Supervisor Report of Employee Injury-Illness - University of Arizona
Supervisor Report of Employee Injury-Illness - University of Arizona
Supervisor Report of Employee Injury-Illness - University of Arizona

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
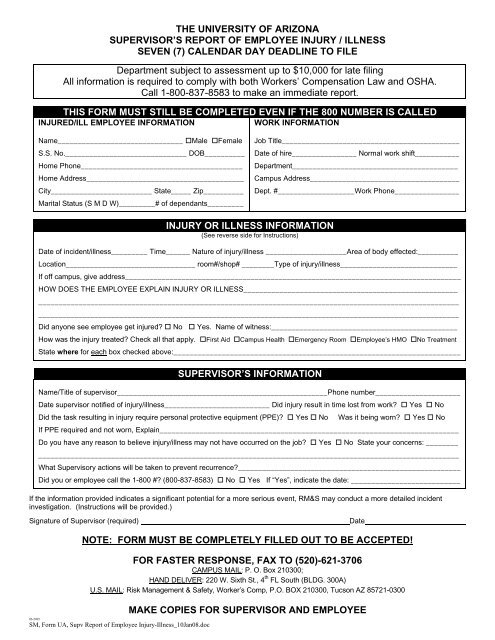
THE UNIVERSITY OF ARIZONASUPERVISOR’S REPORT OF EMPLOYEE INJURY / ILLNESSSEVEN (7) CALENDAR DAY DEADLINE TO FILEDepartment subject to assessment up to $10,000 for late filingAll information is required to comply with both Workers’ Compensation Law and OSHA.Call 1-800-837-8583 to make an immediate report.THIS FORM MUST STILL BE COMPLETED EVEN IF THE 800 NUMBER IS CALLEDINJURED/ILL EMPLOYEE INFORMATIONWORK INFORMATIONName_______________________________ Male FemaleS.S. No.______________________________ DOB__________Home Phone________________________________________Home Address_______________________________________City_________________________ State_____ Zip__________Marital Status (S M D W)_________# <strong>of</strong> dependants_________Job Title____________________________________________Date <strong>of</strong> hire________________ Normal work shift___________Department_________________________________________Campus Address_____________________________________Dept. #___________________Work Phone________________INJURY OR ILLNESS INFORMATION(See reverse side for Instructions)Date <strong>of</strong> incident/illness_________ Time______ Nature <strong>of</strong> injury/illness ____________________Area <strong>of</strong> body effected:__________Location________________________________ room#/shop# ________Type <strong>of</strong> injury/illness_____________________________If <strong>of</strong>f campus, give address___________________________________________________________________________________HOW DOES THE EMPLOYEE EXPLAIN INJURY OR ILLNESS_____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Did anyone see employee get injured? No Yes. Name <strong>of</strong> witness:______________________________________________How was the injury treated? Check all that apply. First Aid Campus Health Emergency Room <strong>Employee</strong>’s HMO No TreatmentState where for each box checked above:_______________________________________________________________________SUPERVISOR’S INFORMATIONName/Title <strong>of</strong> supervisor____________________________________________________Phone number_____________________Date supervisor notified <strong>of</strong> injury/illness__________________________ Did injury result in time lost from work? Yes NoDid the task resulting in injury require personal protective equipment (PPE)? Yes No Was it being worn? Yes NoIf PPE required and not worn, Explain__________________________________________________________________________Do you have any reason to believe injury/illness may not have occurred on the job? Yes No State your concerns: ________________________________________________________________________________________________________________What <strong>Supervisor</strong>y actions will be taken to prevent recurrence?_______________________________________________________Did you or employee call the 1-800 #? (800-837-8583) No Yes If “Yes”, indicate the date: ___________________________If the information provided indicates a significant potential for a more serious event, RM&S may conduct a more detailed incidentinvestigation. (Instructions will be provided.)Signature <strong>of</strong> <strong>Supervisor</strong> (required)DateNOTE: FORM MUST BE COMPLETELY FILLED OUT TO BE ACCEPTED!FOR FASTER RESPONSE, FAX TO (520)-621-3706CAMPUS MAIL: P. O. Box 210300;HAND DELIVER: 220 W. Sixth St., 4 th FL South (BLDG. 300A)U.S. MAIL: Risk Management & Safety, Worker’s Comp, P.O. BOX 210300, Tucson AZ 85721-030006-2005SM, Form UA, Supv <strong>Report</strong> <strong>of</strong> <strong>Employee</strong> <strong>Injury</strong>-<strong>Illness</strong>_10Jan08.docMAKE COPIES FOR SUPERVISOR AND EMPLOYEE
THE UNIVERSITY OF ARIZONASUPERVISOR'S REPORT OF EMPLOYEE INJURY/ILLNESSEMPLOYEE RIGHT: Workers’ compensation is a right <strong>of</strong> all U <strong>of</strong> A employees/student employeesSUPERVISOR MUST FILL OUT THIS REPORT FOR:1) All incidents involving injury or job related illness.2) All incidents that could have resulted in injury or illness.PURPOSE OF REPORT:1) To help prevent similar incidents in the future.2) Support Workers’ Compensation claim for injured/ill employee as applicable.3) OSHA complianceREPORT MUST BE FILED:1) By a supervisor or, in their absence, the acting supervisor.2) Any incident/illness should be reported initially to 1-800-837-8583.3) If the injury or illness required immediate medical treatment, you must report incident/illness to StateRisk Management (<strong>Arizona</strong> Department <strong>of</strong> Administration) 1-800-837-8583 within 24 hours.Fax report to The <strong>University</strong> <strong>of</strong> <strong>Arizona</strong>, Risk Mgmt. & Safety, (520) 621-3706.Mail original by Campus Mail to The <strong>University</strong> <strong>of</strong> <strong>Arizona</strong>, Risk Mgmt. & Safety, P.O. Box 210300Or Hand Deliver to Risk Mgmt. & Safety, 220 W. Sixth Street, 4 th FL South (USA Bldg. 300A)4) All other incidents must be filed in SEVEN CALENDAR DAYS.5) If additional space is needed, please attach separate paperwork.DESCRIPTION BY TYPEBodily ReactionCaught In, Under or BetweenContact w/AnimalsContact w/Electric CurrentContact w/Cold--Atmosphere Contact w/Cold ObjectsContact w/Heat--Atmosphere Contact w/Hot ObjectsContact w/ChemicalsContact w/SubstanceContact w/MachineryContact w/ToolsContact w/ or Exposure to Radiation—Absorption; Ingestion; and/orInhalationFall from ElevationFall from MaterialsFall from ScaffoldFall from VehicleFall in OpeningFall on Same LevelFall on StairsFall onto ObjectsFall onto WalkwayLifting Object – Pulling or Pushing, Wielding or ThrowingMotor Vehicle Accident -- U <strong>of</strong> A, Personal, or Other VehiclePublic Transportation Accident: Aircraft AccidentBus or Boat AccidentStreetcar or Subway AccidentTaxi or Train AccidentOther Transportation AccidentRubbed or Abraded: By Leaning, Kneeling, or SittingBy Vibration <strong>of</strong> ObjectsBy Foreign Matter in EyeBy Repetition <strong>of</strong> Pressure06-2005SM, Form UA, Supv <strong>Report</strong> <strong>of</strong> <strong>Employee</strong> <strong>Injury</strong>-<strong>Illness</strong>_10Jan08.docNATURE OF INJURY--CATEGORIESAmputationBurn (chemical)Burn or Scald (heat)CancerConcussionContagious/InfectiousContusionCrushing/BruiseCut/LacerationDermatitis/RashDislocationElectric ShockFractureFreezingHearing LossHeart AttackHeat StrokeHernia, RuptureInflammationPneumoconiosisPoisoningPuncture/BiteRadiationScratches/AbrasionsSeizureSprains/StrainsStrokeSunburn/SunstrokeMultiple InjuriesOccupational DiseaseOther Injuries