomplication that could be managed with the immediate on-site availability of cardiacsurgical support but cannot be managed effectively by urgent transfer. A study fromthe Medicare database found higher mortality for patients undergoing elective PCI ininstitutions without onsite cardiac surgery. These recommendations may be subject torevision as clinical data and experience increase.The Writing Committee continues to support the recommendationthat elective PCI should not be performed in facilitieswithout on-site cardiac surgery. Mere convenience should notreplace safety and efficacy in establishing an elective PCIprogram without on-site surgery. As with many dynamic areasin interventional cardiology, these recommendations may besubject to revision as clinical data and experience increase.21
D. Primary PCI for STEMI WithoutOn-Site Cardiac SurgeryCompetencyClass IIb1. Primary PCI for patients with STEMI might be consideredin hospitals without on-site cardiac surgery,provided that appropriate planning for program developmenthas been accomplished, including appropriatelyexperienced physician operators (more than75 total PCIs and, ideally, at least 11 primary PCIsper year for STEMI), an experienced catheterizationteam on a 24 hours per day, 7 days per week callschedule, and a well-equipped catheterizationlaboratory with digital imaging equipment, a fullarray of interventional equipment, and intra-aorticballoon pump capability, and provided that thereis a proven plan for rapid transport to a cardiacsurgery operating room in a nearby hospital withappropriate hemodynamic support capability fortransfer. The procedure should be limited to patientswith STEMI or MI with new or presumably new leftbundle-branch block (LBBB) on electrocardiogramand should be performed in a timely fashion (goalof balloon inflation within 90 minutes of presentation)by persons skilled in the procedure (at least75 PCIs per year) and at hospitals that performa minimum of 36 primary PCI procedures per year.(Level of Evidence: B)22
Class III1. Primary PCI should not be performed in hospitalswithout on-site cardiac surgery and without aproven plan for rapid transport to a cardiac surgeryoperating room in a nearby hospital or withoutappropriate hemodynamic support capability fortransfer. (Level of Evidence: C)Competency23
Table 7. Criteria for Performance of Primary PCIat Hospitals Without On-Site Cardiac Surgery■ The operators must be experienced interventionalists who regularly perform elective PCIat a surgical center (at least 75 cases per year). The catheterization laboratory must performa minimum of 36 primary PCI procedures per year.■ The nursing and technical catheterization laboratory staff must be experienced in handlingacutely ill patients and comfortable with interventional equipment. They must haveacquired experience in dedicated interventional laboratories at a surgical center. Theyparticipate in a 24 hours per day, 365 days per year call schedule.Competency■ The catheterization laboratory itself must be well-equipped, with optimal imaging systems,resuscitative equipment, and IABP support, and it must be well-stocked with a broad arrayof interventional equipment.■ The cardiac care unit nurses must be adept in hemodynamic monitoring and IABPmanagement.■ The hospital administration must fully support the program and enable the fulfillmentof the above institutional requirements.■ There must be formalized written protocols in place for immediate and efficient transferof patients to the nearest cardiac surgical facility that are reviewed/tested on a regular(quarterly) basis.■ Primary PCI must be performed routinely as the treatment of choice around the clockfor a large proportion of patients with acute MI, to ensure streamlined care paths andincreased case volumes.■ Case selection for the performance of primary PCI must be rigorous. Criteria for the typesof lesions appropriate for primary PCI and for the selection for transfer for emergentaortocoronary bypass surgery are shown in Table 8.■ There must be an ongoing program of outcomes analysis and formalized periodiccase review.■ Institutions should participate in a 3- to 6-month period of implementation, duringwhich time development of a formalized primary PCI program is instituted that includesestablishment of standards, training of staff, detailed logistic development, and creationof a quality-assessment and error-management system.IABP = intra-aortic balloon pump; MI = myocardial infarction; PCI = percutaneous coronary intervention.Adapted with permission from Wharton TP Jr, McNamara NS, Fedele FA, Jacobs MI, Gladstone AR, Funk EJ.Primary angioplasty for the treatment of acute myocardial infarction: experience at two communityhospitals without cardiac surgery. J Am Coll Cardiol 1999;33:1257-65.24
There are important institutional considerationsin creating an effective program of primary PCIfor STEMI. An institution must commit its catheterizationfacility to be capable of a 24 hours perday, 7 days per week rapid response to a patientpresenting with STEMI. In addition, the institution’scatheterization facility staff must be sufficientlytrained and experienced in the management of theseriously ill patient with STEMI (Table 7) (Table 8).It has been demonstrated that institutions withoutan elective PCI program that care for a largenumber of patients with STEMI can create highqualityPCI for STEMI programs. These programsrequire the 24 hours per day, 7 days per weekavailability of experienced interventionalists andan institutional commitment to invest in thephysical and cognitive resources needed tosupport a high-quality program.Competency25
Table 8. Patient Selection for Primary PCI andEmergency Aortocoronary Bypass at HospitalsWithout On-Site Cardiac SurgeryAvoid intervention in hemodynamically stable patients with:■ Significant (greater than or equal to 60%) stenosis of an unprotectedleft main coronary artery upstream from an acute occlusion in theleft coronary system that might be disrupted by the angioplasty catheterCompetency■ Extremely long or angulated infarct-related lesions with TIMIgrade 3 flow■ Infarct-related lesions with TIMI grade 3 flow in stable patients with3-vessel disease■ Infarct-related lesions of small or secondary vessels■ Hemodynamically significant lesions in other than the infarct arteryTransfer for emergency aortocoronary bypass surgery patients:■ After primary PCI of occluded vessels if high-grade residual left mainor multivessel coronary disease and clinical or hemodynamic instabilityare present, preferably with intra-aortic balloon pump supportPCI = percutaneous coronary intervention; TIMI = Thrombolysis In Myocardial Infarction.Adapted with permission from Wharton TP Jr, McNamara NS, Fedele FA, Jacobs MI,Gladstone AR, Funk EJ. Primary angioplasty for the treatment of acute myocardialinfarction: experience at two community hospitals without cardiac surgery. J Am CollCardiol 1999;33:1257–65.26
IV. Clinical PresentationsTable 9. Grading of Angina Pectoris Accordingto Canadian Cardiovascular Society ClassificationClassDescription of StageIIIIIIIVOrdinary physical activity does not cause … angina, such as walkingor climbing stairs. Angina occurs with strenuous, rapid, or prolonged exertionat work or recreation.Slight limitation of ordinary activity. Angina occurs on walking or climbingstairs rapidly; walking uphill; walking or stair climbing after meals; in cold, inwind, or under emotional stress; or only during the few hours after waking.Angina occurs on walking more than 2 blocks on the level and climbing morethan 1 flight of ordinary stairs at a normal pace and under normal conditions.Marked limitations of ordinary physical activity. Angina occurs on walking1 to 2 blocks on the level and climbing 1 flight of stairs under normal conditionsand at a normal pace.Inability to carry on any physical activity without discomfort—anginalsymptoms may be present at rest.Adapted with permission from Campeau L. Grading of angina pectoris. Circulation 1976;54:522-3.Clinical PresentationsA. Patients With AsymptomaticIschemia or CCS Angina Class I or IIClass IIa1. Percutaneous coronary intervention is reasonablein patients with asymptomatic ischemia or CCSclass I or II angina and with 1 or more significantlesions in 1 or 2 coronary arteries suitable for PCIwith a high likelihood of success and a low risk of27
Clinical PresentationsClass IIbmorbidity and mortality. The vessels to be dilatedmust subtend a moderate to large area of viablemyocardium or be associated with a moderate tosevere degree of ischemia on noninvasive testing.(Level of Evidence: B)2. Percutaneous coronary intervention is reasonablefor patients with asymptomatic ischemia or CCSclass I or II angina, and recurrent stenosis after PCIwith a large area of viable myocardium or high-riskcriteria on noninvasive testing. (Level of Evidence: C)3. Use of PCI is reasonable in patients with asymptomaticischemia or CCS class I or II angina withsignificant left main coronary artery disease (CAD;greater than 50% diameter stenosis) who are candidatesfor revascularization but are not eligible forCABG. (Level of Evidence: B)1. The effectiveness of PCI for patients with asymptomaticischemia or CCS class I or II angina whohave 2- or 3-vessel disease with significant proximalleft anterior descending coronary artery (LAD)CAD who are otherwise eligible for CABG with 1arterial conduit and who have treated diabetes orabnormal left ventricular (LV) function is not wellestablished. (Level of Evidence: B)2. Percutaneous coronary intervention might beconsidered for patients with asymptomatic ischemia28
or CCS class I or II angina with nonproximalLAD CAD that subtends a moderate area of viablemyocardium and demonstrates ischemia onnoninvasive testing. (Level of Evidence: C)Class III1. Percutaneous coronary intervention is not recommendedin patients with asymptomatic ischemia orCCS class I or II angina who do not meet the criteriaas listed under the class II recommendations or whohave 1 or more of the following:a. Only a small area of viable myocardium at risk(Level of Evidence: C)b. No objective evidence of ischemia(Level of Evidence: C)c. Lesions that have a low likelihood of successfuldilatation (Level of Evidence: C)d. Mild symptoms that are unlikely to be dueto myocardial ischemia (Level of Evidence: C)Clinical Presentationse. Factors associated with increased risk ofmorbidity or mortality (Level of Evidence: C)f. Left main disease and eligibility for CABG(Level of Evidence: C)g. Insignificant disease (less than 50% coronarystenosis) (Level of Evidence: C)29
B. Patients With CCS Angina Class IIIClass IIa1. It is reasonable that PCI be performed in patientswith CCS class III angina and single-vessel or multivesselCAD who are undergoing medical therapyand who have 1 or more significant lesions in 1 ormore coronary arteries suitable for PCI with a highlikelihood of success and low risk of morbidity ormortality. (Level of Evidence: B)Clinical Presentations2. It is reasonable that PCI be performed in patientswith CCS class III angina with single-vessel or multivesselCAD who are undergoing medical therapywith focal saphenous vein graft lesions or multiplestenoses who are poor candidates for reoperativesurgery. (Level of Evidence: C)3. Use of PCI is reasonable in patients with CCSclass III angina with significant left main CAD(greater than 50% diameter stenosis) who arecandidates for revascularization but are noteligible for CABG. (Level of Evidence: B)Class IIb1. Percutaneous coronary intervention may beconsidered in patients with CCS class III anginawith single-vessel or multivessel CAD who areundergoing medical therapy and who have 1 ormore lesions to be dilated with a reduced likelihoodof success. (Level of Evidence: B)30
2. Percutaneous coronary intervention may beconsidered in patients with CCS class III anginaand no evidence of ischemia on noninvasive testingor who are undergoing medical therapy andhave 2- or 3-vessel CAD with significant proximalLAD CAD and treated diabetes or abnormal LVfunction. (Level of Evidence: B)Class III1. Percutaneous coronary intervention is notrecommended for patients with CCS class IIIangina with single-vessel or multivessel CAD,no evidence of myocardial injury or ischemiaon objective testing, and no trial of medicaltherapy, or who have 1 of the following:a. Only a small area of myocardium at risk(Level of Evidence: C)b. All lesions or the culprit lesion to be dilatedwith morphology that conveys a low likelihoodof success (Level of Evidence: C)c. A high risk of procedure-related morbidityor mortality (Level of Evidence: C)d. Insignificant disease (less than 50% coronarystenosis) (Level of Evidence: C)e. Significant left main CAD and candidacyfor CABG (Level of Evidence: C)Clinical Presentations31
C. Patients With Unstable Angina/Non-STEMIClass I1. An early invasive PCI strategy is indicatedfor patients with unstable angina (UA)/non-STEMI(NSTEMI) who have no serious comorbidity andwho have coronary lesions amenable to PCI.Patients must have any of the following high-riskfeatures:a. Recurrent ischemia despite intensive antiischemictherapy (Level of Evidence: A)b. Elevated troponin level (Level of Evidence: A)c. New ST-segment depression (Level of Evidence: A)Clinical Presentationsd. heart failure symptoms or new or worseningmitral regurgitation (Level of Evidence: A)e. Depressed LV systolic function (Level of Evidence: A)f. Hemodynamic instability (Level of Evidence: A)g. Sustained ventricular tachycardia(Level of Evidence: A)h. Percutaneous coronary intervention within6 months (Level of Evidence: A)i. Prior CABG (Level of Evidence: A)Class IIa1. It is reasonable that PCI be performed in patientswith UA/NSTEMI and single-vessel or multivesselCAD who are undergoing medical therapy with focal32
Class IIbsaphenous vein graft lesions or multiple stenoseswho are poor candidates for reoperative surgery.(Level of Evidence: C)2. In the absence of high-risk features associatedwith UA/NSTEMI, it is reasonable to perform PCIin patients with amenable lesions and no contraindicationfor PCI with either an early invasiveor early conservative strategy. See full-textguidelines. (Level of Evidence: B)3. Use of PCI is reasonable in patients with UA/NSTEMI with significant left main CAD (greaterthan 50% diameter stenosis) who are candidatesfor revascularization but are not eligible for CABG.(Level of Evidence: B)1. In the absence of high-risk features associatedwith UA/NSTEMI, PCI may be considered in patientswith single-vessel or multivessel CAD who areundergoing medical therapy and who have 1 ormore lesions to be dilated with reduced likelihoodof success. (Level of Evidence: B)2. Percutaneous coronary intervention may be consideredin patients with UA/NSTEMI who are undergoingmedical therapy who have 2- or 3-vesseldisease, significant proximal LAD CAD, and treateddiabetes or abnormal LV function. (Level of Evidence: B)Clinical Presentations33
Class III1. In the absence of high-risk features associatedwith UA/NSTEMI, PCI is not recommended forpatients with UA/NSTEMI with single-vessel ormultivessel CAD and no trial of medical therapy,or who have 1 or more of the following:Clinical Presentationsa. Only a small area of myocardium at risk(Level of Evidence: C)b. All lesions or the culprit lesion to be dilatedwith morphology that conveys a low likelihoodof success (Level of Evidence: C)c. A high risk of procedure-related morbidity ormortality. (Level of Evidence: C)d. Insignificant disease (less than 50% coronarystenosis) (Level of Evidence: C)e. Significant left main CAD and candidacy forCABG (Level of Evidence: B)D. Patients With STEMI1. General and Specific ConsiderationsClass IGeneral Considerations:1. If immediately available, primary PCI should beperformed in patients with STEMI (including trueposterior MI) or MI with new or presumably new34
LBBB who can undergo PCI of the infarct arterywithin 12 hours of symptom onset, if performed ina timely fashion (balloon inflation goal within90 minutes of presentation) by persons skilled inthe procedure (individuals who perform more than75 PCI procedures per year, ideally at least 11 PCIsper year for STEMI). The procedure should be supportedby experienced personnel in an appropriatelaboratory environment (one that performs morethan 200 PCI procedures per year, of which at least36 are primary PCI for STEMI, and that has cardiacsurgery capability). (Level of Evidence: A) Primary PCIshould be performed as quickly as possible, with agoal of a medical contact–to-balloon or door-toballoontime within 90 minutes. (Level of Evidence: B)Specific Considerations:2. Primary PCI should be performed for patients lessthan 75 years old with ST elevation or presumablynew LBBB who develop shock within 36 hours ofMI and are suitable for revascularization that canbe performed within 18 hours of shock, unless furthersupport is futile because of patient’s wishes orcontraindications/unsuitability for further invasivecare. (Level of Evidence: A)Clinical Presentations35
3. Primary PCI should be performed in patients withsevere heart failure and/or pulmonary edema (Killipclass 3) and onset of symptoms within 12 hours. Themedical contact–to-balloon or door-to-balloon timeshould be as short as possible (i.e., goal within 90minutes). (Level of Evidence: B)Clinical PresentationsClass IIa1. Primary PCI is reasonable for selected patients75 years or older with ST elevation or LBBB or whodevelop shock within 36 hours of MI and are suitablefor revascularization that can be performed within18 hours of shock. Patients with good prior functionalstatus who are suitable for revascularization andagree to invasive care may be selected for such aninvasive strategy. (Level of Evidence: B)2. It is reasonable to perform primary PCI forpatients with onset of symptoms within the prior12 to 24 hours and 1 or more of the following:a. Severe heart failure (Level of Evidence: C)b. Hemodynamic or electrical instability(Level of Evidence: C)c. Evidence of persistent ischemia (Level of Evidence: C)36
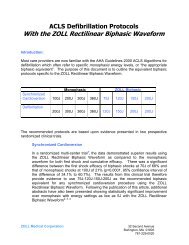
Class IIb1. The benefit of primary PCI for STEMI patientseligible for fibrinolysis when performed by an operatorwho performs fewer than 75 PCI procedures peryear (or fewer than 11 PCIs for STEMI per year)is not well established. (Level of Evidence: C)Class III1. Elective PCI should not be performed in a noninfarct-relatedartery at the time of primary PCIof the infarct-related artery in patients withouthemodynamic compromise. (Level of Evidence: C)2. Primary PCI should not be performed in asymptomaticpatients more than 12 hours after onset ofSTEMI who are hemodynamically and electricallystable. (Level of Evidence: C)Time from symptom onset to reperfusion is animportant predictor of patient outcome. An analysisof the randomized, controlled trials that comparedfibrinolysis with primary PCI suggests that the mortalitybenefit with PCI exists when treatment isdelayed by no more than 60 minutes (Figure 1).Mortality increases significantly with each 15-minutedelay in the time between arrival and restoration ofTIMI-3 flow (door-to-TIMI-3 flow time), whichClinical Presentations37
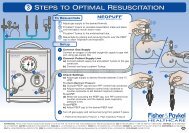
further underscores the importance of timelyreperfusion in patients who undergo primary PCI(Figure 2). Given that the door-to-needle time goalis 30 minutes, this Writing Committee joins theTask Force on the Management of Acute MyocardialInfarction of the European Society of Cardiology andthe <strong>ACC</strong>/<strong>AHA</strong> STEMI <strong>Guidelines</strong> Writing Committeein lowering the door-to-balloon time goal from120 to 90 minutes in an attempt to maximize thebenefits of reperfusion by PCI.Clinical PresentationsAbsolute Risk Difference in Death (%)1050-513 RCTsN=5494P=0.04Figure 1. Percutaneous Coronary InterventionVersus Fibrinolysis with Fibrin-specific Agents:Is Timing (Almost) Everything?30Favors PCIFavors fibrinolysis witha fibrin-specific agent40 50 60 70 80PCI-Related Time Delay (min)38N = number of patients; RCT = randomized controlled trial.Modified with permission from Nallamothu BK, Bates E. Am J Cardiol 2003;92:824-6.
Figure 2. Comparison of Elapsed Timeto Fibrinolysis Versus Primary PCIHospitalsDANAMI-2 (1)FibrinolysisReferralInvasivePrehospitalPrehospitalDoor-Needle = 45 minDoor-to-needleDoor-Needle = 50 minDoor-to-needleTransportationPCIReferralPrehospitalRand-TranspRand-Balloon = 90 min▼Door-toballoonInvasivePrehospitalDoor-to-balloonDoor-Balloon = 93 min0 60 120180 240FibrinolysisPCIPRAGUE-2 (2)Rand-SK▼Pain-Rand Pain-RandSK LysisRand-Transp▼Pain-Rand Pain-RandTranspDoor-to-Balloon▼Clinical PresentationsRand-Balloon = 94 min0 100200300Time is presented as a continuous variable in minutes on the horizontal axis. For DANAMI-2 (second DANishtrial in AMI), times reflect components of delay from symptom onset to randomization (vertical bar) and arefurther separated according to whether patients presented at community referral hospitals or thoseequipped for primary PCI. For those patients randomized to PCI at a referral hospital, the 3 components ofdelay after randomization are related to duration of stay at the referral hospital, time for transport to thePCI hospital, and delay from arrival at the PCI hospital to balloon inflation.PCI = percutaneous coronary intervention; PRAGUE-2 = second study of PRimary Angioplasty after transportof patients from General community hospitals to catheterization Units with/without Emergency thrombolyticinfusion; Rand = randomization; SK = streptokinase; Transp = transportation.Top graph reprinted with permission from Anderson et al. N Engl J Med 2003;349:733-742; (1) Copyright2003 Massachusetts Medical Society. All rights reserved. Bottom graph reprinted from Widimsky et al. EurHeart J 2003;24:94-104 (2) with permission from the European Society of Cardiology.39
Primary stenting using BMS compared with primary PTCA in9 studies showed no differences in mortality (3.0% versus 2.8%)or reinfarction (1.8% versus 2.1%) rates. However, subsequenttarget vessel revascularization rates were lower with stenting.Preliminary reports suggest that compared with conventionalBMS, DES are not associated with increased risk when usedfor primary PCI in patients with STEMI. PCI appears to haveits greatest mortality benefit in high-risk patients. In patientswith cardiogenic shock, an absolute 9% reduction in 30-daymortality with mechanical revascularization instead of immediatemedical stabilization was reported in the SHOCK (SHouldwe emergently revascularize Occluded Coronaries for cardiogenicshocK?) trial.Clinical PresentationsClass I2. Percutaneous Coronary Interventionin Fibrinolytic-Ineligible Patients (Table10)1. Primary PCI should be performed in fibrinolyticineligiblepatients who present with STEMI within12 hours of symptom onset. (Level of Evidence: C)Class IIa1. It is reasonable to perform primary PCI forfibrinolytic-ineligible patients with onset ofsymptoms within the prior 12 to 24 hours and1 or more of the following:a. Severe heart failure (Level of Evidence: C)b. Hemodynamic or electrical instability(Level of Evidence: C)c. Evidence of persistent ischemia (Level of Evidence: C)40
Table 10. Contraindications andCautions for Fibrinolysis in STEMI *Absolute contraindications■ Any prior intracranial hemorrhage■ Known structural cerebral vascular lesion (e.g., arteriovenous malformation)■ Known malignant intracranial neoplasm (primary or metastatic)■ Ischemic stroke within 3 months (except acute ischemic stroke within 3 hours)■ Suspected aortic dissection■ Active bleeding or bleeding diathesis (excluding menses)■ Significant closed head or facial trauma within 3 monthsRelative contraindications■ History of chronic severe, poorly controlled hypertension■ Severe, uncontrolled hypertension on presentation (SBP greater than 180 orDBP greater than 110 mm Hg) †■ History of prior ischemic stroke greater than 3 months, dementia, or known intracranialpathology not covered in contraindications■ Traumatic or prolonged (greater than 10 minutes) CPR or major surgery (less than 3 weeks)■ Recent (within 2 to 4 weeks) internal bleeding■ Noncompressible vascular puncturesClinical Presentations■ For streptokinase/anistreplase: prior exposure (more than 5 days ago) or prior allergicreaction to these agents■ Pregnancy■ Active peptic ulcer■ Current use of anticoagulants: the higher the INR, the higher the risk of bleedingCPR = cardiopulmonary resuscitation; DBP = diastolic blood pressure; INR = international normalized ratio;SBP = systolic blood pressure; STEMI = ST-elevation myocardial infarction..* Viewed as advisory for clinical decision making and may not be all-inclusive or definitive.† Could be an absolute contraindication in low-risk patients with STEMI (see Section 6.3.1.6.3.2in the <strong>ACC</strong>/<strong>AHA</strong> <strong>Guidelines</strong> for the Management of Patients With ST-Elevation Myocardial Infarction,available at: http://www.acc.org/clinical/guidelines/stemi/index.pdf).Reprinted from Antman EM, et al. J Am Coll Cardiol 2004;44:e1-e211.41
3. Percutaneous Coronary InterventionAfter Failed Fibrinolysis (Rescue PCI)Clinical PresentationsClass IClass IIa421. Rescue PCI should be performed in patients lessthan 75 years old with ST elevation or LBBB whodevelop shock within 36 hours of MI and are suitablefor revascularization that can be performedwithin 18 hours of shock, unless further support isfutile because of patient’s wishes or contraindications/unsuitabilityfor further invasive care.(Level of Evidence: B)2. Rescue PCI should be performed in patients withsevere heart failure and/or pulmonary edema (Killipclass 3) and onset of symptoms within 12 hours.(Level of Evidence: B)1. Rescue PCI is reasonable for selected patients75 years or older with ST elevation or LBBB or whodevelop shock within 36 hours of MI and are suitablefor revascularization that can be performedwithin 18 hours of shock. Patients with good priorfunctional status who are suitable for revascularizationand agree to invasive care may be selected forsuch an invasive strategy. (Level of Evidence: B)2. It is reasonable to perform rescue PCI for patientswith 1 or more of the following:a. Hemodynamic or electrical instability(Level of Evidence: C)b. Evidence of persistent ischemia. (Level of Evidence: C)
Class III1. Rescue PCI in the absence of 1 or more of theabove class I or IIa indications is not recommended.(Level of Evidence: C)4. Percutaneous Coronary Intervention AfterSuccessful Fibrinolysis or for Patients NotUndergoing Primary ReperfusionClass I1. In patients whose anatomy is suitable, PCI shouldbe performed when there is objective evidence ofrecurrent MI. (Level of Evidence: C)2. In patients whose anatomy is suitable, PCI shouldbe performed for moderate or severe spontaneousor provocable myocardial ischemia during recoveryfrom STEMI. (Level of Evidence: B)3. In patients whose anatomy is suitable, PCI shouldbe performed for cardiogenic shock or hemodynamicinstability. (Level of Evidence: B)Clinical PresentationsClass IIa1. It is reasonable to perform routine PCI in patientswith LV ejection fraction less than or equal to 0.40,heart failure, or serious ventricular arrhythmias.(Level of Evidence: C)2. It is reasonable to perform PCI when there isdocumented clinical heart failure during the acuteepisode, even though subsequent evaluation showspreserved LV function (LV ejection fraction greaterthan 0.40). (Level of Evidence: C)43
Class IIb1. Percutaneous coronary intervention might beconsidered as part of an invasive strategy afterfibrinolytic therapy. (Level of Evidence: C)5. Percutaneous Coronary Interventionfor Cardiogenic Shock (Figure 3)Clinical PresentationsClass I 1. Primary PCI is recommended for patients lessthan 75 years old with ST elevation or LBBB whodevelop shock within 36 hours of MI and are suitablefor revascularization that can be performedwithin 18 hours of shock, unless further support isfutile because of the patient’s wishes or contraindications/unsuitabilityfor further invasive care. (Levelof Evidence: A)Class IIa 1. Primary PCI is reasonable for selected patients 75years or older with ST elevation or LBBB who developshock within 36 hours of MI and are suitable forrevascularization that can be performed within 18hours of shock. Patients with good prior functionalstatus who are suitable for revascularization andagree to invasive care may be selected for such aninvasive strategy. (Level of Evidence: B)44
▼▼Figure 3. Recommendations for Initial Reperfusion TherapyWhen Cardiogenic Shock Complicates STEMICardiogenic shock▼Early Shock, Diagnosed onHospital Presentation▼Delayed Onset ShockEchocardiogram to rule outmechanical defectsFibrinolytic therapy if all ofthe following are present:1. Greater than 90 minutesto PCI2. Less than 3 hours postSTEMI onset3. No contraindicationsArrange prompt transferto invasive capable centerArrange rapid transferto invasive capable center▼▼▼▼ModerateSevere1-2 vessel CAD Left main CAD3-vessel CAD3-vessel CAD▼▼▼PCI IRA PCI IRA Immediate CABG▼▼IABP▼▼Cardiac Catheterizationand CoronaryAngiographyClinical Presentations▼▼Staged Multivessel PCI▼Staged CABG▼Cannot beperformedEarly mechanical revascularization with PCI/CABG is a class I recommendation for candidates less than75 years of age with ST elevation or LBBB who develop shock less than 36 hours from STEMI and in whomrevascularization can be performed within 18 hours of shock, and it is a class IIa recommendation forpatients 75 years of age or older with the same criteria. Eighty-five percent of shock cases are diagnosedafter initial therapy for STEMI, but most patients develop shock within 24 hours. An intra-aortic balloonpump (IABP) is recommended as a stabilizing measure for patients when shock is not quickly reversed withpharmacological therapy. Dashed lines indicate that the procedure should be performed in patients withspecific indications only. IRA = infarct-related artery; STEMI = ST-elevation myocardial infarction.Reprinted with permission from Hochman. Circulation 2003; 107:2998-3002.45
E. Percutaneous Interventionin Patients With Prior Coronary Bypass SurgeryClass I1. When technically feasible, PCI should be performedin patients with early ischemia (usuallywithin 30 days) after CABG. (Level of Evidence: B)2. It is recommended that distal embolic protectiondevices be used when technically feasible inpatients undergoing PCI to saphenous vein grafts.(Level of Evidence: B)Clinical PresentationsClass IIa461. Percutaneous coronary intervention is reasonablein patients with ischemia that occurs 1 to 3 yearsafter CABG and who have preserved LV functionwith discrete lesions in graft conduits. (Level ofEvidence: B)2. Percutaneous coronary intervention is reasonablein patients with disabling angina secondary to newdisease in a native coronary circulation after CABG.(If angina is not typical, objective evidence ofischemia should be obtained.) (Level of Evidence: B)3. Percutaneous coronary intervention is reasonablein patients with diseased vein grafts more than 3years after CABG. (Level of Evidence: B)4. Percutaneous coronary intervention is reasonablewhen technically feasible in patients with a patentleft internal mammary artery graft who have clinicallysignificant obstructions in other vessels. (Levelof Evidence: C)
Class III1. Percutaneous coronary intervention is not recommendedin patients with prior CABG for chronictotal vein graft occlusions. (Level of Evidence: B)2. Percutaneous coronary intervention is not recommendedin patients who have multiple target lesionswith prior CABG and who have multivessel disease,failure of multiple saphenous vein grafts, andimpaired LV function unless repeat CABG posesexcessive risk due to severe comorbid conditions.(Level of Evidence: B)Class IIaF. Intravascular Ultrasound Imaging1. Intravascular ultrasound is reasonable forthe following:a. Assessment of the adequacy of deployment ofcoronary stents, including the extent of stent appositionand determination of the minimum luminaldiameter within the stent. (Level of Evidence: B)b. Determination of the mechanism of stentrestenosis (inadequate expansion versus neointimalproliferation) and to enable selection of appropriatetherapy (vascular brachytherapy versus repeatballoon expansion). (Level of Evidence: B)c. Evaluation of coronary obstruction at a locationdifficult to image by angiography in a patient with asuspected flow-limiting stenosis. (Level of Evidence: C)47Clinical Presentations
d. Assessment of a suboptimal angiographic resultafter PCI. (Level of Evidence: C)e. Establishment of the presence and distributionof coronary calcium in patients for whomadjunctive rotational atherectomy is contemplated.(Level of Evidence: C)f. Determination of plaque location and circumferentialdistribution for guidance of directionalcoronary atherectomy. (Level of Evidence: B)Class IIb1. Intravascular ultrasound may be considered forthe following:Clinical Presentationsa. Determination of the extent of atherosclerosis inpatients with characteristic anginal symptoms anda positive functional study with no focal stenosesor mild CAD on angiography. (Level of Evidence: C)b. Preinterventional assessment of lesionalcharacteristics and vessel dimensions as a meansto select an optimal revascularization device.(Level of Evidence: C)c. Diagnosis of coronary disease after cardiactransplantation. (Level of Evidence: C)Class III1. Intravascular ultrasound is not recommendedwhen the angiographic diagnosis is clear andno interventional treatment is planned. (Level ofEvidence: C)48
G. Coronary Artery Pressure and Flow:Use of Fractional Flow Reserve and CoronaryVasodilatory ReserveClass IIaClass IIb1. It is reasonable to use intracoronary physiologicalmeasurements (Doppler ultrasound, fractional flowreserve) in the assessment of the effects of intermediatecoronary stenoses (30% to 70% luminalnarrowing) in patients with anginal symptoms.Coronary pressure or Doppler velocimetry may alsobe useful as an alternative to performing noninvasivefunctional testing (e.g., when the functionalstudy is absent or ambiguous) to determine whetheran intervention is warranted. (Level of Evidence: B)1. Intracoronary physiological measurements maybe considered for the evaluation of the success ofPCI in restoring flow reserve and to predict the riskof restenosis. (Level of Evidence: C)2. Intracoronary physiological measurementsmay be considered for the evaluation of patientswith anginal symptoms without an apparent angiographicculprit lesion. (Level of Evidence: C)Clinical PresentationsClass III1. Routine assessment with intracoronary physiologicalmeasurements such as Doppler ultrasoundor fractional flow reserve to assess the severityof angiographic disease in patients with a positive,unequivocal noninvasive functional study is notrecommended. (Level of Evidence: C)49
V. Management of Patients Undergoing PCIA. Oral Antiplatelet TherapyClass I1. Patients already taking daily chronic aspirin therapyshould take 75 to 325 mg of aspirin before thePCI procedure is performed. (Level of Evidence: A)2. Patients not already taking daily chronic aspirintherapy should be given 300 to 325 mg of aspirin atleast 2 hours and preferably 24 hours before the PCIprocedure is performed. (Level of Evidence: C)Patient Management3. After the PCI procedure, in patients with neitheraspirin resistance, allergy, nor increased risk ofbleeding, aspirin 325 mg daily should be given forat least 1 month after BMS implantation, 3 monthsafter sirolimus-eluting stent implantation, and 6months after paclitaxel-eluting stent implantation,after which daily chronic aspirin use should becontinued indefinitely at a dose of 75 to 162 mg.(Level of Evidence: B)4. A loading dose of clopidogrel should be administeredbefore PCI is performed. (Level of Evidence: A) Anoral loading dose of 300 mg, administered at least 6hours before the procedure, has the best establishedevidence of efficacy. (Level of Evidence: B)50
5. In patients who have undergone PCI, clopidogrel75 mg daily should be given for at least 1 monthafter BMS implantation (unless the patient is atincreased risk for bleeding; then it should be givenfor a minimum of 2 weeks), 3 months aftersirolimus stent implantation, and 6 months afterpaclitaxel stent implantation, and ideally up to 12months in patients who are not at high risk ofbleeding. (Level of Evidence: B)Class IIa1. If clopidogrel is given at the time of procedure,supplementation with glycoprotein (GP) IIb/IIIareceptor antagonists can be beneficial to facilitateearlier platelet inhibition than with clopidogrelalone. (Level of Evidence: B)2. For patients with an absolute contraindication toaspirin, it is reasonable to give a 300-mg loadingdose of clopidogrel, administered at least 6 hours,before PCI and/or GP IIb/IIIa antagonists, administeredat the time of PCI. (Level of Evidence: C)3. When a loading dose of clopidogrel is administered,a regimen of greater than 300 mg is reasonableto achieve higher levels of antiplatelet activitymore rapidly, but the efficacy and safety comparedwith a 300-mg loading dose are less established.(Level of Evidence: C)Patient Management51
4. It is reasonable that patients undergoingbrachytherapy be given daily clopidogrel 75 mgindefinitely and daily aspirin 75 to 325 mg indefinitelyunless there is significant risk for bleeding.(Level of Evidence: C)Class IIb1. In patients in whom subacute thrombosismay be catastrophic or lethal (unprotected leftmain, bifurcating left main, or last patent coronaryvessel), platelet aggregation studies may be consideredand the dose of clopidogrel increasedto 150 mg per day if less than 50% inhibition ofplatelet aggregation is demonstrated. (Level ofEvidence: C)Special Considerations Patient Management52Aspirin reduces the frequency of ischemic complicationsafter PCI. A strategy of pretreatment withclopidogrel in patients who have not already hadtheir coronary anatomy defined is controversial,because patients who undergo CABG within 5 to 7days of clopidogrel treatment have an increasedrisk of bleeding.
B. Glycoprotein IIb/IIIa InhibitorsClass I1. In patients with UA/NSTEMI undergoing PCIwithout clopidogrel administration, a GP IIb/IIIainhibitor (abciximab, eptifibatide, or tirofiban)should be administered. (Level of Evidence: A)*Class IIa1. In patients with UA/NSTEMI undergoing PCIwith clopidogrel administration, it is reasonableto administer a GP IIb/IIIa inhibitor (abciximab,eptifibatide, or tirofiban). (Level of Evidence: B)*2. In patients with STEMI undergoing PCI, it isreasonable to administer abciximab as early aspossible. (Level of Evidence: B)3. In patients undergoing elective PCI with stentplacement, it is reasonable to administer a GPIIb/IIIa inhibitor (abciximab, eptifibatide, ortirofiban). (Level of Evidence: B)Class IIb1. In patients with STEMI undergoing PCI, treatmentwith eptifibatide or tirofiban may be considered.(Level of Evidence: C)*It is acceptable to administer the GP IIb/IIIa inhibitor before performance of thediagnostic angiogram (“upstream treatment”) or just before PCI (“in-lab treatment”).Patient Management53
C. Antithrombotic Therapy1. Unfractionated Heparin,Low-Molecular-Weight Heparin, and BivalirudinClass I1. Unfractionated heparin should be administeredto patients undergoing PCI. (Level of Evidence: C)2. For patients with heparin-induced thrombocytopenia,it is recommended that bivalirudinor argatroban be used to replace heparin.(Level of Evidence: B)Class IIa1. It is reasonable to use bivalirudin as an alternativeto unfractionated heparin and GP IIb/IIIaantagonists in low-risk patients undergoing electivePCI. (Level of Evidence: B)2. Low-molecular-weight heparin is a reasonablealternative to unfractionated heparin in patientswith UA/NSTEMI undergoing PCI. (Level of Evidence: B)Patient ManagementClass IIb 1. Low-molecular-weight heparin may beconsidered as an alternative to unfractionatedheparin in patients with STEMI undergoing PCI.(Level of Evidence: B)D. Risk Factor ModificationsAll patients should be instructed about necessary behaviorand risk factor modification, and the appropriate medicaltherapies should be initiated for the secondary prevention54
of atherosclerosis before the patient leaves the hospital.The interventional cardiologist should emphasize the importanceof these measures directly to the patient, becausefailure to do so may suggest that secondary preventiontherapies are not necessary. The interventional cardiologistshould interact with the primary care physician to ensurethat the necessary secondary prevention therapies initiatedduring hospitalization are maintained by patients after dischargefrom the hospital. Secondary prevention measuresare an essential part of long-term therapy because theycan reduce future morbidity and mortality associated withthe atherosclerotic process.E. Left Main CADClass IIa1. It is reasonable that patients undergoing PCIto unprotected left main coronary obstructionsbe followed up with coronary angiography between2 and 6 months after PCI. (Level of Evidence: C)Percutaneous coronary intervention is not recommendedin patients with left main disease who are eligible for CABG.(See Section IV. Clinical Presentations.) In those patientswith significant left main CAD (greater than 50% diameterstenosis) who are not eligible for CABG in whom PCI isperformed, careful postprocedure surveillance, includingcoronary angiography, is needed to prevent fatal MI orsudden death that may be associated with in-stent restenosiswith a large area of myocardium in jeopardy.Patient Management55
VI. Special ConsiderationsA. Management Strategiesfor Restenosis After PTCAClass IIa1. It is reasonable to consider that patientswho develop restenosis after PTCA or PTCAwith atheroablative devices are candidates forrepeat coronary intervention with intracoronarystents if anatomic factors are appropriate.(Level of Evidence: B)B. Drug-Eluting StentsClass I1. A DES should be considered as an alternativeto the BMS in subsets of patients in whom trial datasuggest efficacy. (Level of Evidence: A)Class IIb1. A DES may be considered for use in anatomicsettings in which the usefulness, effectiveness, andsafety have not been fully documented in publishedtrials. (Level of Evidence: C)Special Considerations56
C. Management Strategiesfor In-Stent Restenosis1. Drug-Eluting StentsClass IIa1. It is reasonable to perform repeat PCI forin-stent restenosis with a DES or a new DESfor patients if anatomic factors are appropriate.(Level of Evidence: B)2. RadiationClass IIa1. Brachytherapy can be useful as a safe andeffective treatment for in-stent restenosis.(Level of Evidence: A)D. Subacute Stent ThrombosisIssues of subacute stent thrombosis and technical issueswith the paclitaxel-eluting stent balloon-delivery systemwere early causes for concern. After many more data havebeen accumulated (Table 11), there does not appear to bean increased incidence of early thrombosis with either thesirolimus- or paclitaxel-eluting stent.57Special Considerations
Table 11. Published Randomized Trials and Selected RegistryExperiences of Drug-Eluting Stents Compared with Bare-Metal StentsEluting Number Eluting DrugDrug Trial Year Active /Control Stent DosageSirolimus FIM 2001 30 In Sao Paulo; BxVelocity 140 mcg /cm 215 in RotterdamFIM 2002 15 From BxVelocity 140 mcg /cm 2RotterdamRAVEL 2002 120 /118 BxVelocity 140 mcg /cm 2SIRIUS 2004 533/525 BxVelocity 140 mcg /cm 2C-SIRIUS 2004 50 / 50 BxVelocity 140 mcg /cm 2E-SIRIUS 2003 175 /177 BxVelocity 140 mcg /cm 2RESEARCH 2004 508 / 450 BxVelocity 140 mcg /cm 2Registry OverallRESEARCH 2003 198 /301 BxVelocity 140 mcg /cm 2Registry ACSRESEARCH 2004 186 /183 BxVelocity 140 mcg /cm 2Registry STEMIRESEARCH 2004 56 / 28 BxVelocity 140 mcg /cm 2RegistryChronic TotalsPaclitaxel QuaDS-QP2 2002 15 QuaDS-QP2 2400 to 3200 mcgtotal doseASPECT 2003 59 High dose / Supra-G 3.1 mcg /mm 258 low dose / (high dose);59 control 1.3 mcg /mm 2(low dose)TAXUS I 2003 31/ 30 NIR 1.0 mcg /mm 2TAXUS II 2003 266 / 279 NIR 1.0 mcg /mm 2Special Considerations58TAXUS III 2003 28 In-stent restenosis NIR 1.0 mcg /mm 2TAXUS IV 2004 662 / 652 Express 1.0 mcg /mm 2ACS = acute coronary syndromes; ASPECT = ASian Paclitaxel-Eluting stent Clinical Trial; C-SIRIUS =Canadian SIRIUS trial; E-SIRIUS = European SIRIUS trial; FIM = First In Man; MACE = major adverse cardiacevents; MI = myocardial infarction; NA = not applicable; QuaDS-QP2 = 7-hexanoyltaxol—eluting polymer
Death, Active / MI, Active / Restenosis, Active / TLR, Active /Control, % Control, % Control, % Control, %NA NA 0% at 1 year Minimal neointimalproliferation at 1 yearNA NA 0% at 2 years Minimal neointimalproliferation at 2 years1.7 /1.7 3.3/4.2 0 /26.6 at 6 months 0 / 22.9 at 1 year(P less than 0.001) (P equals 0.001)0.9 / 0.6 2.8 / 3.2 8.9 / 36.3 at 8 months 4.9 / 20 at 1 year(P less than 0.001) (P less than 0.001)0 / 0 2.0 / 4.0 2.3 / 51.1 4.0 / 18.0 at 9 months(P less than 0.001)1.1/ 0.6 4.6/2.3 5.9 / 42.3 4.0 / 20.9 at 9 months(P less than 0.001)1.6 / 2.0 at 30 days 0.8 / 1.6 at 30 days NA 1.0 / 1.8 at 30 days3.0 / 3.0 at 30 days 3.0 / 1.0 at 30 days NA 1.0 / 2.7 at 30 days8.3 / 8.2 at 300 days 0.5 / 2.2 at 300 days NA 1.1/ 8.2 at 300 days(P less than 0.01)0 / 0 In hospital NA NA 12-MonthMACE: 5.6 / 17.2(P less than 0.05)NA NA 13.3 at 6 months; 20 at 6 months;61.5 at 1 year 60 at 1 year0.9 / 0 2.6 / 1.7 4 / 12 / 27 at 4 to 6 months 2 / 2 / 2 at(high dose vs control, 1 to 6 monthsP less than 0.001)0 / 0 0 / 0 0 /10 at 6 months 0 /10 at 1 year(P equals 0.012) (P equals 0.237)0 / 0.8 3.1 / 5.3 7.1/ 21.9 at 6 months 10.4 /21.7 at 12 monthsNA NA NA 21.4 at 1 year1.4 / 1.1 3.5 / 3.7 7.9 / 26.6 at 9 months 4.4 / 15.1 at 1 year(P less than 0.0001) (P less than 0.0001)stent system; RAVEL = RAndomized study with the sirolimus-eluting VELocity balloon expandable stent;RESEARCH = Rapamycin-Eluting Stent Evaluated At Rotterdam Cardiology Hospital; SIRIUS =SIRolImUs-coated stent in de novo native coronary lesions; TLR = target-lesion revascularization.59Special Considerations