THE ASSOCIATION OF BRITISH NEUROLOGISTSHeather Angus-Leppan MSc (Ep),MD, FRACP, FRCPwas born in South Africa,trained in Australia and wona Scholarship as VisitingAustralasian Registrar to theRadcliffe Infirmary, Oxford,in 1993. She is ConsultantNeurologist, HonorarySenior Lecturer and EpilepsyLead at the Barnet and RoyalFree Hospitals, London, UK.She is the HonorarySecretary of the Associationof British Neurologists, pastHonorary Secretary of theNeurosciences Section ofthe Royal Society ofMedicine and Chair of theMap of Medicine EpilepsyGroup, UK.Correspondence to:Heather Angus-Leppan,Honorary AssistantSecretary, ABN.Heather.Angus-Leppan@bcf.nhs.ukAcknowledgement:Drs David Bateman,Steve Pollock and theworking party laboured hardon the joint report; withDr Patrick Cadigan andothers at the RCP, withAlastair Compston andCharles Warlow at the ABN.Martin Rossor,Charles Warlow andGeraint Fuller contributedvaluably to the ABNsubmission on directaccess MRI.Avoiding VOMITs andImproving CareBritish neurology is under pressure to meet newdemands in our outpatient and inpatient work.The two are closely linked and the Association ofBritish Neurologists (ABN) is working hard to influencechanges in both areas.Outpatient neurology, open access MRI andreal efficiencyCancer targets have infiltrated all areas of medicine,including neurology. In particular, headache is seen as apotential area of change. The potential ‘solution’ ofdirect access MRI scanning for GPs for all newheadache patients (trialled locally in some areasalready) won’t solve any problems, will create new onesand at the end of it all, won’t get rid of the patient’sheadache. Instead of more scans, the ABN suggestsincreasing partnership with primary care, working toincrease awareness and utilisation of current headachemanagement guidelines such as BASH (The BritishAssociation for the Study of Headache), Map ofMedicine, and other locally produced guidelines.Eliminating cancer as the underlying cause is only avery small part of neurological practice, and canusually be done clinically in the case of headache.Headache makes up a huge chunk of neurology referrals,and, as an isolated symptom, is almost never theconsequence of a brain tumour. With the large numberof patients with migraine and other headaches, manyscans would be requested if direct access was implemented.Given the limited number of MRI scannersavailable, this will compromise the availability of scansin patients for whom the scan will have a greater rolein diagnosis and management.Given that migraine occurs in 5% to 10% of the population(at least), and may resist treatment for over amonth and sometimes much longer, it would be unnecessaryand costly to arrange MRI brain scans oneveryone with chronic migraine. Patients with chronicmigraine rarely require an MRI scan. Furthermore, a scandoes not cure their headache, and up to 6% will have anincidental or false positive finding such as a smallaneurysm. This creates unnecessary and enormousanxiety, as well as potentially leading to more investigationswith added costs and occasional risks, and even tosurgery with very serious risks. This figure does notinclude the findings of VOMITs, UBOs, and withincreasing age, white matter hyperintensities andmicrobleeds. Incidental findings generate a huge needfor specialist referrals to settle anxiety, and explain findings.Indiscriminate MRI scanning would be enormouslyexpensive over and above the cost of the scan itself.Access to scanning is not the most important issuefor patients with headache, and will not solve theirpain. Education and empowerment of GPs to treatmigraine earlier and more could have a significantimpact on improving their care.Making a difference at the coal-faceA joint report from the ABN and Royal College ofPhysicians (RCP) “Local adult neurology services forthe next decade” has just been launched and is availableon the RCP website. It is staggering that the UK isone of the few places in the world where neurologistsare not acutely involved in neurological emergencies.They are common, making up 10% of emergencymedical admissions (and many more with stroke).Services for patients admitted to hospital with an acuteneurological illness are particularly concerningbecause they are rarely provided by neurologists, incontrast to those for stroke and other acute medicalspecialties, which may result in patients not receivingthe best possible care available. Neurology remains ashortage specialty, with appointments mainly to theregional neurosciences centres and an inequality ofmore than three to one in numbers of neurologists indifferent parts of the UK.Neurology services in the UK are organised aroundlarge regional neurosciences centres with anemphasis on research and academic excellence.These are crucial and should not be threatened, or wewill lose the heart of what is needed to maintain excellence.They have produced world class research andnew treatments for patients. But district generalhospital services remain under-resourced because of alack of local neurologists, in contrast to the USA andEurope with more neurologists per head of the population(1:40,000 versus 1:125,000). The lack of localneurologists in the DGH has resulted in poor localservices exacerbated by an increase in outpatientdemand driven by waiting time targets, inadequateresources and sometimes poorly structured servicesnetworked across health providers.Long-term care of neurology patients also requirebig improvements. Patients need a range of neurologyservices at different stages of their illness - acute admission,outpatient care and long-term care. However,these are currently badly integrated, leaving manypatients unable to access the right specialist at theright time and often far from home. They include sucha variety of conditions that more than one model isneeded for good care. For the patient, and their families,they need to be able to move between services,without fights or delays in provisions.To solve these problems, the report recommendsbetter integrated primary, secondary and tertiaryresources to achieve a neurology network that is easilyaccessible, provides local care where appropriate and,as needed, at the regional neurosciences centre. Thereport proposes changes to cover acute neurologyservices, outpatient care, care for patients with longtermneurological conditions, the relationshipbetween local services and the regional centres,commissioning, workforce planning and training.What can we do?We don’t want the new report to grow dusty on theshelf. It is clear that both large and small scale changesare needed to improve acute and long-term care ofneurology patients.Improvements have been, and can be, made at locallevel and we really would like to hear about more ofthese, as models of good care.The neurological charities support our calls forimprovements in services for patients, both acutely andin the long term, and it is clear that central changes areneeded. It is also clear that some of the changes willrequire more money. The resources required for directaccess MRI would be much better spent on implementationof the RCP-ABN report, and we are making thiscrucial point to the Department of Health. l22 > <strong>ACNR</strong> > VOLUME 11 NUMBER 4 > SEPTEMBER/OCTOBER 2011
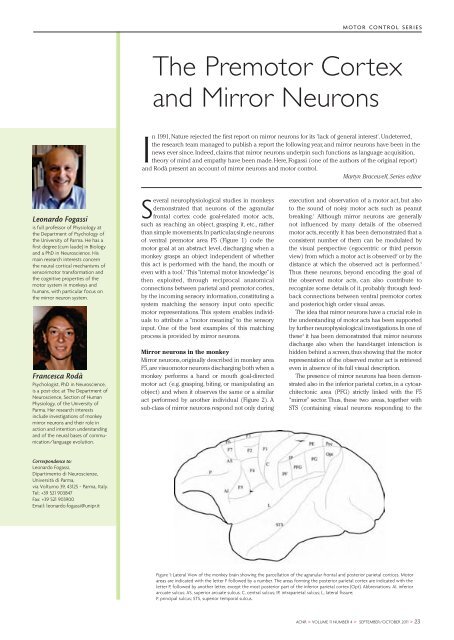
MOTOR CONTROL SERIESThe Premotor Cortexand Mirror NeuronsIn 1991, Nature rejected the first report on mirror neurons for its 'lack of general interest'. Undeterred,the research team managed to publish a report the following year, and mirror neurons have been in thenews ever since. Indeed, claims that mirror neurons underpin such functions as language acquisition,theory of mind and empathy have been made. Here, Fogassi (one of the authors of the original report)and Rodà present an account of mirror neurons and motor control.Martyn Bracewell, Series editorLeonardo Fogassiis full professor of Physiology atthe Department of Psychology ofthe University of Parma. He has afirst degree (cum laude) in Biologyand a PhD in Neuroscience. Hismain research interests concernthe neural cortical mechanisms ofsensorimotor transformation andthe cognitive properties of themotor system in monkeys andhumans, with particular focus onthe mirror neuron system.Francesca RodàPsychologist, PhD in Neuroscience,is a post-doc at The Department ofNeuroscience, Section of HumanPhysiology, of the University ofParma. Her research interestsinclude investigations of monkeymirror neurons and their role inaction and intention understandingand of the neural bases of communication/languageevolution.Several neurophysiological studies in monkeysdemonstrated that neurons of the agranularfrontal cortex code goal-related motor acts,such as reaching an object, grasping it, etc., ratherthan simple movements. In particular, single neuronsof ventral premotor area F5 (Figure 1) code themotor goal at an abstract level, discharging when amonkey grasps an object independent of whetherthis act is performed with the hand, the mouth oreven with a tool. 1 This “internal motor knowledge” isthen exploited, through reciprocal anatomicalconnections between parietal and premotor cortex,by the incoming sensory information, constituting asystem matching the sensory input onto specificmotor representations. This system enables individualsto attribute a “motor meaning” to the sensoryinput. One of the best examples of this matchingprocess is provided by mirror neurons.Mirror neurons in the monkeyMirror neurons, originally described in monkey areaF5, are visuomotor neurons discharging both when amonkey performs a hand or mouth goal-directedmotor act (e.g. grasping, biting, or manipulating anobject) and when it observes the same or a similaract performed by another individual (Figure 2). Asub-class of mirror neurons respond not only duringexecution and observation of a motor act, but alsoto the sound of noisy motor acts such as peanutbreaking. 1 Although mirror neurons are generallynot influenced by many details of the observedmotor acts, recently it has been demonstrated that aconsistent number of them can be modulated bythe visual perspective (egocentric or third personview) from which a motor act is observed 2 or by thedistance at which the observed act is performed. 3Thus these neurons, beyond encoding the goal ofthe observed motor acts, can also contribute torecognize some details of it, probably through feedbackconnections between ventral premotor cortexand posterior, high order visual areas.The idea that mirror neurons have a crucial role inthe understanding of motor acts has been supportedby further neurophysiological investigations. In one ofthese 4 it has been demonstrated that mirror neuronsdischarge also when the hand-target interaction ishidden behind a screen, thus showing that the motorrepresentation of the observed motor act is retrievedeven in absence of its full visual description.The presence of mirror neurons has been demonstratedalso in the inferior parietal cortex, in a cytoarchitectonicarea (PFG) strictly linked with the F5“mirror” sector. Thus, these two areas, together withSTS (containing visual neurons responding to theCorrespondence to:Leonardo Fogassi,Dipartimento di Neuroscienze,Università di Parma,via Volturno 39, 43125 - Parma, Italy.Tel: +39 521 903847Fax: +39 521 903900Email: leonardo.fogassi@unipr.itFigure 1: Lateral View of the monkey brain showing the parcellation of the agranular frontal and posterior parietal cortices. Motorareas are indicated with the letter F followed by a number. The areas forming the posterior parietal cortex are indicated with theletter P, followed by another letter, except the most posterior part of the inferior parietal cortex (Opt). Abbreviations: AI, inferiorarcuate sulcus; AS, superior arcuate sulcus; C, central sulcus; IP, intraparietal sulcus; L, lateral fissure;P, principal sulcus; STS, superior temporal sulcus.<strong>ACNR</strong> > VOLUME 11 NUMBER 4 > SEPTEMBER/OCTOBER 2011 > 23