


You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
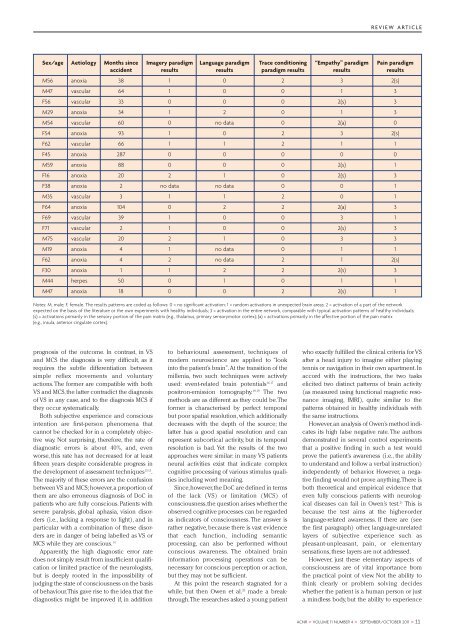
REVIEW ARTICLESex/age Aetiology Months since Imagery paradigm Language paradigm Trace conditioning “Empathy” paradigm Pain paradigmaccident results results paradigm results results resultsM56 anoxia 38 1 0 2 3 2(s)M47 vascular 64 1 0 0 1 3F56 vascular 33 0 0 0 2(s) 3M29 anoxia 34 1 2 0 1 3M54 vascular 60 0 no data 0 2(a) 0F54 anoxia 93 1 0 2 3 2(s)F62 vascular 66 1 1 2 1 1F45 anoxia 287 0 0 0 0 0M59 anoxia 88 0 0 0 2(s) 1F16 anoxia 20 2 1 0 2(s) 3F38 anoxia 2 no data no data 0 0 1M35 vascular 3 1 1 2 0 1F64 anoxia 104 0 2 2 2(a) 3F69 vascular 39 1 0 0 3 1F71 vascular 2 1 0 0 2(s) 3M75 vascular 20 2 1 0 3 3M19 anoxia 4 1 no data 0 1 1F62 anoxia 4 2 no data 2 1 2(s)F30 anoxia 1 1 2 2 2(s) 3M44 herpes 50 0 1 0 1 1M47 anoxia 18 0 0 2 2(s) 1Notes: M, male; F, female. The results patterns are coded as follows: 0 = no significant activation; 1 = random activations in unexpected brain areas; 2 = activation of a part of the networkexpected on the basis of the literature or the own experiments with healthy individuals; 3 = activation in the entire network, comparable with typical activation patterns of healthy individuals;(s) = activations primarily in the sensory portion of the pain matrix (e.g., thalamus, primary sensorymotor cortex); (a) = activations primarily in the affective portion of the pain matrix(e.g., insula, anterior cingulate cortex).prognosis of the outcome. In contrast, in VSand MCS the diagnosis is very difficult, as itrequires the subtle differentiation betweensimple reflex movements and voluntaryactions. The former are compatible with bothVS and MCS, the latter contradict the diagnosisof VS in any case, and to the diagnosis MCS ifthey occur systematically.Both subjective experience and consciousintention are first-person phenomena thatcannot be checked for in a completely objectiveway. Not surprising, therefore, the rate ofdiagnostic errors is about 40%, and, evenworse, this rate has not decreased for at leastfifteen years despite considerable progress inthe development of assessment techniques 13 15 .The majority of these errors are the confusionbetween VS and MCS; however, a proportion ofthem are also erroneous diagnosis of DoC inpatients who are fully conscious. Patients withsevere paralysis, global aphasia, vision disorders(i.e., lacking a response to light), and inparticular with a combination of these disordersare in danger of being labelled as VS orMCS while they are conscious. 14Apparently, the high diagnostic error ratedoes not simply result from insufficient qualificationor limited practice of the neurologists,but is deeply rooted in the impossibility ofjudging the state of consciousness on the basisof behaviour. This gave rise to the idea that thediagnostics might be improved if, in additionto behavioural assessment, techniques ofmodern neuroscience are applied to “lookinto the patient’s brain”. At the transition of themillenia, two such techniques were activelyused: event-related brain potentials 16,17 andpositron-emission tomography. 18,19 The twomethods are as different as they could be. Theformer is characterised by perfect temporalbut poor spatial resolution, which additionallydecreases with the depth of the source; thelatter has a good spatial resolution and canrepresent subcortical activity, but its temporalresolution is bad. Yet the results of the twoapproaches were similar: in many VS patientsneural activities exist that indicate complexcognitive processing of various stimulus qualitiesincluding word meaning.Since, however, the DoC are defined in termsof the lack (VS) or limitation (MCS) ofconsciousness, the question arises whether theobserved cognitive processes can be regardedas indicators of consciousness. The answer israther negative, because there is vast evidencethat each function, including semanticprocessing, can also be performed withoutconscious awareness. The obtained braininformation processing operations can benecessary for conscious perception or action,but they may not be sufficient.At this point the research stagnated for awhile, but then Owen et al. 20 made a breakthrough.The researches asked a young patientwho exactly fulfilled the clinical criteria for VSafter a head injury to imagine either playingtennis or navigation in their own apartment. Inaccord with the instructions, the two taskselicited two distinct patterns of brain activity(as measured using functional magnetic resonanceimaging, fMRI), quite similar to thepatterns obtained in healthy individuals withthe same instructions.However, an analysis of Owen’s method indicatesits high false negative rate. The authorsdemonstrated in several control experimentsthat a positive finding in such a test wouldprove the patient’s awareness (i.e., the abilityto understand and follow a verbal instruction)independently of behavior. However, a negativefinding would not prove anything. There isboth theoretical and empirical evidence thateven fully conscious patients with neurologicaldiseases can fail in Owen’s test. 21 This isbecause the test aims at the higher-orderlanguage-related awareness. If there are (seethe first paragraph) other, language-unrelatedlayers of subjective experience such aspleasant-unpleasant, pain, or elementarysensations, these layers are not addressed.However, just these elementary aspects ofconsciousness are of vital importance fromthe practical point of view. Not the ability tothink clearly or problem solving decideswhether the patient is a human person or justa mindless body, but the ability to experience<strong>ACNR</strong> > VOLUME 11 NUMBER 4 > SEPTEMBER/OCTOBER 2011 > 11














