Peacekeeping without Accountability - Yale Law School
Peacekeeping without Accountability - Yale Law School
Peacekeeping without Accountability - Yale Law School
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Peacekeeping</strong><strong>without</strong><strong>Accountability</strong>The United Nations’ Responsibility for theHaitian Cholera EpidemicTransnational DevelopmentClinic, Jerome N. Frank LegalServices Organization<strong>Yale</strong> <strong>Law</strong> <strong>School</strong>Global Health Justice Partnershipof the <strong>Yale</strong> <strong>Law</strong> <strong>School</strong> and the<strong>Yale</strong> <strong>School</strong> of Public HealthandAssociation Haitienne de Droitde L’Environnment.1 section
The Transnational Development Clinic is a legal clinic, part of the Jerome N.Frank Legal Services Organization at the <strong>Yale</strong> <strong>Law</strong> <strong>School</strong>. The clinic works on arange of litigation and non-litigation projects designed to promote communitycenteredinternational development, with an emphasis on global poverty. Theclinic works with community-based clients and client groups and provides themwith legal advice, counseling, and representation in order to promote specificdevelopment projects. The clinic also focuses on development projects that havea meaningful nexus to the U.S., in terms of client populations, litigation oradvocacy forum, or applicable legal or regulatory framework.The Global Health Justice Partnership (GHJP) is a joint program of the <strong>Yale</strong><strong>Law</strong> <strong>School</strong> and the <strong>Yale</strong> <strong>School</strong> of Public Health, designed to promote research,projects, and academic exchanges in the areas of law, global health, and humanrights. The GHJP has undertaken projects related to intellectual property andaccess to medicines, reproductive rights and maternal health, sexual orientationand gender identity, and occupational health. The partnership engages studentsand faculty through a clinic course, a lunch series, symposia, policy dialogues,and other events. The partnership works collaboratively with academics,activists, lawyers, and other practitioners across the globe and welcomes manyof them as visitors for short- and long-term visits at <strong>Yale</strong>.Copyright © 2013,Transnational DevelopmentClinic, Jerome N. Frank LegalServices Organization, <strong>Yale</strong><strong>Law</strong> <strong>School</strong>, Global HealthJustice Partnership of the<strong>Yale</strong> <strong>Law</strong> <strong>School</strong> and the <strong>Yale</strong><strong>School</strong> of Public Health,and Association Haitiennede Droit de L’Environnment.All rights reserved.Printed in the UnitedStates of AmericaReport design byJessica SvendsenCover photograph was takenoutside the MINUSTAH basein Méyè in March of 2013,during the research team’svisit to Haiti.L’Association Haïtienne de Droit de l’Environnement (AHDEN) is a non-profitorganization of Haitian lawyers and jurists with scientific training. Theorganization’s mission is to help underprivileged Haitians living in rural areasfight poverty through the defense and promotion of environmental and humanrights. These rights are in a critical condition in places like Haiti where ruralcommunities have limited access to education and justice.
ContentsIIIAcknowledgementsGlossary6 Executive Summary10 Summary of Recommendations11 Methodology13 chapter IMINUSTAH and the Cholera Outbreak in Haiti22 chapter IIScientific Investigations Identify MINUSTAHTroops as the Source of the Cholera Epidemic33 chapter IIIThe Requirement of a Claims Commission39 chapter IVThe U.N. Has Failed to Respect Its InternationalHuman Rights Obligations47 chapter VThe U.N.’s Actions Violated Principles andStandards of Humanitarian Relief54 chapter VIRemedies and Recommendations62 Endnotes
AcknowledgmentsThis report was written by Rosalyn Chan MD,MPH, Tassity Johnson, Charanya Krishnaswami,Samuel Oliker-Friedland, and Celso PerezCarballo, student members of the TransnationalDevelopment Clinic (a part of the Jerome N. FrankLegal Services Organization) and the Global HealthJustice Partnership of the <strong>Yale</strong> <strong>Law</strong> <strong>School</strong> and the<strong>Yale</strong> <strong>School</strong> of Public Health, in collaboration withAssociation Haitienne de Droit de L’Environnment(AHDEN). The project was supervised by ProfessorMuneer Ahmad, Professor Ali Miller, and SeniorSchell Visiting Human Rights Fellow Troy Elder.Professor James Silk also assisted with supervision.Jane Chong, Hyun Gyo (Claire) Chung, and PaigeWilson, also students in the TransnationalDevelopment Clinic, provided research andlogistical support.The final draft of the report incorporatescomments and feedback from discussions withrepresentatives from: AHDEN, Association desUniversitaires Motivés pour une Haiti de Droits(AUMOHD), Bureau des Avocats Internationaux(BAI), U.S. Centers for Disease Control (CDC),Collectif de Mobilisation Pour Dedommager LesVictimes du Cholera (Kolektif), Direction Nationalede l’Eau Potable et de l’Assainissement (DINEPA),Médecins Sans Frontières (MSF); Partners inHealth (PIH), and the United States Agency forInternational Development (USAID). The authorsalso wish to thank the residents of Méyè, Haiti whowere directly affected by the cholera epidemic forsharing their experiences with the authors duringtheir visit to Méyè.The report has benefited from the close reviewand recommendations of Professor Jean-AndrèVictor of AHDEN and Albert Icksang Ko, MD, MPH,Professor of Epidemiology and Public Health at the<strong>Yale</strong> University <strong>School</strong> of Medicine. The authors aregrateful for their time and engagement.The authors would like to thank <strong>Yale</strong> <strong>Law</strong><strong>School</strong> and the Robina Foundation for theirgenerosity in funding this project.Finally, the authors thank the followingorganizations and individuals for sharing their timeand wisdom with the team: Joseph Amon, Directorof Health and Human Rights at Human RightsWatch; Dyliet Jean Baptiste, Attorney at BAI; Jean-Marie Celidor, Attorney at AHDEN; Paul ChristianNamphy, Coordinator at DINEPA; Karl “Tom”Dannenbaum, Research Scholar in <strong>Law</strong> and RobinaFoundation Human Rights Fellow at <strong>Yale</strong> <strong>Law</strong><strong>School</strong>; Melissa Etheart, MD, MPH, Cholera MedicalSpecialist, CDC; Evel Fanfan, Attorney and Presidentof AUMOHD; Jacceus Joseph, Attorney and Authorof La MINUSTAH et le cholera; Olivia Gayraud, Head ofMission in Port-au-Prince at MSF; Yves-Pierre Louisof Kolektif; Alison Lutz, Haiti Program Coordinatorat PIH; Duncan Mclean, Desk Manager at MSF;Nicole Phillips, Attorney at Institute for Justiceand Democracy in Haiti ; Leslie Roberts, MPH,Clinical Professor of Population and Family Healthat the Columbia University Mailman <strong>School</strong> ofPublic Health; Margaret Satterthwaite, Professor ofClinical <strong>Law</strong> at New York University <strong>School</strong> of <strong>Law</strong>;Scott Sheeran, Director of the LLM in InternationalHuman Rights <strong>Law</strong> and Humanitarian <strong>Law</strong> at theUniversity of Essex; Deborah Sontag, InvestigativeReporter at the New York Times; Chris Ward,Housing and Urban Development Advisor at USAID;and Ron Waldman, MD, MPH, Professor of GlobalHealth in the Department of Global Health atGeorge Washington University. The authors are alsograteful for the assistance of Maureen Furtak andCarroll Lucht for helping coordinate travel to Haiti.While the authors are grateful to all of theindividuals and organizations listed above,the conclusions drawn in this report representthe independent analysis of the TransnationalDevelopment Clinic, the Global Justice HealthPartnership, and AHDEN, based solely on theirresearch and fieldwork in Haiti.Iacknowledgments
Glossary of Acronyms and AbbreviationsCDCCEDAWCERDCRCCRPDCTCDINEPAGeneral ConventionIACHRICESCRICJICRCIDPHAPHRCICCPRLNSPMINUSTAHMSFMSPPNGOPAHOSOFAUDHRU.N.UNCCCenters for Disease ControlConvention on the Elimination of All Forms of Discrimination against WomenInternational Convention on the Elimination of All Forms of Racial DiscriminationConvention on the Rights of the ChildConvention on the Rights of Persons with DisabilitiesCholera Treatment CenterHaitian National Directorate for Water Supply and SanitationConvention on the Privileges and Immunities of the United NationsInter-American Commission on Human RightsInternational Covenant on Economic, Social, and Cultural RightsInternational Court of JusticeInternational Committee of the Red CrossInternally Displaced PersonHumanitarian <strong>Accountability</strong> PartnershipHuman Rights CommissionInternational Convention on Civil and Political RightsHaitian National Public Health LaboratoryU.N. Stabilization Mission in Haiti (Mission des Nations Unies pour la Stabilisationen Haïti)Médecin Sans Frontières (Doctors Without Borders)Haitian Ministry of Health (Ministère de la Santé Publique et de la Population)Non-Governmental OrganizationPan-American Health OrganizationStatus of Forces AgreementUniversal Declaration of Human RightsUnited NationsV. cholerae Vibrio choleraeVCFWHOUnited Nations Compensation Commission in IraqSeptember 11th Victims Compensation FundWorld Health OrganizationIIglossary
Executive SummaryThis report addresses the responsibility of the United Nations (U.N.) for the choleraepidemic in Haiti—one of the largest cholera epidemics in modern history. The reportprovides a comprehensive analysis of the evidence that the U.N. brought cholerato Haiti, relevant international legal and humanitarian standards necessary tounderstand U.N. accountability, and steps that the U.N. and other key national andinternational actors must take to rectify this harm. Despite overwhelming evidencelinking the U.N. Mission for the Stabilization in Haiti (MINUSTAH) 1 to the outbreak, theU.N. has denied responsibility for causing the epidemic. The organization has refusedto adjudicate legal claims from cholera victims or to otherwise remedy the harmsthey have suffered. By causing the epidemic and then refusing to provide redress tothose affected, the U.N. has breached its commitments to the Government of Haiti, itsobligations under international law, and principles of humanitarian relief. Now, nearlyfour years after the epidemic began, the U.N. is leading efforts to eliminate cholera buthas still not taken responsibility for its own actions. As new infections continue tomount, accountability for the U.N.’s failures in Haiti is as important as ever.The Cholera Epidemic in Haiti and U.N.<strong>Accountability</strong>: BackgroundIn October 2010, only months after the countrywas devastated by a massive earthquake, Haiti wasafflicted with another human tragedy: the outbreakof a cholera epidemic, now the largest in the world,which has killed over 8,000 people, sickened morethan 600,000, and promises new infections for adecade or more. Tragically, the cholera outbreak—the first in modern Haitian history—was causedby United Nations peacekeeping troops whoinadvertently carried the disease from Nepal tothe Haitian town of Méyè. In October 2010, theU.N. deployed peacekeeping troops from Nepal tojoin MINUSTAH in Haiti. The U.N. stationed thesetroops at an outpost near Méyè, approximately 40kilometers northeast of Haiti’s capital, Port-au-Prince. The Méyè base was just a few meters froma tributary of the Artibonite River, the largestriver in Haiti and one the country’s main sourcesof water for drinking, cooking, and bathing.Peacekeepers from Nepal, where cholera is endemic,arrived in Haiti shortly after a major outbreakof the disease occurred in their home country.Sanitation infrastructure at their base in Méyèwas haphazardly constructed, and as a result,sewage from the base contaminated the nearbytributary. Less than a month after the arrival ofthe U.N. troops from Nepal, the Haitian Ministry ofPublic Health reported the first cases of cholera justdownstream from the MINUSTAH camp.Cholera spread as Haitians drank contaminatedwater and ate contaminated food; the country’salready weak and over-burdened sanitary systemonly exacerbated transmission of the diseaseamong Haitians. In less than two weeks after theinitial cases were reported, cholera had alreadyspread throughout central Haiti. During the first30 days of the epidemic, nearly 2,000 people died.By early November 2010, health officials recordedover 7,000 cases of infection. By July 2011, cholerawas infecting one new person per minute, and thetotal number of Haitians infected with cholerasurpassed the combined infected population ofthe rest of the world. The epidemic continued toravage the country throughout 2012, worsenedby Hurricane Sandy’s heavy rains and flooding1 executive summary
in October 2012. In the spring of 2013, with thecoming of the rainy season, Haiti has once moresaw a spike in new infections.Haitian and international non-governmentalorganizations have called on the U.N. to acceptresponsibility for causing the outbreak, but to datethe U.N. has refused to do so. In November 2011,Haitian and U.S. human rights organizations fileda complaint with the U.N. on behalf of over 5,000victims of the epidemic, alleging that the U.N.was responsible for the outbreak and demandingreparations for victims. The U.N. did not respondfor over a year, and in February 2013, invoking theConvention on Privileges and Immunities of theUnited Nations, summarily dismissed the victims’claims. Relying on its organizational immunityfrom suit, the U.N. refused to address the merits ofthe complaint or the factual question of how theepidemic started.Summary of the MethodologyResearch, writing, and editing for this report wascarried out by a team of students and professorsfrom the <strong>Yale</strong> <strong>Law</strong> <strong>School</strong> and the <strong>Yale</strong> <strong>School</strong> ofPublic Health. Desk research draws from primaryand secondary sources, including official U.N.documents, international treatises, news accounts,epidemiological studies and investigations, andother scholarly research in international lawand international humanitarian affairs. Over aone year period, student authors also conductedextensive consultations with Haitians affected bythe epidemic, as well as national and internationaljournalists, medical doctors, advocates, governmentofficials, and other legal professionals with firsthandexperience in the epidemic and its aftermath.In March 2013, students and faculty traveled toHaiti to carry out additional investigations. Theyconsulted stakeholders and key informants in boththe Haitian capital of Port-au-Prince and near theMINUSTAH Méyè base where the outbreak started.The <strong>Yale</strong> student and faculty team presentedstakeholders in and outside of Haiti with a draftsummary and outline of the report for review,discussion and comment. The final draft of thereport incorporates comments and feedback fromall of these consultations.Summary of FindingsThis report provides the first comprehensiveanalysis of not only the origins of the choleraoutbreak in Haiti, but also the U.N.’s legal andhumanitarian obligations in light of the outbreakand the steps the U.N. must take to remediate thisongoing humanitarian disaster. This analysis hasconcluded the following:1 The cholera epidemic in Haiti is directly traceableto MINUSTAH peacekeepers and the inadequatewaste infrastructure at their base in Méyè.2 The U.N.’s refusal to establish a claimscommission for the victims of the epidemicviolates its contractual obligation to Haiti underinternational law.3 By introducing cholera into Haiti and denyingany form of remedy to victims of the epidemic,the U.N. has failed to uphold its duties underinternational human rights law.4 The U.N.’s introduction of cholera into Haitiand refusal to accept responsibility for doingso has violated principles of internationalhumanitarian aid.Chapter I examines the legal and political statusof MINUSTAH before and during the epidemic, aswell as the U.N.’s official response to the outbreak.From its establishment in 2004, MINUSTAH hasbeen charged with a broad mandate encompassingpeacekeeping, the re-establishment of the rule oflaw, the protection of human rights, and social andeconomic development. Moreover, following theJanuary 12, 2010 earthquake, MINUSTAH troopsalso assisted in humanitarian recovery effortsin Haiti. After cholera broke out in October 2010,a number of independent studies and clinicalinvestigations pointed to the MINUSTAH basein Méyè as the source of the epidemic. Choleravictims and their advocates have subsequentlycalled on the U.N. for reparations to remedy thesituation and requested meaningful accountabilitymechanisms to review claims, to no avail.Meanwhile, the national and international2 executive summary
esponse to the epidemic has been underfundedand incomplete.In the years following the outbreak, the U.N.has denied responsibility for the epidemic. TheU.N. has repeatedly relied on a 2011 study by a U.N.Independent Panel of Experts, which concludedthat at the time there was no clear scientificconsensus regarding the cause of the epidemic.However, these experts have since revised theirinitial conclusions. In a recent statement, theyunequivocally stated that new scientific evidencedoes point to MINUSTAH troops as the cause of theoutbreak. As Chapter II of this report establishes,epidemiological studies of the outbreak linkingthe outbreak to the MINUSTAH base in Méyèbelie the U.N.’s claims. Four key findings confirmthat MINUSTAH peacekeeping troops introducedcholera into the country. First, doctors observedno active transmission of symptomatic cholera inHaiti prior to the arrival of the MINUSTAH troopsfrom Nepal. Second, the area initially affectedby the epidemic encompassed the location ofthe MINUSTAH base. Third, the troops at theMINUSTAH base were exposed to cholera in Nepal,and their feces contaminated the water supplynear the base. Finally, the outbreak in Haiti istraceable to a single South Asian cholera strainfrom Nepal. No compelling alternative hypothesisof the epidemic’s origins has been proposed.As Chapter III details, in refusing to provide aforum to address the grievances of victims of thecholera epidemic, despite clear scientific evidencetracing the epidemic to the MINUSTAH camp’sinadequate waste infrastructure, the U.N. violatesits obligations under international law. According tothe U.N. Charter and the Convention on Privilegesand Immunities of the U.N., the U.N. is immunefrom suit in most national and internationaljurisdictions. Because of this legal immunity,the U.N. must provide to third parties certainmechanisms for holding it accountable if and whenit engages in wrongdoing during peacekeepingoperations—an obligation the U.N. Secretary-General has publicly recognized. In a series ofreports submitted to the General Assembly in thelate 1990s, the Secretary-General explained thatthe U.N. has an international responsibility for theactivities of U.N. peacekeepers. This responsibilityincludes liability for damage caused by peacekeepersduring the performance of their duties.The U.N. historically has addressed the scopeof its liability in peacekeeping operations throughStatus of Forces Agreements (SOFAs) signed withhost countries. The Haitian government signedsuch an agreement with MINUSTAH in 2004. Inthis SOFA, the U.N. explicitly promises to create astanding commission to review third party claimsof a private law character—meaning claims relatedto torts or contracts—arising from peacekeepingoperations. Despite its obligations under the SOFA,the U.N. has not established a claims commission inHaiti. In fact, the U.N. has promised similar claimscommissions in over 30 SOFAs since 1990. To date,however, the organization has not established asingle commission, leaving countless victims ofpeacekeeper wrongdoing <strong>without</strong> any remedy at law.The U.N.’s refusal to establish a claims commissionnot only violates the terms of its own contractualagreement with Haiti; it also defies the organization’sresponsibilities under international humanrights law. As Chapter IV explains, the U.N.’s foundingdocuments require that the U.N. respect internationallaw, including international human rightslaw, and promote global respect for human rights. Inaddition, the SOFA requires that MINUSTAH observeall local laws, which include Haiti’s obligations toits citizens under international human rights law.International human rights law guarantees accessto clean water and the prevention and treatment ofinfectious disease, forbids arbitrary deprivation oflife, and ensures that when a person’s human rightsare not respected, he or she may seek reparation forthat harm. By failing to prevent MINUSTAH fromintroducing cholera into a major Haitian watersystem and subsequently denying any remedy to thevictims of the epidemic it caused, the U.N. failed torespect its victims’ human rights to water, health,life, and an effective remedy. Furthermore, giventhe U.N.’s role as a leader in the development, promotion,and protection of international human rightslaw, it risks losing its moral ground by refusing tocomply with the very law it demands states andother international actors respect.The U.N.’s role in introducing cholera into Haitiis particularly troubling given the humanitarianrole that MINUSTAH has played in Haiti. AsChapter V explains, through its conduct thatled to the cholera epidemic in Haiti, MINUSTAH3 executive summary
violated widely accepted principles that mostinternational humanitarian aid organizationspledge to follow. These principles have also beenaccepted and promoted by U.N. agencies. First, theU.N. violated the “do no harm” principle, whichrequires, among other general and specific duties,that humanitarian organizations observe minimalstandards of water management, sanitation, andhygiene in order to prevent the spread of disease.Second, by denying victims of the epidemicany remedy for the harms it caused, the U.N.violated the principle of accountability to affectedpopulations. Humanitarian relief standardsemphasize that establishing and recognizingmechanisms for receiving and addressingcomplaints of those negatively affected by reliefwork is a critical responsibility of humanitarianaid organizations. In Haiti, the U.N. has refusedto create a claims commission to receive andadjudicate third party claims. By not only rejectingits responsibility for the epidemic but also refusingto provide a forum in which its victims canmake their claims, the U.N. continues to violateminimum standards of accountability.Necessary Steps toward <strong>Accountability</strong>in HaitiHaving examined the U.N.’s derogation of itsobligations to the victims of the cholera epidemicunder international law, international humanrights law, and international humanitarianstandards, Chapter VI outlines the steps the U.N.and other principal actors in Haiti must take tomeaningfully address the cholera epidemic andensure U.N. compliance with its legal and moralduties. The U.N. will need to accept responsibilityfor its failures in Haiti, apologize to the victimsof the epidemic, vindicate the legal rights of thevictims, end the ongoing epidemic, and takesteps to ensure that it will never again cause suchtragically avoidable harm, in Haiti or elsewhere.The first three proposed courses of action forthe U.N. respond to the concerns raised in ChaptersIII-V: By accepting accountability when it errs,apologizing for its wrongs, and providing a remedyto victims of its wrongdoing, the U.N. will satisfyits obligations under the SOFA, internationalhuman rights law, and the humanitarian ethic ofaccountability. Furthermore, by taking concreteand meaningful steps to end the ongoing epidemicand guaranteeing that it will reform its practicesto ensure that it does not again cause such a publichealth crisis, the U.N. will address the structuralfailures that led to the outbreak and will begin tofulfill its moral duty to repair what it has damaged.To accomplish this, the U.N. must commit tomaking all necessary investments—particularlyin the areas of emergency care and treatmentfor victims of the disease and clean waterinfrastructure—to ensure that the epidemic doesnot claim more lives. In addition to reducing Haiti’svulnerability to future waterborne epidemics,investments in clean water can also help eliminatecholera from the country.Other entities, starting with the Governmentof Haiti and including NGOs, foreign governments(notably the United States, France, and Canada),and other intergovernmental actors, are also key toremediating the cholera epidemic. These actors musthelp provide direct aid to victims, infrastructuralsupport, and adequate funding for the preventionand treatment of cholera. This includes properlyfunding and supporting the recently completedNational Plan for the Elimination of Cholera in Haiti.The Plan is the Haitian Ministry of Health’s (MSPP)comprehensive program for the elimination ofcholera in Haiti and the Dominican Republic over thenext ten years.Finally, prevention of similar harms in thefuture requires that the U.N. commits to reformingthe waste management practices of its peacekeepersand complying with all provisions of the SOFAs itsigns with countries hosting peacekeepers.While the U.N. has played an important role inthe Haitian post-earthquake recovery effort, it hasalso caused great harm. The introduction of choleraby U.N. peacekeepers in Haiti has killed thousandsof people, sickened hundreds of thousandsmore, and placed yet another strain on Haiti’sfragile health infrastructure. The U.N.’s ongoingunwillingness to hold itself accountable to victimsviolates its obligations under international lawand established principles of humanitarian relief.Moreover, in failing to lead by example, the U.N.undercuts its very mission of promoting the rule oflaw, protecting human rights, and assisting in thefurther development of Haiti.4 executive summary
Recommendations Divided by Relevant Actor1. The United Nations and its Organs,Agencies, Departments, and ProgramsOffice of the Secretary-General• Appoint a claims commissioner per therequirements of paragraph 55 of the SOFA.• Ensure, per the requirements of Paragraph51 of the SOFA, that a claims commission isestablished and that its judgments are enforced.• Apologize publicly to the Haitian people for thecholera epidemic.• Coordinate funding for the MSPP Plan.Security Council• Ensure that peacekeepers are accountable fortheir actions in future missions.Department of <strong>Peacekeeping</strong> Operations• Ensure that SOFAs are followed in all missions topromote peacekeeper accountability.• Promulgate procedures consistent with SphereStandards to guide peacekeeping operations andconduct.MINUSTAH• Apologize publicly to the Haitian people for thecholera epidemic.• Ask the Secretary-General to establish a claimscommission.• Abide by compensation decisions as ordered by aclaims commission or any other legal forum• Vacate the Méyè peacekeeper base and allow thecommunity to turn the land into a treatmentcenter or memorial.2. The World Health Organization andthe Pan-American Health Organization• Continue and increase funding of the MSPP plan.• Provide technical expertise and ensureimplementation of the MSPP plan.3. National GovernmentsHaiti• Fund and supply cholera treatment centers forprimary care of cholera victims.• Continue to monitor outbreaks and gatherreliable data on the incidence of cholera.• Appoint a claims commissioner under Paragraph55 of the SOFA.• Demand that the U.N. appoint a claimscommissioner under paragraph 55 of the SOFA.• Effectively implement the MSPP Plan.United States• Fund immediate cholera treatment andprevention via grants to NGOs, the MSPP, andDINEPA.• Fund the MSPP plan, both directly and viaassistance to the U.N with fundraising fromother countries.• Request that the U.N. appoint a claimscommissioner.• Ensure that the CDC continues to support theMSPP Plan.France, Canada, and other NationalGovernments• Fund immediate cholera treatment andprevention, via grants to NGOs, the MSPP, andDINEPA.• Fund the MSPP plan, both directly and viaassistance to the U.N. with fundraising fromother countries.4. Non-Governmental Organizations• Provide supplies and technical expertise forimmediate cholera relief.• Help fundraise for and channel donations towardthe MSPP plan.• Continue to support the Government of Haiti inits public health efforts.5 recommendations
MethodologyThe findings in this report are based on aninvestigation of the origins of the outbreak andU.N. legal accountability conducted over a oneyearperiod. Researchers consulted U.N. treatiesand resolutions, international law treatises,and epidemiological studies of the cholerabacterium causing the epidemic, news accounts,and academic research in international law andinternational humanitarian law. Researchersalso consulted victims of the epidemic, activists,attorneys, journalists, aid workers, medicaldoctors, and government agency officials with firsthandknowledge of the epidemic and its aftermath.Researchers conducted most of theirinvestigation from the United States and wereregularly in contact with experts in Haiti. InMarch 2013, researchers traveled to Haiti to consultstakeholders in both the Haitian capital of Port-au-Prince and in the town closest to the MINUSTAHbase where the cholera epidemic began.While in Haiti, researchers met withrepresentatives from: Association Haitienne deDroit de L’Environnment (AHDEN), Association desUniversitaires Motivés pour une Haiti de Droits(AUMOHD), Bureau des Avocats Internationaux(BAI), U.S. Centers for Disease Control (CDC),Collectif de Mobilisation Pour Dedommager LesVictimes du Cholera (Kolektif), Direction Nationalede l’ l’Eau Potable et de l’Assainissement (DINEPA),Médecins Sans Frontières (MSF), Partners inHealth (PIH), and the United States Agency forInternational Development (USAID). Researchersalso consulted residents of Méyè, Haiti who weredirectly affected by the cholera epidemic and whofiled claims against the U.N. seeking relief.Researchers presented the stakeholderswith a summary and outline of the report forcritical discussion. The final draft of the reportincorporates comments and feedback from theconsultations made during the trip to Haiti, as wellas from the close review of experts in internationallaw and public health.6 methodology
Chapter IMINUSTAH and theCholera Outbreak in Haiti7 section
Chapter IMINUSTAH and the Cholera Outbreak in HaitiSince the early 1990s, the United Nations hasdeployed several peacekeeping and humanitarianmissions to Haiti in response to recurring periodsof political unrest and socio-economic instability.In 2004, following a period of political turmoil,the U.N. Security Council established its currentHaitian mission: the U.N. Stabilization Missionin Haiti, known as MINUSTAH. 2 The SecurityCouncil charged MINUSTAH with a broadmandate encompassing both peacekeeping andhumanitarian operations. On January 12, 2010,a devastating earthquake struck Haiti, killinghundreds of thousands and further jeopardizingthe country’s already fragile infrastructure. Inthe wake of this tragedy, the Security Councilexpanded MINUSTAH’s mandate to respond to theongoing crisis. While MINUSTAH has contributedto Haiti’s stabilization, the mission has also beencriticized for its failures to protect human rights.Between October 19–20, 2010, nine monthsafter the earthquake, health officials confirmedeight cases of cholera in a remote region of centralHaiti. Cholera had not been observed in thecountry in over a century. The disease spread atan alarming rate, rapidly causing severe cases ofdiarrhea, dehydration, and death. Even before the2010 earthquake, Haiti suffered from a history ofpoor water, sanitation, and health infrastructure.While cholera can be easily prevented and treated,the country’s scarce resources and socio-politicalinstability have made the disease difficult tocontrol. As of April 2013, over 650,000 Haitians hadbeen infected by cholera and over 8,100 had died.The disease continues to spread through Haititoday, and the most optimistic estimates suggestit will take at least another decade to eliminate itfrom the country and the island.Independent investigations by scientists andjournalists have traced the source of the epidemicto MINUSTAH peacekeeping troops. An extensivebody of evidence shows that between October8–21, 2010, troops arriving from cholera-affectedareas of Nepal carried the disease into Haiti. Dueto poor sanitation facilities at the base wherethe troops were stationed, waste containingcholera contaminated the Artibonite River, Haiti’slargest river, and spread to the local population.Scientific studies and firsthand accounts leavelittle doubt that MINUSTAH peacekeepers were theinadvertent source of the cholera outbreak.Since the outbreak began, cholera victims andtheir advocates have repeatedly called on the U.N.to remedy past injuries and meaningfully addressthe ongoing crisis. The U.N., however, has refusedto hear these claims and its overall response to thecholera epidemic remains inadequate. The U.N.has denied its role in the epidemic and refusedto address victims’ claims for redress, despite itsobligations to do so under its own agreementswith Haiti and under instruments and principlesof international law. National and internationalactors have proposed plans to treat and eliminatecholera, but the plans lack sufficient funding toeffectively prevent and treat the disease. Haitianhealth and water and sanitation officials andNGOs that have been essential to the provision ofcholera treatment struggle to manage waves ofthe epidemic that spike during each rainy season.Haitians continue to suffer the consequences of thelargest cholera epidemic in the country’s history,while the party responsible for the outbreak—the U.N.—refuses to make a meaningful effort tocontain, control, and eliminate the disease or toremedy the harm already done.A. MINUSTAH Has Had an ExpandingMandate Marked by a Broad<strong>Peacekeeping</strong> Authority <strong>without</strong><strong>Accountability</strong>.The U.N. has had an intermittent peacekeepingpresence in Haiti since the early 1990s. 3 In April2004, following a period of political instability,the Security Council passed Resolution 1542,creating the U.N. Mission for the Stabilization ofHaiti (MINUSTAH). 4 MINUSTAH was establishedas a joint military and civilian mission with amandate to help Haiti address a broad range of8 minustah and the cholera outbreak in haiti
issues, including peace and political stability, there-establishment of the rule of law, the protectionof human rights, and social and economicdevelopment. 5 MINUSTAH’s scope and operationshave expanded since 2004, and the longstandingpresence and activity of the mission have been metwith local criticism.MINUSTAH’s administration and fundinginvolve many players. In Resolution 1542, theSecurity Council supported the establishment ofthe Core Group, comprising representatives of theOrganization of American States, the CaribbeanCommunity and Common Market, internationalfinancial institutions, and other interestedstakeholders. 6 The Core Group’s purpose is tofacilitate the implementation of MINUSTAH’smandate and states enhance the effectiveness ofthe role of the international community in Haiti.Several countries, including Argentina, Brazil,Canada, Chile, France, Peru, and the United States,have assumed lead roles in MINUSTAH’s operationsin Haiti pursuant to Resolution 1542. 7Since its establishment, MINUSTAH has been amultidimensional peacekeeping mission uniquelyaimed at addressing a broad range of concerns. 8Whereas U.N. peacekeeping operations are generallydeployed in support of a peace agreement reachedbetween parties to a conflict, MINUSTAH wasdeployed <strong>without</strong> such an agreement or ongoingconflict. 9 Instead, MINUSTAH was established inresponse to a complicated and sometimes violentpolitical struggle among different factions in Haiti.In 2000, President Jean-Bertrand Aristide was votedinto office during an election contested by politicalopponents and some members of the internationalcommunity. 10 In February 2004, former soldierstraining in the Dominican Republic invaded Haitiand took large areas of the country. PresidentAristide left Haiti on a plane controlled by the U.S.government. The U.S. government claimed thatPresident Aristide left willingly; President Aristideclaimed he was forced onto the plane. BonifaceAlexandre, then President of the Supreme Court,was sworn in as Interim President. 11 Mr. Alexandrerequested assistance from the United Nations instabilizing the country in the aftermath of theinsurrection, a request that eventually led to theestablishment of MINUSTAH. 12The complicated politics of MINUSTAH’sorigins are reflected in the mission’s broadmandate. The terms of MINUSTAH’s missionhave been defined by a series of Security CouncilResolutions establishing and renewing theMINUSTAH mandate. MINUSTAH’s originalmandate, set forth in Security Council Resolution1542, established three main mission goals: toensure a secure and stable environment, to supportthe conditions for democratic governance andinstitutional development, and to support thepromotion and development of human rights. 13In the same resolution, the Security Councilprovided that MINUSTAH “shall cooperate with theTransitional Government [of Haiti] as well as withtheir international partners, in order to facilitatethe provision and coordination of humanitarianassistance.” 14 Subsequent resolutions between 2005and 2009 renewed and provided minor adjustmentsto the original MINUSTAH mandate. 15MINUSTAH’s mission structure and operationsreflect the breadth of its mandate. The original 2004mission plan envisioned three main components:a military force to establish a secure and stableenvironment throughout the country, a civilianaffairs component responsible for overseeing acivilian police force and supporting initiatives tostrengthen local governmental and civil societyinstitutions, and a humanitarian affairs anddevelopment component. 16 The humanitarianaffairs and development office was tasked withcoordinating humanitarian aid among differentnational and international actors. Senior officersof all three components reported to the head ofmission, the U.N. Special Representative of theSecretary-General. 17 Additionally, the mission as awhole received support from the U.N. Secretariat’sDepartment of <strong>Peacekeeping</strong> Operations. 18 While thespecific structure of the different components haschanged since 2004, the basic organization remains. 19On January 12, 2010, a 7.0-magnitudeearthquake struck Haiti, killing over 200,000,destroying much of the capital, and strainingthe country’s already fragile social and politicalorder. 20 In response to the earthquake, the SecurityCouncil passed Resolutions 1908 and 1927, raisingMINUSTAH’s in-country troop levels and adjustingthe MINUSTAH mandate to include assisting9 minustah and the cholera outbreak in haiti
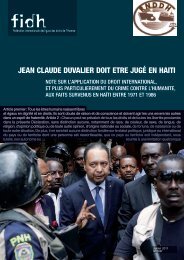
the Government of Haiti in post-disaster reliefand recovery. 21 The Resolutions also reaffirmedMINUSTAH’s obligation to promote and protect thehuman rights of the Haitian people. 22MINUSTAH troops were tasked with key rolesin the immediate response to the earthquake, aswell as the longer-term humanitarian effort. 23Troops assisted in essential humanitarianfunctions including clearing debris, distributingfood, and rebuilding local infrastructure. 24MINUSTAH troops were also responsible formonitoring the human rights situation ofparticularly vulnerable Haitians. For instance,troops led security assessments and policingefforts to ensure the security of those living inspontaneous camps and in areas affected by theearthquake. 25 The mission was further chargedwith building capacity of local institutions toadminister justice and ensure the rule of law. 26Despite MINUSTAH’s role in Haiti’sstabilization, the mission has drawn repeatedcriticism on several fronts. 27 Since the earlydays of the mission, Haitians have denouncedalleged physical abuses by troop members 28 —andMINUSTAH’s seeming unwillingness to investigatethese claims. In November 2007, for instance, over100 Sri Lankan troops were repatriated due toallegations of sexual exploitation and abuse. 29 InSeptember 2011, media outlets released a video ofUruguayan troops harassing an 18-year-old boy,who later claimed that he had been raped by thetroops. 30 In August 2010, 16-year-old Jean GéraldGilles was found hanging outside the MINUSTAHbase in Cap Haitïen. 31 MINUSTAH never initiateda public investigation. 32 These and other similarincidents have led to popular discontent amongHaitians with MINUSTAH’s presence.artibonite riverMirebalais ● MéyèPort-au-Prince ●10 minustah and the cholera outbreak in haiti
The MINUSTAH base (misspelled “MINUSTHA” on Google Earth) in Méyè, on the banks of the Méyè Tributary.Artibonite RiverMéyè TributaryThe town of Mirebalais, located just north of Méyè, where the Méyè Tributary meets the Artibonite River.11 minustah and the cholera outbreak in haiti
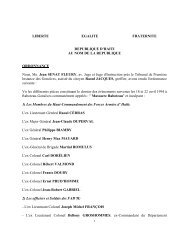
B. The Outbreak of Cholera Has HadDevastating Consequences for theHaitian Population.On October 19, 2010, Haitian health officialsdetected an unusually high number of cases ofacute diarrhea, vomiting, and severe dehydrationin two of Haiti’s ten geographical regions known asadministrative departments. 33 Officials sent stoolsamples for testing to the Haitian National PublicHealth Laboratory (LNSP), and four days later, theLNSP confirmed the presence of Vibrio cholerae(V. cholerae), the bacterium that causes cholera. 34The first set of cases was localized in the upperArtibonite River region, where the Méyè Tributarymeets the Artibonite. By late October 2010, Haitianofficials reported a second set of cases in the lowerArtibonite River region, near the river’s delta. 35 Byearly November, cholera had reached the capital ofPort-au-Prince. 36 Cholera had also spread to citiesacross the North-West and North Departments. 37By November 19, the Haitian Ministry of Health(MSPP) reported positive cholera cases in all tenadministrative departments. 38 By then, over 16,000Haitians had been hospitalized with acute waterydiarrhea and over 900 had died from cholera. 39As Chapter II details, cholera is transmitted bythe consumption of food or water contaminatedwith V. cholerae. 40 The main sources of an outbreakare usually contaminated drinking water andinadequate sanitation; feces from those infectedwith V. cholerae contaminate the water supply,and the bacterium spreads when others drinkthe contaminated water. 41 A gastrointestinaldisease characterized by vomiting, diarrhea, anddehydration, cholera is easily treatable. Withaggressive electrolyte replacement—often simplydelivered in drinking water—fatalities are reducedto less than 1%. 42In Haiti, poor water, sanitation, and healthinfrastructure has facilitated the spread of choleraand prevented its effective treatment. Even beforethe earthquake, the country had an ineffectual andinstitutionally fragmented water and sanitationsector. 43 Approximately 10% of Haitians had accessto running water and only 17% had access toimproved sanitation services. 44 Additionally, untilAugust 2009, the water and sanitation sector hadneither a single national coordination authoritynor sufficient funds. 45 Instead, the sector wasregulated by several governmental institutionsthat were unable to ensure quality water andsanitation services. 46 After a 2009 reform, the waterand sanitation sector still lacked sufficient fundingand was unable to prevent the spread of cholerain the early stages of the epidemic. 47 Meanwhile,the public health sector in Haiti has been unableto treat cholera effectively. The health system inHaiti is supervised and coordinated by a singleentity, the MSPP. 48 Due to financial constraints andthe lack of local capacity to coordinate health careservices, the MSPP has been unable to guaranteeadequate cholera treatment for all Haitians.The Haitian cholera epidemic is one of theworld’s largest national cholera epidemics inrecent history. 49 In 2010 and 2011, Haitiansaccounted for roughly half of cholera cases anddeaths reported to the World Health Organization(WHO). 50 In the first year of the epidemic, over470,000 Haitians were infected and over 6,600 diedof cholera. 51 By October 2012, over 600,000 Haitianshad been infected and over 7,400 had died fromcholera. 52 As of April 2013, the MSPP has reportedover 650,000 infections, and over 8,100 deaths. 53Due to unreported cases in remote areas, thesenumbers likely underestimate the actual harmcaused by the cholera epidemic in Haiti. 54Although more than two years have passedsince the outbreak began, cholera still poses anongoing threat to people in Haiti. 55 The diseasecontinues to contaminate Haiti’s drinking watersources. As rivers overflow with each rainy season,inadequate sewage systems allow for continuedcross-contamination between infected feces anddrinking water sources, perpetuating the cycle ofdisease. Additionally, treatment programs remaininadequate due to a shortage of funding. 56 Expertsexpect Haiti will suffer from cholera for at least adecade more. 57C. Independent Investigations HaveTraced the Source of the Epidemic toMINUSTAH <strong>Peacekeeping</strong> Troops.As Chapter II discusses, nearly every majorinvestigation of the cholera crisis has identified12 minustah and the cholera outbreak in haiti
Top:The MINUSTAH base in Méyè.Below:MINUSTAH peacekeepersentering the base.U.N. peacekeeping troops from Nepal as thesource of the outbreak. 58 Outbreak investigations,environmental surveys, molecular epidemiologicalstudies, and journalistic accounts all demonstratethat the troops were exposed to cholera in Nepaland introduced V. cholerae bacterium into Haiti.These investigations highlight five key factsabout the epidemic. First, there was no activetransmission of cholera in Haiti prior to October2010. Second, the epidemic began at a single pointin an area that encompassed the MINUSTAHbase where Nepalese peacekeeping troops werestationed. Third, these troops had been exposedto cholera in Nepal, and fourth, their fecescontaminated the local water supply in Haiti.Finally, the Haitian outbreak involved a singlestrain of Nepalese origin.Historical records show no reported cases ofsymptomatic cholera in Haiti before the arrivalof MINUSTAH troops in October 2010. 59 Expertshave identified three major cholera outbreaks inthe Caribbean: in 1833–1834, 1850–1856, and 1865-13 minustah and the cholera outbreak in haiti
1872. 60 None of these three outbreaks affected Haiti,even though cholera cases were reported in theneighboring Dominican Republic in 1867. 61 As earlyas 1850, Haitian historians commented on thestriking absence of cholera cases in the country.Additionally, no symptomatic cases of cholera werereported in the Caribbean during the 20th century. 62The 2010 Haitian outbreak began in a regionencompassing the MINUSTAH base in Méyè,a small town in the Artibonite administrativedepartment of central Haiti. Following the firststool samples from patients in this area sent fortesting on October 19 and 20, 2010, 63 the LNSPconfirmed the presence of V. cholerae on October22. 64 Initial cases of cholera were clustered in anarea surrounding the MINUSTAH base. The base issituated on the Méyè Tributary, which flows pastthe town of Mirebalais and into the ArtiboniteRiver. The initial cases of confirmed choleraoccurred downstream from the base. 65Nepalese troops stationed at the Méyè basehad been recently exposed to cholera in Nepal, andtheir feces contaminated the drinking water oflocal Haitians. As part of MINUSTAH’s 2010 troopincrease, a battalion of Nepalese soldiers arrivedin Haiti between October 8–24, 2010. 66 The soldierscame from regions of Nepal recently afflicted byoutbreaks of cholera. 67 The MINUSTAH base hadpoor sanitation conditions. The camp’s wasteinfrastructure was haphazardly constructed,allowing for waste from the camp’s drainage canaland an open drainage ditch to flow directly intothe nearby Méyè Tributary. 68 The drainage siteswere also susceptible to flooding and overflow intothe tributary during rainfall. 69 Direct evidencethat sewage from the base contaminated theMéyè Tributary of the Artibonite River exists. 70 OnOctober 27, journalists caught MINUSTAH troopson tape trying to contain what appeared to be asewage spill at the MINUSTAH base. Families inthe area also confirmed that waste from the campfrequently flowed into the river. 71 Most of the initialcholera patients reported drinking water from theArtibonite River.The close relationship between the Haitiancholera strain and the Nepalese strain furthersupports the conclusion that Nepalese troopsbrought cholera into Haiti. 72 Although there hasbeen no medical documentation of the MINUSTAHtroops carrying cholera, researchers have identifieda common strain of V. cholerae causing cholera inHaiti. 73 Experts have compared this strain with anumber of known cholera strains from around theworld. 74 Genetic evidence shows that the Haitianstrain is descended from a V. cholerae strain ofNepalese origin. In other words, the cholera thatcaused Haiti’s epidemic originated in Nepal. 75D. National and International EffortsHave Been Unsuccessful inEliminating Cholera.A combination of Haitian national agencies,multilateral agencies, other countries, andinternational NGOs have responded to thecholera outbreak. Unfortunately for Haitians, thispatchwork of services, training, and surveillancehas proven inadequate. Much of the choleraresponse effort is not adequately funded andineffective for either the short or longterm.1. Short-term ResponseIn the immediate aftermath of the earthquake,national, international, and NGOs anticipatedthat the massive damage done to Haiti’s fragileinfrastructure would render the countryvulnerable to disease and began to prepareaccordingly. None of these organizations, however,expected an outbreak of cholera, given the disease’slong absence from the country. As a result, localhealth workers had little more than basic trainingon cholera treatment. National health staff had anexisting knowledge of cholera, how it was spread,its treatment, and proper modes of prevention,but few were trained in handling an emergencyoutbreak of the disease.Because of this, during the first phase ofthe epidemic, an international NGO, MédecinSans Frontières (MSF), was the lead provider oftreatment. International humanitarian NGOslike MSF have provided medical services in Haitithroughout the cholera crisis. MSF establishedsome of the first cholera treatment programs,rapidly expanding services in the months of thespiraling outbreak by deploying health workers tothe country and opening cholera treatment centers14 minustah and the cholera outbreak in haiti
(CTCs). By November 2010, just a month after thefirst cases of cholera appeared in Haiti, MSF hadset up 20 CTCs; by early December, 20 more CTCshad been built. CTCs providing oral rehydrationsolution, the primary course of treatment forcholera, were also created in all of the regionsaffected by the disease. MSF set aside some 3,300beds in its facilities for cholera treatment, and bymid-December 2010, the organization had providedcare for more than 62,000 people. 76 MSF’s abilityto provide cholera treatment, however, was soonoverwhelmed by the volume of cholera cases as theoutbreak proved worse than originally anticipated.The treatment plan in the immediateaftermath of the outbreak focused on preventionof cholera infection and death. Local healthauthorities disseminated prevention informationto inhabitants of the rural areas near Mirebalaisand the Artibonite Delta where the first casesappeared. The prevention materials advised boilingor chlorinating drinking water and buryinghuman waste in the hope of stemming the spreadof cholera and avoiding further contaminationof water sources. Due to the rapid spread of thedisease and the high initial case fatality rate, MSPPand the U.S. government focused on five immediatepriorities: preventing deaths in treatment facilitiesby distributing supplies and providing training;preventing deaths in communities by supplyingoral rehydration solution sachets to homes andurging sick individuals to seek immediate care;preventing disease spread by promoting properhygiene and sewage disposal; conducting fieldinvestigations and guiding prevention strategies;and establishing a national cholera surveillancesystem to monitor the spread of the disease. 77Some training of field workers by internationaland bilateral organizations, including the U.S.Centers for Disease Control (CDC), contributed tothe treatment of effected populations during thefirst months of the epidemic. However, neitherthe MSPP nor international NGOs were able tocompletely contain the outbreak.outbreak. The mere task of providing treatmentsupplies has proven daunting as people in Haiticontinue to contract cholera. Difficulties inproviding treatment at the onset of the epidemicwere exacerbated by the fact that only one actor—the Program on Essential Medicine and Supplies,overseen by MSPP and the Pan-American HealthOrganization (PAHO)—distributed all donatedhealth care materials.Several medical organizations continue toprovide prevention and treatment for cholera inpartnership with the MSPP, but the initial fundingfor such work is nearly exhausted. Many aid groupshave already withdrawn from the country due toa lack of funding, and emergency cholera fundingfrom the CDC and World Bank is expected todecrease next year. 78In November 2012, the U.N. announced a $2.27billion initiative to eliminate cholera in Haiti andthe Dominican Republic in the next ten years. 79 Ajoint initiative among the WHO, PAHO, the CDC,and MSPP, the plan is comprehensive; it addresseswater and sanitation, waste disposal, integration ofcholera diagnosis and treatment into basic medicalscreening practices, and provision of choleravaccinations to high-risk groups. However, theU.N. has yet to secure all but a small fraction of thefunding necessary to complete the project fromU.N. member states. 80 To date, the U.N. has onlycommitted to supplying $23.5 million, less than 1%of the necessary funding.Both the short-term and long-term plans forresponding to cholera in Haiti have been criticizedas unrealistically optimistic. International NGOslike MSF struggle to provide quality care as theirbasic treatment supplies dwindle. The mortalityrate in some CTCs has recently risen to analarming 4% as a result of diminishing supplies. 81Although the plan to eliminate cholera in Haitimay be well-conceived in the abstract, it is of littlepractical value <strong>without</strong> proper funding.2. Long-term ResponseThe long-term effort to treat cholera and eliminatethe disease from Haiti has been less effectivethan the short-term response following the initial15 minustah and the cholera outbreak in haiti
E. The United Nations Has Failed toProvide Redress for Victims of theEpidemic.Cholera victims and their advocates have calledon the U.N. to redress the injuries of those harmedby the disease and take responsibility for theongoing epidemic. A number of efforts to hold theU.N. accountable have been underway since theoutbreak began, although to date they have notbeen successfulFirst, Haitian human rights organizations,activists, and lawyers have called for the U.N.to assume responsibility for its actions underthe Status of Forces Agreement (SOFA) it signedwith the Government of Haiti in July of 2004. 82The SOFA defines the relationship between theU.N., including its agents in MINUSTAH, and theGovernment of Haiti. It also lays out the terms ofthe MINUSTAH mission, providing peacekeepingtroops and U.N. personnel legal immunity fromsuit in national and international courts. Inexchange, the SOFA provides for the establishmentof a commission to hear claims from third partiesinjured as a result of MINUSTAH operations.Despite this, no such claims commission has beenestablished for victims of the cholera epidemic. 83In a letter to the Haitian Senate dated March 25,2013, lawyers on behalf of Haitian victims calledon the Government of Haiti to assert its right to aclaims commission under the SOFA. 84 In responseto the inaction of the U.N. and the Governmentof Haiti, these attorneys are also considering asuit to compel the Government of Haiti to initiatethe establishment of a claims commission byappointing a commissioner. 85A second effort to hold the U.N. accountablefor the epidemic was attempted through an appealto the Inter-American Commission on HumanRights (IACHR). In October 2011, a team of Brazilianlawyers acting on behalf of Haitian choleravictims filed a case against the U.N. at the IACHR. 86Petitioners claimed that the U.N.’s actions in Haitiviolated a number of rights under the AmericanConvention on Human Rights. Petitioners arguedthat the IACHR could receive the complaintbecause the U.N. was an organization actingwithin a territory under the IACHR’s jurisdiction. 87To date, the IACHR has not provided an officialresponse to this petition. 88A third legal process began in November 2011,when Haitians infected by cholera and familymembers of those who had died of the diseasesubmitted a petition for relief to the MINUSTAHclaims unit in Haiti and U.N. headquarters inNew York. 89 Petitioners alleged that MINUSTAHnegligently maintained its waste managementfacilities at the MINUSTAH camp in Méyè,which led to the cholera outbreak. 90 Petitionersrequested a fair and impartial adjudication ofthe claim according to the terms of the SOFA,compensation to petitioners, monetary reparationsto victims of cholera at large, and a public apologyincluding acceptance of responbility for causingthe epidemic. 91 On December 21, 2011, the U.N.acknowledged receipt of the petition, and promised“a response in due course.” 92 Fourteen monthslater, on February 21, 2013, petitioners received aresponse from the U.N. Under-Secretary-Generalfor Legal Affairs, Patricia O’Brien. 93 The U.N. refusedto consider the claims because such consideration“would necessarily include a review of political andpolicy matters.” 94 Citing no precedent or authority,the U.N. response stated that this made the claim“not receivable” under Section 29 of the Conventionon the Privileges and Immunities of the UnitedNations. Thus, the U.N. effectively invoked legalimmunity to defeat the claims. On May 7, 2013,petitioners responded to the letter, challenging theU.N.’s argument that the claim was not receivable. 95Additionally, petitioners stated that if they did notreceive a timely a response within 60 days, theywould file their claims in a court of law. 96Since the 2010 outbreak, Haitians haverepeatedly expressed discontent with MINUSTAHand the U.N. for causing the cholera epidemicin the first instance and their management of itthereafter. Repeated protests since 2010 have calledfor U.N. withdrawal. The U.N., however, has notprovided a meaningful response. The organizationhas refused to consider the petition for relief or toprovide a forum to adjudicate repeated demandsthat it accept responsibility for the introduction ofcholera into Haiti. 97 To this day, the U.N. continuesto deny accountability for the epidemic or considerthe merits of any claims made by its victims.16minustah and the cholera outbreak in haiti
Chapter IIScientific InvestigationsIdentify MINUSTAHTroops as the Sourceof the Cholera Epidemic17 section
Chapter IIScientific Investigations Identify MINUSTAHTroops as the Source of the Cholera EpidemicAn extensive scientific literature has tracedthe source of the Haitian cholera epidemicto the MINUSTAH camp in Méyè. Outbreakinvestigations, environmental surveys, andmolecular epidemiological studies—includingthose conducted by the U.N.’s own experts andsome of the world’s foremost experts on choleraand infectious disease—all demonstrate thatcholera in Haiti was transmitted from a singlesource, the Méyè MINUSTAH base in central Haiti.These studies show that the peacekeepers stationedat the base, who had arrived from Nepal shortlybefore the first cases of cholera were reportedin Haiti, were carriers of a strain of V. cholerae,the bacterium (V. cholerae), the bacterium thatcauses cholera, also from Nepal. Poor sanitationconditions at the MINUSTAH camp allowed forwaste to flow into the nearby waterways, resultingin the inadvertent introduction of V. cholerae intothe Méyè tributary. The bacterium spread throughthe Tributary into the Artibonite River and otherconnected water sources. As a result, individualsconsuming water from the Méyè Tributary and theArtibonite River contracted cholera.Four key findings confirm that the epidemic’spoint source transmission—or common origin—was the MINUSTAH peacekeeping troops:• There was no active transmission of cholera inHaiti prior to October 2010. Historical recordsdating back to the 1800s report no cases ofcholera in Haiti. No cholera epidemics weredocumented in the Caribbean during the 20thcentury. During the Caribbean epidemics of the19th century, no cases were reported in Haiti.• The initial area affected by the epidemicencompassed the location of the MINUSTAHbase. Epidemiological modeling during theinitial outbreak shows no symptomatic choleracases other than in the areas surrounding theMINUSTAH camp in Méyè. Models suggestthat the origin of the disease was near theMINUSTAH base, from which cholera thenspread throughout the country.• The troops at the MINUSTAH base wereexposed to cholera in Nepal, and their fecescontaminated the water supply near the base.The peacekeeping troops stationed at theMINUSTAH base in Méyè were deployed toHaiti from Nepal, where cholera is endemicand a outbreak had occurred one month priorto their arrival in Haiti. These troops wereexposed to cholera in Nepal just prior to theirdeparture to Haiti. Due to the poor sanitationinfrastructure at the MINUSTAH base, fecesfrom the troops contaminated the ArtiboniteRiver, one of Haiti’s main water sources.• The Haiti cholera outbreak is traceable to asingle cholera strain of South Asian origin foundin Nepal. Molecular studies of stool samplescollected from multiple patients reveal a singlecholera strain as the source of infection in Haiti.Genetic analyses show that the Haitian strain isidentical to recent South Asian strains found inNepal and is most likely a descendant of thesestrains. Outbreak investigations demonstratethat the initial cases were confined to the areanear the MINUSTAH base in Méyè. Both setsof studies suggest that the outbreak beganwith the introduction of a single cholera strainendemic to parts of Nepal into the water sourcenear the MINUSTAH base.Separately, these various studies propose a linkbetween the MINUSTAH peacekeepers from Nepaland the Haitian cholera epidemic. Combined,they provide compelling evidence of the causalrelationship between the MINUSTAH troops andthe introduction of cholera into Haiti.18 scientific investigations identify minustah troops as the source of the cholera epidemic
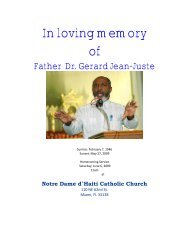
The Méyè Tributary. The MINUSTAH camp is to the left of the tributary.The left-hand side of the picture shows barricades along the perimeterof the MINUSTAH camp.Barricades along the perimeter of the MINUSTAH camp.A. Historical Records Show No Evidenceof an Active Transmission of Cholera inHaiti Before October 2010.Historical records dating back to the 19th centuryshow no evidence of cholera in Haiti prior toOctober 2010. 98 While it is difficult to confirm thehistorical absence of disease, no cholera epidemicwas reported in the Caribbean region during the20th century. 99 Historical accounts documentthree Caribbean pandemics of cholera in the 19thcentury: in 1833–1834, 1850–1856, and 1865–1872. 100 Nomedical reports document cholera in Haiti duringthese periods. 101 Researchers thus have concludedthat there were no significant cases of cholera inHaiti during the 19th or 20th centuries. 102 Historicalevidence therefore supports the conclusion thatthe 2010 outbreak was caused by the introductionof cholera into Haiti from a foreign source.B. The Initial Area Affected by theEpidemic Encompassed the Locationof the MINUSTAH Base.Geographical and temporal analyses of theHaitian cholera outbreak show that the epidemicoriginated near the MINUSTAH base in Méyè andspread downstream through the Méyè Tributaryand into the Artibonite River. Case analyses revealthat only individuals exposed to water from thisriver system initially contracted cholera.The first cholera cases documented betweenOctober 14–18 arose in Méyè and Mirebalais, just2 kilometers north of Méyè. Hospital admissionrecords and anecdotal information from theMirebalais Government Hospital showed thatbetween September 1–October 17, sporadic diarrheacases <strong>without</strong> death were seen at a consistentbaseline rate in both adults and children. 103 Thefirst recorded case of severe diarrhea necessitatinghospitalization, and the first deaths fromdehydration in adult patients occurred the nightof October 17 and early morning of October 18.During these two days, the majority of the patientpopulation was of adult age, a fact stronglysuggesting that the cause of the diarrheal caseswas cholera as severe diarrhea in adults is rare. 104Staff reported that the first cases of cholerawere attributed to an area located 150 metersdownstream from the MINUSTAH camp in Méyè. 105On October 19, clusters of patients near theArtibonite Delta were hospitalized with severeacute diarrhea and vomiting, and deaths, includingof three children, were reported by health centersand hospitals in the region. 106 Staff at the AlbertSchweitzer Hospital reported that their firstsuspected case of cholera occurred on October18, 2010, when a migrant worker arrived at thehospital already deceased. The first confirmed casesof cholera occurred at the hospital on October 20.After October 20, the number of cases admittedto the hospital was so high that exact record19scientific investigations identify minustah troops as the source of the cholera epidemic
keeping became difficult. 107 At St. Nicolas Hospitalin St. Marc, a city located 70 kilometers southwestof Mirebalais, medical records showed that aconsistently low level of diarrhea cases, mostlyamong children, remained stable until October20, when 404 hospitalizations were recorded in asingle day—one patient every 3.6 minutes—alongwith 44 deaths from cholera. These cases came from50 communities throughout the Artibonite RiverDelta region, with an average of eight patients percommunity arriving at the hospital on October 20. 108Following the early reports of cholera, theMSPP and the CDC conducted an investigation ofdisease incidence at five hospitals in the ArtiboniteDepartment from October 21st to October 23.To establish a date of onset for the outbreak,investigators reviewed medical records fromOctober 2010 for each hospital to identify casesthat required hospitalization due to diarrheaand dehydration. Because detailed medicalrecords were not available for the investigation,hospitalizations due to “severe diarrhea” were usedas a proxy for cholera cases, with a particular focuson adult patients since severe diarrhea within thisage group is considered rare. 109 From October 20–22,the majority of patients admitted with symptomsof cholera and the majority of those who diedfrom these symptoms were older than 5 years old,strongly suggesting that the cause of their illnesswas in fact cholera. 110 In addition, stool samplesfrom patients hospitalized in the administrativedepartments of Artibonite and Centre, southeastof Artibonite Department, were brought to theLNSP where rapid tests on eight specimens testedpositive for V. cholerae O1. 111Epidemiologists have modeled the Haitianoutbreak using data collected by the MSPP’sNational Cholera Surveillance System. 112 Withan “explosive” start in the Lower Artibonite, thecholera epidemic peaked within two days, andthen decreased drastically until October 31. 113Once adjustments were made for population andspatial location, the risk of contracting cholerafor an individual living downstream of the MéyèTributary was calculated at 4.91 times higher thanthe average Haitian. 114By October 22, cholera cases were noted infourteen additional communes, 115 most of themin the mountainous regions that border theArtibonite plain and in Port-au-Prince. In eachcommune, the incidence of cholera coincidedwith the arrival of patients from the borderingcommunes where affected individuals worked inrice fields, salt marshes, or road construction. 116The southern half of Haiti, in contrast, remainedcholera-free for as long as six weeks after theepidemic broke out, with clusters of the diseasegradually occurring over a slightly staggeredtimespan in the North-West, Port-au-Prince, andNorth Departments. 117Cholera emerged in Port-au-Prince on October22 with the arrival of patients from Artibonite, andremained surprisingly moderate in the capital cityfor some time after the beginning of the outbreak.From October 22–November 5, 2010, the incidence ofcholera remained moderate with an average of only74 daily cases. Although the epidemic eventuallyexploded in Cité-Soleil, a slum located in thefloodplain near the sea, internally displaced person(IDP) camps in the city remained relatively free ofcholera for up to six weeks after the epidemic brokeout. Overall, despite the earthquake-related damageto the city and the presence of many IDP camps,cholera struck less severely in Port-au-Prince thanin other departments in the country. In the Haitiancapital, the incidence rate was only 0.51% untilNovember 30. By contrast, during this same period,the following incidence rates were reported: 2.67%in the Artibonite Department, 1.86% in the CentreDepartment, 1.45% in the North-West Department,and 0.89% in North Department. The mortality ratein Port-au-Prince was also significantly lower (0.8deaths/10,000 persons compared with 5.6/10,000 inArtibonite, 2/10,000 in Centre, 2.8/10,000 in North-West, and 3.2/10,000 in North). 118 As cholera is adisease commonly associated with poor water andsanitation, slum areas, over-crowding, and flooding,the low cholera incidence and mortality rates inPort-au-Prince, and the IDP camps in particular,were unexpected. Also contrary to expectations,data showed the highest incidence of disease in therural Artibonite region.The incredible speed at which choleraspread to all seven communes near the lowerArtibonite River in Haiti strongly suggests thatthe contamination began at the Méyè Tributary.20scientific investigations identify minustah troops as the source of the cholera epidemic
2010July 28–August 14 A 1,400-case outbreak of cholera occurs in mid-western region of Nepal.October 8–21October 12October 14–19October 19October 21–23October 23Late OctoberEarly NovemberNovember 19MINUSTAH troops arrive in Haiti after a 10-day leave visiting their families in Nepal.A 28-year-old man from the town of Mirebalais, located downstream from the MéyèMINUSTAH Base, is the first cholera patient of the 2010 epidemic. This man suffers from apsychiatric condition and regularly drank untreated water from a stream fed by the MéyèTributary. The man develops profuse watery diarrhea. Less than a day after the onset ofsymptoms, he dies <strong>without</strong> medical attention. The man is not diagnosed with V. choleraethrough laboratory methods.Outbreak investigations also identify several families living in Méyè as the firsthospitalized cholera patients. These individuals exhibit cholera symptoms. Stool samplesfrom a subset of these patients test positive for V. cholerae.Haitian health officials report unusually high numbers of patients with watery diarrheaand dehydration in two of Haiti’s ten administrative departments.Additional cases of cholera are reported among the inhabitants of Mirebalais.National Public Health Laboratory (LNSP) confirms presence of V. cholerae.Haitian officials report an explosion of cases across the Artibonite River Delta.Cholera has spread to cities across the Haitian North-West and North Departments,which are roughly equidistant from the Artibonite Delta.The Haitian Ministry of Health (MSPP) reports positive cholera cases in all ten Haitianadministrative departments.The transmission of a waterborne disease likecholera across geographical regions takes aslong as it would take for the water to travel thesame distance. An Independent Panel of Experts,appointed by the U.N. to investigate the originsof the epidemic, calculated that it would take twoto eight hours for water in the Méyè Tributaryto flow from near the MINUSTAH camp’s wastefacilities to its junction with the ArtiboniteRiver. 119 The U.N. Independent Panel of Expertsalso found that a contamination of the Artibonitestarting at the Méyè Tributary would be fullydispersed throughout the Artibonite River Deltawithin a maximum of two to three days. Thistimeline, the panel noted, was “consistent withthe epidemiological evidence” showing that theoutbreak began in Mirebalais, near the MéyèTributary, and that cases of patients experiencingcholera-like symptoms appeared in the ArtiboniteRiver Delta area two to three days after thefirst cases of cholera were seen upstream inMirebalais. 120C. The Troops at the MINUSTAH Base WereExposed to Cholera in Nepal, and TheirFeces Contaminated the Water SupplyNear the Base.Epidemiological studies report that the U.N.peacekeeping troops that arrived in Méyè justbefore the Haitian cholera outbreak had beenexposed to the disease in Nepal shortly before theirdeparture to Haiti. Poor sanitation infrastructureat the MINUSTAH camp in Méyè led to fecalcontamination of the water supply near the campand near the site of the first cases of cholera inHaiti. Locals regularly used this water for drinking,cooking, and bathing.Nepalese peacekeeping troops arriving at theMINUSTAH camp in Méyè between October 8–24had been exposed to cholera in Nepal. Cholera isendemic to Nepal and the country experiencessporadic outbreaks every year. In 2010, a 1,400-case outbreak occurred in the country, beginningaround July 28 and lasting until mid-August,just prior to the Nepalese troops’ deploymentto Haiti. 121 During this outbreak, MINUSTAH21scientific investigations identify minustah troops as the source of the cholera epidemic
peacekeeping troops were training in Kathmandu.At the end of their training in late Septemberand early October, the peacekeepers received amedical evaluation, and none showed symptomsof cholera. 122 The absence of symptoms, however,did not prove that the peacekeepers were cholerafree.Cholera has a two to five day incubationperiod and can be carried asymptomatically. 123Prior to their departure for Haiti, the peacekeepersspent ten days visiting their families. 124 Afterthis visiting period, none of the troops exhibitedcholera symptoms. 125 Despite the recent choleraoutbreak in Nepal and the high risk of exposureand infection during the ten-day visitation period,none of the peacekeepers were tested for V. choleraeimmediately before their departure to Haiti. 126Once a water source like the Méyè Tributarybecomes contaminated with cholera, humanpopulations exposed to the contaminated water areprone to subsequent outbreaks. 127 The magnitude ofsuch outbreaks varies according to the probabilityof secondary transmission. 128 A higher likelihoodof such transmission exists in countries likeHaiti with poor infrastructure and inadequatesewage systems and is also associated with thefrequent arrival of foreign populations like troopdeployments from overseas.Environmental surveys conducted by theU.N. Independent Panel of Experts describethe MINUSTAH camp’s inadequate wasteinfrastructure at the beginning of the epidemic.The experts identified a “significant potentialfor cross-contamination” of shower and cookingwater waste with water waste containing humanfeces due to the poor pipe connections in themain showering and toilet area of the camp. 129The experts also noted that the construction ofthe water pipes in these areas was “haphazard,with leakage from broken pipes and poorpipe connections.” 130 The experts found thatcontamination was especially likely in an areawhere pipes “run over an open drainage ditch thatruns throughout the camp and flows directly intothe Méyè Tributary system.” 131The U.N. Independent Panel of Experts’ surveyof the MINUSTAH base and its facilities furtherobserved that disposal of human waste outsidethe camp contaminated the Méyè Tributary. Blackwater tanks, containing water contaminatedwith fecal matter from the camp, were emptied“on demand by a contracting company approvedby MINUSTAH headquarters in Port-au-Prince.” 132According to MINUSTAH staff, the companycollected the waste in a truck and deposited itin a disposal pit several hundred meters fromthe camp. 133 This pit was near the southeasternbranch of the Méyè Tributary and was susceptibleto flooding and overflow into the Méyè Tributaryduring rainfall. 134 The experts calculated that itwould take roughly two to eight hours for water toflow from the septic pit to the junction with theArtibonite River. 135Haitians who contracted cholera in the earlystages of the epidemic had consumed water fromthe Artibonite River. Almost no cases of cholerawere reported in communities along the Artibonitethat did not use water from the river. From October21–23 the MSPP and CDC investigative team issueda standardized questionnaire to a sample of 27patients in the five hospitals of the ArtiboniteDepartment. The majority of the surveyedpatients reported living or working in rice fields incommunities that were located alongside a stretchof the Artibonite River. Of the patients surveyed,67% reported consumption of untreated water fromthe river or canals connected to the Artiboniteprior to onset of symptoms, 67% did not practiceclean water precautions (chlorination or boilingof water prior to use), and 27% practiced opendefecation.Furthermore, the U.N. Independent Panelof Experts found that in the Mirebalais market,seafood was neither sold nor consumed,making a route of infection originating inthe ocean surrounding Haiti highly unlikely.This determination left the Artibonite Riveras the only potential source of the epidemic.The experts concluded that, based on theepidemiological evidence, the cholera epidemicbegan in the upstream region of the ArtiboniteRiver on October 17 and the most likely cause ofinfection in individuals was their consumptionof contaminated water from the river. In theirinitial report in 2011, the U.N. Independent Panelof Experts concluded that there was insufficientevidence to attribute the epidemic to MINUSTAH22scientific investigations identify minustah troops as the source of the cholera epidemic
troops. However, in a follow-up study released inJuly 2013, this same group of experts revised theirinitial conclusion. They explained that additionalevidence presented between 2011 and 2013demonstrated MINUSTAH troops were in fact thecause of the outbreak. 136Researchers have thus concluded thatthe Haitian cholera epidemic’s point sourcetransmission is near the MINUSTAH base in Méyè,based on a combination of three factors: 1) theMINUSTAH peacekeeping troops were exposed tocholera in Nepal prior to their deployment to Méyè;2) feces from these troops contaminated the localwater supply due to poor waste infrastructureat the camp; and 3) a few days after the Nepalesepeacekeeping troops’ arrival to the MINUSTAHbase in Méyè, Haitians drinking from the MéyèTributary and the connected Artibonite Riverexhibited cholera symptoms.D. The Haiti Cholera Outbreak IsTraceable to a Single Cholera Strainof Nepalese Origin.Epidemiological research into the origins of theHaiti cholera outbreak has repeatedly confirmedthat the Haitian strain is closely related to a familyof cholera strains from South Asia. Specifically,the Haitian V. cholerae strain has a near identicalgenetic resemblance to the strain observed inNepal in the summer of 2010.Molecular epidemiological studies suggestthe outbreak started with the introduction ofa single strain into Haiti. V. cholerae strains areclassified into sero-groups based on the structureof their bacterial membranes, and strains arefurther classified into serotypes, pulsotypes,and biotypes on the basis of various biochemicaland microbiological tests. Samples from differentspecimens of the Haitian V. cholerae strain haverepeatedly tested positive for the same sero-groupO1, biotype El Tor, suggesting the epidemic had acommon source. 137Whole genome sequencing of Haitian cholerasamples also shows that the samples share acommon genetic ancestry. Whereas sero-grouping,sero-typing, and bio-typing compare the largermolecular structures of V. cholerae cells, sequencingcompares the highly specific genetic code of thecells. Thus, sequencing provides a more preciseidentification of V. cholerae. Due to the rapidevolution of bacteria over the course of an epidemic,different samples almost never present the exactsame sequence. Instead, sequences that closelyresemble one another will indicate that theirsamples have similar origins. Over the course of theepidemic, genetic material from various Haitian V.cholerae samples has been isolated and sequenced, 138and analysis of these sequences consistently showsthat the samples are closely related to one anotherand stem from a common ancestor. 139The ancestor V. cholerae strain of the Haitianstrain responsible for the outbreak has been tracedto Nepal. Molecular and epidemiological studiesreveal that the Haitian and Nepalese El Tor O1 V.cholerae strains are closely related. Research alsoshows that the Haitian V. cholerae strain belongs tothe same El Tor O1 family as the Nepalese strains. 140Additionally, a comparison of genetic sequencesfrom the 2010 Nepalese and Haitian strains found aclose genetic resemblance between the two. 141The most contemporary strains from Nepalwere compared with the whole genome sequencesof isolates 142 from Haiti as well as those of otheravailable strains. All Nepalese isolates were foundto be similar to the Haitian isolates in both theirantibiotic resistance and susceptibility. 143 Onegenetic cluster containing four Nepalese isolateswas found to be identical to a minor variant of themain pulsotype from Haiti, 144 whereas anothercluster of four Nepalese isolates was virtuallyindistinguishable from the most commonpulsotype observed in Haiti. 145 One study foundthat only one Single Nucleotide Polymorphism 146separates the Haitian and Nepalese isolates andthat phylogenetic 147 patterns indicated a closerelationship between the Haitian and Nepaleseepidemic V. cholerae strains, thus “providingstrong evidence that the source of the Haitianepidemic was from this [Nepalese] clonal group.” 148Notably, another study of the Haitian V. choleraestrains determined that the Haitian sampleswere markedly different from Latin Americanand African El Tor O1 strains, a result “stronglysuggest[ing]” that the source of the epidemic was“the introduction of a V. cholerae strain into Haiti23scientific investigations identify minustah troops as the source of the cholera epidemic
y human activity from a distant geographicsource.” 149 This result, the study observed,countered hypotheses that “the Haitian strainarose from the local aquatic environment” or that“climatic events led to the Haitian epidemic.” 150The most recent study of the origins of thecholera epidemic provides further evidence thatthe Haitian strain of cholera has a single, foreignsource. Researchers investigating the evolutionarydynamics of V. cholerae O1 compared the wholegenome sequence of Haitian isolates collected earlyin the epidemic with isolates collected near orafter one year following the start of the outbreak,isolates recovered from more recent outbreaks, andisolates collected at other time points throughoutthe country during the CDC’s routine laboratorysurveillance of the epidemic. 151 The results of thecomparison were consistent with previous findingsthat the Nepalese isolates are the closest relativesto the Haitian strain identified to date. 152 Theresearchers “observed remarkably few differences”in the genetic makeup of the population ofHaitian isolates studied, despite the variance inthe times and locations of their collection. 153 Thisgenetic consistency provides further evidencethat the observed Haitian isolates emerged froma single source. In addition, the study calculateda molecular clock model of the epidemic thatsupports the time frame of the outbreak proposedin earlier studies and discussed above. 154Multiple scientific studies have concluded thatthe close genetic similarities between the Nepaleseand Haitian cholera strains support the hypothesisthat cholera was introduced into Haiti from aNepalese source. 155 The outbreak investigations andmolecular epidemiological studies of the Haitiancholera epidemic also suggest that a single foreignstrain of V. cholerae was introduced into Haiti in asingle event.A single study (“Hasan study”) has proposedthat the Nepalese peacekeeping troops were notthe only source of the epidemic. The Hasan studyargues that two strains—one local, one introducedby the Nepalese peacekeeping troops—wereresponsible for the cholera outbreak in Haiti.One strain, found in 48% of those infected, wasV. cholerae O1, the strain most commonly linkedto Nepal. The other strain, found in 21% of thoseinfected, was V. cholerae non-O1/O139, a strain thatthe study postulated as local in origin. The studyshowed 7% of patients were infected with both. 156The scientific authority of the Hasan study,however, has been disputed. The study does notstate the case definition of cholera—that is, it doesnot define its criteria for choosing the diarrhealcases it observes in its study. The lack of such a casedefinition calls into question the medical legitimacyof the cases studied and, as a direct result, thevalidity of the study’s conclusions on the numberof identified cholera patients. Diarrhea has multiplecauses, but the Hasan study fails to explain howcholera, as opposed to other bacterial forms ofdiarrhea, was diagnosed in the cases it studies. 157Five epidemiologists, including the author ofone of the first studies of the origins of the choleraepidemic in Haiti, have responded with skepticismto the Hasan study’s results. In their response, theynote that it is not unusual for humans to harborseveral putative pathogens that cause diarrheaand question the study’s proposal that V. choleraenon-O1/O139 could be the sole pathogen of 21% ofclinical cholera specimens in Haiti. 158 The authorsobserve that among the 435 stool specimenscollected by the LNSP between mid-October andNovember 2010, 249 harbored bacteria compatiblewith V. cholerae, and 243 were confirmed as beingO1 and El Tor, leading to a diagnosis of the presenceof V. cholerae O1, or the Nepalese strain, in thespecimens. Based on this data, the authors argue,the maximum frequency of non-O1 V. choleraecollected by the LNSP was no more than 6 out of 435samples, or 1.4%. 159 The authors thus conclude thatthe Hasan study “provided no evidence to counterthat cholera was brought to Haiti by a contingentof Nepalese United Nations peacekeeping troops.” 16024scientific investigations identify minustah troops as the source of the cholera epidemic
ConclusionScientific study of the origins of the cholera epidemic in Haiti overwhelminglydemonstrates that U.N. peacekeeping troops from Nepal introduced the diseaseinto the country. No cases of active transmission of cholera had been reportedin Haiti for at least a century prior to October 2010. The foci of the epidemicencompasses the location of the MINUSTAH base in Méyè. The peacekeepingtroops stationed at the MINUSTAH camp in Méyè at the time of the outbreak weredeployed from Nepal, where cholera is endemic and an outbreak occurred justprior to their departure, increasing their likelihood of exposure and transmission.Lastly, molecular and genetic studies demonstrate that the Haitian cholerastrain is genetically almost identical to the Nepalese strain, thus supporting thehypothesis that the outbreak originated from a single strain of cholera foreignto Haiti prior to October 2010. Although one study proposes that an additionalstrain of cholera local to Haiti contributed to the epidemic, other epidemiologistsinvestigating the outbreak have questioned this study’s methods and results.The most scientifically plausible explanation of the origin of cholera in Haiti,according to the majority of scientific research on the matter, continues to tracethe epidemic to the U.N. peacekeepers from Nepal stationed at the MINUSTAHbase in Méyè.25scientific investigations identify minustah troops as the source of the cholera epidemic
Chapter IIIThe Requirementof a Claims Commission26 section
Chapter IIIThe Requirement of a Claims CommissionBy failing to hold itself accountable for causingthe cholera outbreak in Haiti, the United Nationsviolates the very principles of accountability andrespect for law that it promotes worldwide. Underinternational human rights and humanitariannorms, which Chapters IV and V demonstrate applyto all U.N. member states as well as the organizationitself, the U.N. is accountable through appropriatemechanisms for certain wrongs it commits. Thisbedrock principle is reflected in every SOFA the U.N.has signed with countries hosting peacekeepersover the past two decades. These SOFAs requirethe creation of standing claims commissions tohear claims against U.N. peacekeepers and are oneimportant measure for ensuring U.N. accountability.However, in practice, the U.N. has refused torespect this principle of accountability, despiteits place in the U.N.’s own governing law and itscontractual agreements. Although the U.N. haspromised a standing claims commission in theSOFA, it has never once honored this obligationin Haiti or anywhere else in the world, despitehaving entered into 32 such agreements since 1990.As a result, a meaningful mechanism to ensurepeacekeeper accountability has been rendereda nullity.The introduction of cholera by U.N. peacekeepersin Haiti exemplifies why such a standing claimscommission is a vital part of any peacekeepingmission: Because U.N. peacekeepers enjoy immunityin courts of law, a claims commission is often theonly avenue an injured civilian may have to redressinjury caused by U.N. peacekeepers.This chapter describes the U.N.’s obligation—in convention, charter, and contract—to holditself accountable for wrongs it commits. In thepeacekeeping context, the U.N. is required toestablish adequate accountability mechanismsto address wrongs committed by peacekeepers.However, the U.N. routinely veers from theseobligations, including the explicit provisionsin SOFAs mandating that it create claimscommissions and fulfill the accountabilityrequirement. Instead, in the rare instances whenthe U.N. has taken any remedial steps for itspeacekeepers’ wrongdoing, the U.N. has relied ondeficient, ex post substitutes in which it sits asboth defendant and judge. Establishing a standingclaims commission would address cholera victims’claims in an unbiased and meaningful manner,and it constitutes one step the U.N. must take touphold its obligations of accountability.A. The U.N. Charter and the GeneralConvention Reflect a Bedrock Principleof Limited Immunity.Although the U.N. enjoys immunity for officialaction, this immunity does not mean impunity.On the contrary, the same legal instruments thatconfer the U.N. with immunity contemplate thecreation of accountability mechanisms to ensurethat those injured by the organization will receiveadequate redress.Both the U.N. Charter and the Conventionon the Privileges and Immunities of the UnitedNations (General Convention) contemplate a limitedimmunity checked by appropriate accountabilitymechanisms. The U.N. Charter recognizes that theorganization and its representatives “shall enjoy. . . such privileges and immunities as are necessaryfor the fulfillment of its purposes.” 161 Thus, the plainlanguage of the Charter qualifies the scope oforganizational immunity. While the Charterimplies that the organization’s immunity is notunbounded, the General Convention makes thisexplicit. Like the Charter, the General Conventiongenerally immunizes the U.N. from legal process. 162However, Section 29 of the General Convention,which is titled “Settlement of Disputes,” providesthat the United Nationsshall make provisions for appropriate modes ofsettlement of: disputes arising out of contractsor other disputes of a private law character towhich the United Nations is a party; disputesinvolving any official of the United Nationswho by reason of his official position enjoys27 the requirement of a claims commission
immunity, if immunity has not been waived bythe Secretary-General. 163The Article 29 provision has been characterizedas “an acknowledgment of the right of access tocourt as contained in all major human rightsinstruments.” 164 Thus, this provision qualifiesthe broad immunity the General Conventionotherwise grants by requiring that the U.N.provide appropriate accountability mechanismsfor disputes. As exemplified by this provision, suchsettlement resolution mechanisms are especiallyimportant where a U.N. official or organizationalentity otherwise enjoys immunity, becauseinternal settlement dispute mechanisms may bethe only avenue for injured civilians to seek relief.Moreover, this limitation on immunity and theright of judicial redress it guarantees are in serviceof the U.N.’s human rights obligations, as discussedfurther in Chapter IV.The U.N. Secretary-General has publiclyrecognized the organization’s obligation to createaccountability mechanisms under the regimeof the Charter and the General Convention. Ina series of reports interpreting Article 29, then-Secretary-General Kofi Annan explained that theU.N. has an “international responsibility” for theactivities of U.N. peacekeeping forces, and thatthis responsibility is fulfilled by the assumptionof liability through claims commissions. 165 Thisresponsibility includes “liability for damagecaused by members of forces during theperformance of their duties.” 166 The Secretary-General’s acknowledgment that “damage causedby members of the United Nations is attributableto the organization” illustrates that the U.N. itselfrecognizes that it cannot decline responsibility forwrongs it commits, including wrongs committedby its peacekeeping forces.B. The Principle of Limited ImmunityIs Reflected in the U.N.’s SOFA,Which Requires Creation of a ClaimsCommission.The principle of limited immunity establishedin these documents is also reflected in the U.N.’sSOFA with the Government of Haiti. The SOFAshields the organization from unrestrictedliability while protecting innocent individualswho may be harmed by peacekeeper action. TheSOFA “defines the relation between the force andthe host state.” 167 It specifies which actions cantrigger organizational liability, what law governspeacekeeper action in the host country, and howcivilians can receive redress if they are wronged bymembers of the organization. As written, the SOFAfulfills the U.N.’s obligations under the Charter andSection 29 of the General Convention.Prior to 1990, no uniform agreement governingthe legal arrangement between the host countryand the peacekeeping troops existed. While somepeacekeeping missions had mission-specific SOFAs,others had no SOFA at all. When no SOFA was inplace, the law governing peacekeepers was unclear,creating uncertainty for both peacekeeperspotentially subject to unnecessary liability as wellas individuals injured by peacekeepers. 168To resolve this uncertainty, the GeneralAssembly charged the Secretary-General in 1989with drafting a SOFA that could serve as a templatefor mission-specific agreements and would be usedin all future peacekeeping arrangements. 169 In 1990,the Secretary-General promulgated a model SOFAbased on “established practices” and “drawingupon earlier and current agreements.” 170 Althoughintended to serve as the basis for mission-specificagreements, 171 in practice the model SOFA has oftenbeen used <strong>without</strong> modification. Thus, the U.N. anda host country frequently enter into a peacekeepingarrangement using the model SOFA. Typically, themandate creating the peacekeeping operation willsimply incorporate the terms of the model SOFA. 172Moreover, while peacekeeping mandates in the 1990sstated that the terms of the model SOFA “should”apply, mandates in the 21st century state that thoseterms “shall” apply, underscoring its importance topeacekeeping arrangements worldwide. 173While the SOFA contains several provisionsthat immunize peacekeepers 174 from certain formsof liability, such immunity is conditioned on thetype of action in which peacekeepers are engaged. 175Specifically, the SOFA shields peacekeepers fromliability stemming from official acts, but alsomaintains the possibility of redress for civiliansharmed by unlawful or unauthorized peacekeeper28the requirement of a claims commission
ehavior. The establishment of a claims commissionmakes this balance of interests possible.Paragraph 51 of the model SOFA incorporatesthe U.N.’s legal obligations under Article 29 of theGeneral Convention and requires the establishmentof a standing claims commission:[A]ny dispute or claim of a private law characterto which the United Nations peacekeepingoperation or any member thereof is a partyand over which the courts of [host country/territory] do not have jurisdiction because ofany provision of the settled Agreement, shallbe settled by a standing claims commission tobe established for that purpose. 176Paragraph 51 also specifies that the claimscommission be comprised of three members:one appointed by the Secretary-General, one bythe host government, and a chairman jointlyappointed by both. 177 Furthermore, the paragraphprovides that in the event that the two partiescannot agree upon a chairman within 30 days ofthe appointment of the first member, either partymay request that the president of the InternationalCourt of Justice (ICJ) appoint the chairman. 178 Twomembers constitute a quorum, and all decisionsrequire approval by two members. 179To date, neither the Secretary-General nor theGovernment of Haiti has appointed a commissioner.Responding to this inaction, Haitian lawyers areconsidering a suit to compel their governmentto appoint a commissioner, 180 thereby triggeringthe creation of the commission. 181 The HaitianGovernment thus potentially holds the powerto provide redress to its people under the SOFA.However, in light of its dependency on the U.N. forsecurity and stability, 182 politically it may not be in aposition to do so.C. The U.N. Has Never Created a ClaimsCommission, and Its Reliance on ExPost Substitutes Are Inadequate toEnsure <strong>Accountability</strong>.Despite the clear obligation to create a claimscommission under the SOFA, the U.N. has neverdone so for any of its peacekeeping missions.Although in the past it has created alternativemechanisms to respond to specific claims, suchas claims review boards and mass settlementagreements, these alternatives are rarelygranted and are in practice inferior to the claimscommission guaranteed by the SOFA. 1831. The U.N. Has Never Honored the SOFA’s Promiseof a Claims Commission.Though Paragraph 51 of the model SOFAhas been incorporated into 32 peacekeepingarrangements since 1990, the Secretary-Generalhas acknowledged that the U.N. has never oncecreated a claims commission in practice, 184 evenin the face of affirmative claims and demands forthe establishment of commissions. 185 Instead, theU.N. has treated the establishment of commissionsas optional, ignoring the mandatory languageof Paragraph 51. For example, in a 1996 report,the Secretary-General stated that “two kindsof procedures” exist for the handling of thirdpartyclaims arising in peacekeeping operations:the SOFA claims commission and procedures“established internally.” The report goes on to notethat “to date, claims of a private law nature havebeen settled <strong>without</strong> resort to the establishmentof standing claims commissions.” 186 Rather thancreate a claims commission as it is required to do,the U.N. instead relies on procedures in which the“investigation, processing, and final adjudicationof claims” is, in the Secretary-General’s own words,“entirely in the hands of the Organization.” 1872. Alternatives for Claims Commissions AreDeficient and Ineffectual and Cannot BeViewed as an Adequate Fulfillment of the U.N.’sContractual Obligations under the SOFA.While the U.N. recognizes that it has never createda standing claims commission, it cites certaininternally established procedures that purportedlysatisfy its obligation to settle disputes. 188 Thesealternatives, however, are both procedurally andsubstantively inferior to the standing claimscommission it is contractually obligated toestablish, and as such are inadequate substitutes.The first alternative is a “local claims review29the requirement of a claims commission
oard.” Unlike a claims commission, which requiresthe independent appointment of three claimscommissioners, the local claims review board ismade up entirely of U.N. personnel. 189 Also unlikea claims commission, which should be a standingbody, the claims review board is convened onlyafter a dispute has arisen. In practice, claims reviewboard determinations are shrouded in secrecy—theirdecisions are never made public—and face longbacklogs in reviewing claims. 190 Many peacekeepingmissions have at some time set up internal claimsreview boards to review private-law claims. 191 Thisreflects an understanding that disputes betweensuch missions and civilians are common andforeseeable, underscoring the logic of establishing astanding commission rather than an ad hoc board.A 2009 U.N. interoffice memorandum mentionsthe existence of a MINUSTAH Local ClaimsReview Board. 192 The memorandum notes thatthe board, in 2008, recommended an ex gratiapayment (i.e., a payment made out of moralrather than legal obligation) to be disbursed to aHaitian civilian shot in the leg during a militaryoperation involving local gang members. However,because the Local Claims Review Board’s processis internal and not publicly disclosed, it is unclearhow, to what extent, and on what legal groundsthe MINUSTAH board regularly resolves disputesagainst MINUSTAH peacekeepers, or even if it stillexists. Aside from this single mention of the LocalClaims Review Board, no other information aboutit is known.The U.N. has also participated in masssettlement agreements as alternatives to claimscommissions. Unlike claims commissions or evenlocal claims review boards, mass settlements lackany established process to guide claimants inseeking redress. Instead, settlement agreementsdepend on the host country’s ability to negotiatewith the U.N. for a lump-sum amount, whichit then distributes to its injured citizens.However, “international diplomatic power isnot a characteristic typical of states hostingpeacekeepers.” 193 Whereas Paragraph 51 seeks tomitigate such power imbalances through its threememberstructure and appointments process, masssettlement agreements lack any such correctives.No host country of U.N. peacekeepers hasever successfully negotiated such a settlement,although on at least one occasion, WesternEuropean countries have done so on behalf of theirown citizens injured by peacekeepers in anothercountry. Specifically, from 1965 to 1967, the UnitedNations acceded to demands from the governmentsof Belgium, Greece, Italy, Luxembourg, andSwitzerland to pay compensation related to deathsand injuries of their citizens as a result of U.N.peacekeeping operations in the Congo. 194 No recordof settlements on behalf of injured Congolesecitizens, however, exists. Such history stronglysuggests the inadequacy of mass settlementagreements as a fair substitute for a standingclaims commission.Predicating settlement of dispute on acountry’s power or on a panel made up entirely ofU.N.-appointed officials when the U.N. is a party tothe dispute is inconsistent with fair adjudication.By contrast, the standing claims commissionenvisioned in the SOFA promises fair judgmentby requiring the appointment of impartialadjudicators, hearing claims individually, and,crucially, predating the damage caused by the U.N.D. The SOFA Requires the U.N. to Establisha Claims Commission to Hear theClaims of Cholera Victims.Had a claims commission been in place when thecholera outbreak occurred, the U.N. would havebeen required to address the victims’ claims in atimely and meaningful manner. Like the modelSOFA, the SOFA signed by the Government of Haitiand the U.N. states that claims of a “private lawcharacter . . . shall be settled by a standing claimscommission.” 195 Despite this plain and mandatorylanguage, the claims commission was never set up.In November 2011, over 5,000 Haitian victimsof the outbreak filed a petition for relief withthe chief of the Claims Unit of MINUSTAH. Thepetition alleged that the U.N. had failed to establisha standing claims commission as required bythe SOFA. It argued that because claims arisingfrom the cholera outbreak were “private lawdisputes” within the ambit of Paragraph 55 ofthe MINUSTAH SOFA, the claims commission,once established, should be the designated forum30the requirement of a claims commission
to hear such a complaint. 196 The petition askedfor the establishment of a fair and impartialstanding claims commission as well as monetarycompensation for injuries suffered. 197The U.N. acknowledged receipt of theclaims after they were filed, but did not respondsubstantively until February 20, 2013, when itsummarily rejected the complaint, claiming that itwas “not receivable” because the claims touched ona “political and policy matter.” 198 In its statement,the U.N. made no mention of its own contractualobligation to establish a claims commission to hearprecisely the type of complaints Haitians seek tobring. As a result, Haitians affected by an outbreakstemming from the U.N.’s own actions may nowhave no forum in which to seek redress.The SOFA’s claims commission is vital toredressing the cholera outbreak for three reasons:(1) because the U.N. was contractually requiredto do so; (2) because the cholera victims’ injuriesare exactly the kind of claims such a commissionshould be tasked with hearing; and (3) becausethe U.N.’s failure to create a claims commissioneffectively forecloses all other avenues of relief.1. MINUSTAH Was Required by Its Own Contractto Create a Claims Commission.As it has in at least 32 peacekeeping agreementssince 1990, the U.N. promised the creation of aclaims commission in the SOFA it signed with theGovernment of Haiti when MINUSTAH was createdin 2004. 199 In Paragraph 55, which is titled “Settlementof Disputes,” the agreement promises that:Except as provided in paragraph 57 [whichcovers disputes between MINUSTAH andthe Government of Haiti over interpretationof the SOFA], any dispute or claim of aprivate-law character, not resulting fromthe operational necessity of MINUSTAH, towhich MINUSTAH or any member thereofis a party and over which the courts of Haitido not have jurisdiction because of anyprovision of the present Agreement shall besettled by a standing claims commission tobe established for that purpose. One membershall be appointed by the Secretary-Generalof the United Nations, one member by theGovernment and a chairman jointly by theSecretary-General and the Government. 200As in the model SOFA, the MINUSTAH SOFAcontemplates a claims commission that is standingand mandatory. In addition, like the modelSOFA, the MINUSTAH SOFA requires at least oneadjudicator who is not appointed by the U.N. inorder to ensure impartiality in the adjudication.2. A Demand for Individual Redress for theIntroduction of Cholera Is a Prototypical“Dispute of a Private <strong>Law</strong> Character” asContemplated by the SOFA.Paragraph 55 of the MINUSTAH SOFA limits thejurisdiction of claims commissions to “dispute[s]or claim[s] of a private law character.” The choleravictims’ complaints clearly constitute privatelawclaims squarely within the jurisdiction ofthe claims commission. The core of the claims—namely, requests for compensation for illness anddeath of private citizens resulting from improperactions by peacekeepers that led to contaminationof the Haitian water supply—sound in tort, aclassically private law domain. 201Characterizing the victims’ claims as “disputesof a private law character” is consistent withaccepted understanding of the distinctionsbetween public and private law. For example, akey distinction between public and private lawclaims is the identity of the complainant. Publiclaw claims may exist between governments or beinitiated by a public authority. By contrast, privatelaw claims are brought by private citizens. 202 Therequested remedy also sheds light on whetherthe claim is public or private in nature. In thiscase, the victims’ claims were for monetarycompensation, 203 a traditional private law remedy.This conclusion comports with guidance fromthe Secretary-General on the application of claimscommissions to disputes of a private law character.This guidance cites “third party claims forcompensation for personal injury/death or propertyloss/damage” as the kind of dispute a claimscommission should hear. 204 Because the choleravictims’ claims were claims for compensation for31the requirement of a claims commission
personal injury or death, they are of an appropriatesubject matter for a claims commission under theMINUSTAH SOFA. Although the U.N. statementrejected the victims’ claims on the ground thatthey touched on a “political or policy matter,” theclaims are, in fact, quintessentially of a private lawcharacter and thus are appropriate for adjudicationby a claims commission.3. The Cholera Outbreak Did Not Arise out of an“Operational Necessity.”In addition to requiring that claims be of a “privatelaw character,” Paragraph 55 prohibits a claimscommission from hearing claims that arise out of“operational necessity.” 205 “Operational necessity”consists of those “necessary actions taken by apeacekeeping force in the course of carrying outits operations in pursuance of its mandates.” 206According to the Secretary-General, operationalnecessity takes into account four elements: (1) agood-faith conviction (in other words, a sincerebelief that the course of action at issue wasnecessary to realizing the peacekeeping operation’smandates); (2) strict necessity, rather than mereconvenience or expediency; (3) execution in pursuitof an operational plan; and (4) proportionalitybetween damage caused and necessity for theoperational goal. 207In the case of the cholera outbreak, none ofthese requirements are met. Dumping cholerainfectedwaste in a river cannot be deemed an“operational necessity.” These actions were in noway necessary for the furtherance of the U.N.’smission. At most, failing to outfit the MINUSTAHcamp with adequate waste infrastructure mighthave been “convenient” or “expedient,” but it wasnot “necessary” to the U.N.’s mission of stabilizingHaiti. The U.N.’s role in causing the outbreak simplycannot be classified an “operational necessity,”particularly when considering the extent of thedevastation caused by the cholera outbreak.4. Without a Claims Commission, HaitianVictims May Never Have a Forum in Which toBring Their Claims.While the cholera victims have claims well withinthe purview of a judicial forum, <strong>without</strong> thecreation of a claims commission, they may haveno opportunity to have their grievances redresseddue to the generous immunity afforded the U.N.and its employees (acting in their official capacity)from suit in courts of law. 208 Indeed, it is preciselybecause of this immunity that settlement disputemechanisms were created.Article 29 of the General Convention and Article55 of the MINUSTAH SOFA carve out a narrowexception to the general rule that U.N. officials areprotected from judicial scrutiny of their actions.Although scholars disagree about whether U.N.officials in Haiti enjoy only functional (thatis, limited to actions stemming from officialfunctions) immunity, it is still extremely difficultto overcome this immunity to sue them in a courtof law. 209 Under the SOFA, civil suits can onlyproceed if the commander of the mission approvesthem, and even if the commander does so, it is“nearly impossible” to litigate within the Haitianlegal system. 210While it is possible that the U.N. may set upan internal claims review board or enter intosettlement negotiations with the Government ofHaiti, it is unlikely that either of these avenues willvindicate the victims’ right to a forum where theycan have their grievances meaningfully redressed.As discussed above, these internal mechanisms arefar inferior to a claims commission, both becausethey are set up after the injury—as opposed to“standing” throughout the course of a peacekeepingmission—and because they are not impartial.32the requirement of a claims commission
ConclusionUltimately, a claims commission is the only meaningful forum in which victimsmay press their claims. Furthermore, it is the very process that the U.N. itselfhas contemplated in all of its peacekeeping agreements, as well as in its foundingdocuments. Lastly, as Chapter IV emphasizes, it is also a concrete example of theU.N. fulfilling its obligation to provide access to remedies for violations of humanrights, especially when, as here, the U.N.’s actions led to massive amounts ofpreventable death and illness. However, while establishing a claims commissionis necessary for the U.N. to meet its obligations under the SOFA, it is neither asufficient nor complete remedy for the U.N.’s introduction of cholera into Haiti.Chapter IV addresses the broader range of reparations to which victims of thecholera epidemic are entitled under international human rights law.33the requirement of a claims commission
Chapter IVThe U.N. Has Failed toRespect Its InternationalHuman Rights Obligations34 section
Chapter IVThe U.N. Has Failed to Respect ItsInternational Human Rights ObligationsThe United Nations is responsible underinternational human rights law for the choleraepidemic it has caused in Haiti. AlthoughU.N. accountability for actions that disregardinternational human rights law was onceconsidered a novel proposition, increasinglyscholars and policymakers, including keyfigures within the U.N., have concluded that ablanket denial of legal obligations for the U.N.is incompatible with international law andinternational human rights law. 211 Reports ofU.N. peacekeepers committing a range of humanrights abuses in Haiti have been dismayinglyfrequent throughout MINUSTAH’s presence in thecountry. 212 These reports have made the propositionthat the U.N. need not answer for such violationsall the more untenable.The principle of U.N. accountability underinternational human rights law is rooted intwo key premises. First, the U.N.’s capacity toincur legal obligations under international law,and international human rights law—its legalpersonality—is well-settled. Second, scholars,policymakers, and U.N. officials have highlightedthat one of the U.N.’s institutional purposes isthe promotion of human rights. Such promotionentails a duty on the part of the U.N. and its agentsto respect the international human rights lawthat it promotes. MINUSTAH’s specific chargeto promote human rights and respect Haitianlaw—law that includes Haitian human rightsobligations—further supports this conclusion.The range of human rights that the U.N.,operating through MINUSTAH, must respect isdetermined by standards established in humanrights treaties and obligations under customaryinternational law. Through its contractualcommitment under the SOFA to respect Haitianlaws, which includes Haitian treaty-based humanrights obligations, the U.N. has assumed dutiestoward the Haitian people based on their rightsunder these treaties. In first bringing cholera toHaiti and then attempting to foreclose any remedyfor harms caused by the epidemic, the U.N. hasneglected its duties to respect and promote thoserights set out in Haitian treaty obligations as wellas accepted international norms and customaryinternational law.In Haiti, the U.N. has committed a seriesof failures. It negligently failed to prevent theintroduction of cholera bacterium brought by itspeacekeepers into a major Haitian waterway andthen failed to provide any form of remedy to thevictims. These failures are now compounded by theU.N.’s failure to guarantee non-repetition of similarharms, a guarantee that includes taking adequatesteps toward ameliorating the epidemic. Each ofthese failures is also a failure to respect humanrights—specifically, the rights to water, health,life, and an effective remedy. In failing to respecthuman rights, the U.N. has also failed to uphold itsobligations under international human rights law.The failures of U.N. actors to respect thesefundamental human rights must have visibleconsequences if the U.N.’s global operations are toretain legitimacy. The need for such accountabilityis especially acute when these failures arise fromthe activities of peacekeeping operations likeMINUSTAH, mandated to promote and respecthuman rights, in poor countries like Haiti thatlack sufficient infrastructure to prevent or controlthe harms that stem from such failures. Therecognition of this need adds a moral dimensionto the argument for U.N. accountability underinternational human rights law: In light of theU.N.’s critical role in developing and promotinghuman rights globally, the U.N. must demonstratethe same commitment to comply with internationalhuman rights law that it demands fromstates and other non-state actors, or risk losing itsmoral authority to make these demands at all.35 the u.n. has failed to respect its international human rights obligations
A. The U.N. Can Have Duties and Liabilitiesunder International <strong>Law</strong>.The U.N. has long acknowledged that it canpossess legal obligations under international law.This possibility extends to international humanrights law, which is a subset of international law.Article I of the General Convention codifies theorganization’s international legal personality. 213The ICJ later affirmed that the U.N. is, “a subjectof international law . . . capable of possessinginternational rights and duties.” 214 These rightsand duties “must depend upon [the U.N.’s]purposes and functions as specified or impliedin its constituent documents and developed inpractice.” 215 As one of the U.N.’s purposes is theachievement of international cooperation “inpromoting and encouraging respect for humanrights,” 216 the U.N. cannot possess any right or dutyunder international law that hinders its ability topromote or encourage respect for human rights.The U.N. has also formally recognized that itslegal personality renders it liable for the actionsof its peacekeeping operations. As noted inChapter III, in a 1995 report discussing the scopeof U.N. liability for peacekeeping troops, thenSecretary-General Kofi Annan acknowledged thatthe “international responsibility” of the U.N. forthe activities of its forces “is an attribute of itsinternational legal personality and its capacity tobear international rights and obligations.” 217 Theseinternational obligations and liability for theirbreach area reflection of the principle of Stateresponsibility—widely accepted to beapplicable to international organizations—thatdamage caused in a breach of an internationalobligation and which is attributable to theState (or to the Organization), entails theinternational responsibility of the State(or of the Organization) and its liability incompensation. 218In 2004, United Nations Legal Counsel to theDirector of the Codification Division reiterated thisprinciple, stating that “an act of a peacekeepingforce is, in principle, imputable to the Organization,and if committed in violation of aninternational obligation entails the internationalresponsibility of the Organization and its liabilityin compensation.” 219Thus, as the U.N. itself has recognized, whena peacekeeping force breaches an internationalobligation of the U.N., the organization isresponsible both for the breach and for remedyingit. This rule extends to MINUSTAH’s activitiesin Haiti, and therefore the U.N. must beaccountable for MINUSTAH’s breaches of the U.N.’sinternational obligations.B. The U.N. Is Obligated to RespectHuman Rights.The U.N.’s foundational commitments, as wellas the contractual obligations of MINUSTAH toHaiti, give rise to its specific obligation underinternational law to respect internationalhuman rights. It is undisputable that one ofthe U.N.’s purposes includes the promotion andencouragement of respect for human rights; theU.N. Charter obligates the organization to “promote. . . universal respect for, and observance of, humanrights,” and requires member states of the U.N. to“pledge themselves” to cooperate with the U.N. inachieving this obligation. 220 Similarly, the ViennaDeclaration and Programme of Action of 1993identifies “[t]he promotion and protection of allhuman rights” as a “priority objective” of the U.N.and notes that the “processes of promoting andprotecting human rights should be conducted inconformity with . . . international law.” 221The MINUSTAH mandate promotes thesehuman rights objectives in Haiti by requiringthe peacekeeping operation to “support theTransitional Government and Haitian humanrights institutions and groups in their efforts topromote and protect human rights.” 222 While theprecise meaning of “promote” is not supplied in theU.N. Charter or the MINUSTAH mandate, a humanrights breach would obviously fall outside of itsdefinition. As the ICJ has recognized, “[A] denial offundamental human rights is a flagrant violationof the purposes and principles of the Charter.” 223Because the U.N. and MINUSTAH cannot fulfilltheir purposes to promote and support the36the u.n. has failed to respect its international human rights obligations
promotion of human rights while simultaneouslyacting in ways that disrespect human rights, thefulfillment of their mandate requires that theiractions be guided by human rights standards.The scope of human rights law that theU.N. must respect is determined in part byHaiti’s international law obligations. The SOFArequires MINUSTAH to “respect all local lawsand regulations” of Haiti. 224 These “local laws andregulations” include any treaty provisions to whichHaiti has committed. 225 As the U.N. is liable for anybreaches by MINUSTAH of its legal obligations, 226 itis responsible for the consequences of MINUSTAH’sfailure to respect Haitian laws and regulations,including its human rights treaty commitments.Moreover, the U.N.’s legal personality alonesuggests that it may be judged according tocustomary international law, including customaryinternational human rights law. 227 The U.N. canbe legally bound to customary international law,defined by the ICJ as “evidence of a general practiceaccepted as law,” 228 or any international humanrights standards that have been similarly widelyaccepted as general principles of law, 229 because theforce of customary international law comes fromits practice, not from its codification in treaties. 230Unlike treaty obligations, which only attach toparties if and when they consent by signing oracceding to the treaty, 231 customary internationallaw obligations are conferred upon any entity thatcan possess international obligations. 232 Givenits legal personality, the U.N. is one such entity,and thus can be legally obligated to comply withcustomary international law. 233Furthermore, if the U.N. fails to comply withinternational human rights law—law that it hashelped to develop, promote, and protect—the U.N.risks losing its moral authority to demand thatstates and other international actors comply withit. One of the U.N.’s primary objectives, expressedin the preamble of its Charter, is to “reaffirm faithin fundamental human rights.” 234 For decades,the U.N. has repeatedly institutionalized itscommitment to the promotion of human rights. 235Further, since its inception, the U.N. has overseenthe development, ratification, and implementationof countless international human rightstreaties and has issues even more resolutions,recommendations, and comments clarifyingand elaborating those legal obligations that areconcomitant with human rights protections. 236Having committed to the global advancement ofinternational human rights, the U.N.’s appeals tostates to respect human rights carry a uniquelyauthoritative force. The U.N.’s refusal to similarlyrespect these rights, however, threatens to sapthese appeals of their authority and legitimacy.C. The U.N. Has Failed to Respect HumanRights in HaitiBy polluting a major Haitian water source withhuman waste contaminated with the cholerabacterium carried by U.N. troops, resulting in thedeaths of thousands and the infection of hundredsof thousands, and subsequently refusing to provideany remedy for the injury its negligence caused,the U.N. has clearly contravened its obligationsunder international law to respect, promote, andprotect human rights. MINUSTAH’s depositing ofcholera-laced human waste into the ArtiboniteRiver failed to respect the victims’ human right towater. The victims’ contraction of cholera from thepolluted river water, and their resultant sicknessand, in many cases, death, stemmed from a failureto respect their human rights to health and life.And the U.N.’s failure to provide any form of redressto its victims for their loss and injury fails torespect their human right to remedy.1. The U.N. Has Failed to Respect the Rightto Water.The U.N. has led the international effort to developand recognize the human right to water. In 2010,the General Assembly adopted a resolution onthe human right to water and sanitation that“recognizes the right to safe and clean drinkingwater and sanitation as a human right that isessential for the full enjoyment of life and all humanrights,” and calls upon international organizations,among others, to provide financial and otherresources to help developing countries expeditetheir efforts “to provide safe, clean, accessible andaffordable drinking water and sanitation for all.” 237The Human Rights Council of the U.N. has also37the u.n. has failed to respect its international human rights obligations
issued a resolution acknowledging the human rightto water and affirming its origins in the bindingrights to an adequate standard of living, the highestattainable standard of health, and life. 238 The Inter-American Court of Human Rights, which judiciallyoversees the fulfillment of commitments madeunder the American Convention on Human Rightsratified by Haiti in 1977, has further interpretedthe right to life under the American Convention toinclude access to safe drinking water and sanitation,and has attributed deaths resulting from lack ofaccess to clean water to the state’s failure to provideadequate water and sanitation. 239The U.N. Committee on Economic, Social,and Cultural Rights has set guidelines for therealization of the right to water. The committee,which has found that the right to health and rightto an adequate standard of living established inthe International Covenant on Economic, Social,and Cultural Rights (ICESCR) include access to safedrinking water and sanitation, has stated that “safe”water means water “free from micro-organisms,chemical substances and radiological hazards thatconstitute a threat to a person’s health.” 240 Violationsof this right can occur through “the direct actionsof State parties or other entities insufficientlyregulated by States” and involve, among otherthings, “pollution and diminution of waterresources affecting human health.” 241 For states thathave resource constraints limiting their ability tofully realize the right to water, the committee notesthat they “have a constant and continuing dutyunder the Covenant to move as expeditiously and iteffectively as possible” toward full implementationof the right. 242The U.N.’s negligent oversight of its ownpeacekeeping forces’ water and sanitationpractices, which caused human waste to leak intothe tributary of a major Haitian water source andpollute the main source of water for hundreds ofthousands of people, was a clear failure to respectthe human right to water. The MINUSTAH camp’shaphazardly constructed waste infrastructure,which allowed for waste from the camp’s drainagecanal and an open drainage ditch to flow directlyinto the Méyè Tributary, 243 virtually guaranteedcontamination of the nearby water systems. Asa result, the many people who relied on naturalwater resources for drinking, cooking, and bathingwere deprived of their human right to water.Notably, MINUSTAH’s pollution of the Artibonitewas not the result of insufficient regulation byHaiti, as the Government of Haiti is not in aposition to “regulate” the U.N., but rather theconsequence of MINUSTAH’s violation of Haitianlaws prohibiting the disposal of human waste intonatural water resources. 244The U.N.’s failure to respect the human rightto water was especially troubling in Haiti, wheretreated or potable water was and remains a scareresource for many; 245 a 2006 study found that nearly90% of Haitians lack access to piped water, andonly 17% have access to improved sanitation. 246The cholera epidemic has only diminished theavailability of clean water, while increasing theneed for it. Because cholera is a waterborne diseasethat causes illness and death through dehydration,access to clean water is essential to treatmentand prevention. 247 Further, the U.N.’s negligentpollution of the Artibonite greatly impedes Haiti’sability to realize its own duty, under the ICESCR, toexpeditiously realize the human right to water.2. The U.N. Has Failed to Respect the Rightto Health.The human right to health is widely recognizedin international human rights law and standards.The Universal Declaration of Human Rights(UDHR) states that “[e]veryone has the right toa standard of living adequate for the health andwell-being of himself and his family.” 248 TheICESCR acknowledges “the right of everyone to theenjoyment of the highest attainable standard ofphysical . . . health.” 249 The Convention on the Rightsof the Child (CRC), Convention on the Eliminationof All Forms of Discrimination against Women(CEDAW), Convention on the Rights of Persons withDisabilities (CRPD), and the Convention on theElimination of All Forms of Racial Discrimination(CERD) all provide that children, women, racialminorities, and people with disabilities should enjoythe highest attainable standard of health <strong>without</strong>discrimination. 250 The American Declaration onthe Rights and Duties of Man, which the Inter-American Court of Human Rights has held as a38the u.n. has failed to respect its international human rights obligations
source of binding international obligations formembers of the Organization of American States,including Haiti, deems the “the preservation of. . . health through sanitary and social measures . . .to the extent permitted by public and communityresources” an essential human right. 251The ICESCR, CRC, and U.N. Committee onEconomic, Social, and Cultural Rights have allelaborated on what measures must be taken tocomply with the right to health. The ICESCRprovides for the achievement of the right to healththrough “[t]he improvement of all aspects ofenvironmental and industrial hygiene [and] . . .[t]he prevention, treatment and control of epidemic,endemic, occupational and other diseases.” 252 Underthe CRC, the right to health to which childrenare entitled must be protected by the “combat [of]disease . . . taking into consideration the dangersand risks of environmental pollution.” 253 TheCommittee on Economic, Social, and CulturalRights includes access to safe and potable water andadequate sanitation within the right to health. 254Much like the right to water, the committeeemphasizes that the right to health must beimplemented as expeditiously and effectively aspossible by resource-constrained states and notesthat those whose right to health has been violatedshould have access to appropriate remedies. 255 Thecommittee also acknowledges that when providinghumanitarian aid, “given that some diseases areeasily transmissible beyond the frontiers of a State,the international community has a collectiveresponsibility to address this problem.” 256By failing to prevent the introduction ofcholera into Haiti, the U.N. failed to respect thehuman right to health. The MINUSTAH camp,which housed peacekeepers from a country wherecholera is endemic and where multiple choleraoutbreaks had occurred shortly before theirdeployment to Haiti, 257 lacked adequate water andsanitation infrastructure that the U.N. shouldhave provided. Such conditions made the camp’spollution of the nearby Méyè Tributary withcholera-infected human waste nearly inevitable.The U.N.’s negligent introduction of cholerainto Haiti disregarded its duty to prevent thetransmission of communicable diseases that, asnoted above, the U.N. Committee on Economic,Social, and Cultural Rights has determined thehuman right to health requires. Moreover, theU.N.’s creation of a major public health crisis inHaiti further hinders the country’s attempts tocomply with its own obligations under the humanright to health.3. The U.N. Failed to Respect the Right against theArbitrary Deprivation of Life.The right to life and the right against arbitrarydeprivation of that life recur throughout internationalhuman rights law. Article 3 of the UDHRstates, unequivocally, that “[e]veryone has the rightto life, liberty and security of person.” The CRCrecognizes the “inherent right to life” that everychild enjoys. The American Convention and theAmerican Declaration of the Rights and Duties ofMan both affirm the right of everyone to life andto the protection of this life by law. The ICCPRdeems the right to life “inherent” in “[e]very humanbeing,” demands that “[t]his right . . . be protectedby law,” and forbids the arbitrary deprivation oflife. The Human Rights Committee advises thatthe right to life not be “narrowly interpreted” andsuggests that the right to life can be protectedby adopting, among other things, “measures toeliminate . . . epidemics.” 258With over 8,100 lives already claimed by thecholera epidemic, the U.N.’s role in causing theepidemic has undeniably demonstrated a failure torespect the human right to life. Rather than takemeasures to control and eliminate epidemics, asthe U.N. Human Rights Committee has suggestedstates do to effectuate the right to life, the U.N.created an epidemic in Haiti. The U.N.’s failureto prevent cholera’s introduction into the majorwaterway of a post-earthquake country, wherean adequate water and sanitation system wasstill developing, arbitrarily deprived thousands ofHaitians of their lives.39the u.n. has failed to respect its international human rights obligations
4. The U.N. Failed to Respect the Right to anEffective Remedy.The human right to an effective remedy for theviolation of an international obligation is wellestablishedthroughout international humanrights law. The UDHR, understood to be the“international standard of human rights,” 259with many of its components a critical part ofcustomary international law, 260 recognizes that“[e]veryone has the right to an effective remedyby the competent national tribunals for actsviolating the fundamental rights granted to himby the constitution or by law.” 261 Indeed, the rightto an effective remedy has entered the catalogof customary international law norms. 262 TheAmerican Convention provides everyone the rightto “simple and prompt recourse . . . to a competentcourt or tribunal for protection against acts thatviolate his fundamental rights recognized by theconstitution or laws of the state concerned or bythis Convention.” 263 The ICCPR, CERD, CRC, andICESCR, all treaties to which Haiti has accededor ratified, affirm a right to remedy for victims ofviolations of international human rights law. 264The human right to remedy encompasses anumber of substantive requirements, includingrestitution and the guarantee of non-repetition,developed by U.N. human rights organs. TheHuman Rights Committee has stated that theright to remedy requires reparation to those whoserights under the ICCPR have been violated, andthat reparation “generally entails appropriatecompensation” and “can involve restitution,rehabilitation and measures of satisfaction, suchas public apologies, public memorials, guaranteesof non-repetition and changes in relevant lawsand practices . . . [and] bringing to justice theperpetrators of human rights violations.” 265 TheBasic Principles and Guidelines on the Right toa Remedy and Reparation for Victims of GrossViolations of International Human Rights<strong>Law</strong> and Serious Violations of InternationalHumanitarian <strong>Law</strong> (Basic Principles), a GeneralAssembly resolution of recommendations forstate’s implementation of the right, affirmsthat victims should be provided with “full andeffective reparation,” which includes compensationand guarantees of non-repetition. 266 The BasicPrinciples further provide that, “[i]n cases wherea person, a legal person, or other entity is foundliable for reparation to a victim, such party shouldprovide reparation to the victim.” 267 In adoptingthe Basic Principles, the General Assemblyrecognized that the right to remedy “reaffirms theinternational legal principles of accountability,justice and the rule of law.” 268The ICJ and Inter-American Court bothhave acknowledged that the right to remedyentails guarantees of non-repetition. The ICJhas developed a doctrine for guarantees of nonrepetition,most prominently in the LaGrandcase, 269 that requires that specific steps towardpreventing future repetition of a human rightsbreach be taken when the breach makes fullrestitution impossible. In LaGrand, Germany suedthe U.S. for executing two German citizens after alegal technicality barred judicial consideration oftheir claim for release from imprisonment. Afterfinding for Germany, the ICJ held that the casepresented an “exceptional circumstance” where,because the victims had already been executed, theonly effective remedy would be for the perpetratorsto take concrete measures toward preventing thesame fate from befalling others in the future. TheInter-American Court similarly has establishedthat if full restitution, “which consists of restoringa previously-existing situation,” is not practicable,the entity responsible for the breach of a dutyunder human rights must provide its victimscompensation for the damages caused by thebreach and take measures to prevent the breachfrom reoccurring. 270By attempting to foreclose any potentialremedy for individuals in Haiti who contractedcholera from MINUSTAH, 271 the U.N. failed torespect the right to remedy. The U.N.’s refusalto implement a claims commission, waive itsimmunity, or apologize for the harms caused byits negligence denies the victims the possibilityof redress or compensation for their suffering. TheU.N.’s repeated denial of any responsibility for theintroduction of cholera into Haiti deprives thevictims of an apology. The U.N.’s unwillingness tomake any effort to ensure that its peacekeepingforces do not create a similar crisis in the future40the u.n. has failed to respect its international human rights obligations
is no guarantee of non-repetition. Rather, the U.N.has thus far resisted implementing measures toprevent future introduction of cholera into cholerafreeregions, as Haiti once was, by peacekeepers.As of May 2013, it has implemented only two ofthe U.N. Panel of Independent Experts’ sevenrecommendations for responding to the outbreak. 272This resistance greatly risks the possibility thatpeacekeepers in Haiti and elsewhere will continueto negligently dispose of their waste.The remedy provisions of the GeneralConvention and SOFA, which include theestablishment of a claims commission in the eventthat the U.N. causes harm, are consistent withthe U.N.’s obligation to respect the human rightto remedy. The U.N.’s failure to establish such acommission to hear the cholera victims’ claims,or waive its immunity so that the victims canbring their claims to a judicial forum, effectivelydenies the victims any remedy at law and thusfails to respect their right to remedy. The GeneralConvention and SOFA require the U.N. to providesome form of remedy for civil disputes involvingthe U.N. and MINUSTAH, thus ensuring that theU.N.’s broad immunity from suit is not distortedinto an abdication of legal accountability. 273While the U.N.’s obligations under the GeneralConvention and SOFA are necessary in satisfying theright to remedy, they are not sufficient. The U.N.’sfailure to take meaningful steps to respond to theongoing epidemic in Haiti further compounds theharmful effects of its initial violations. At minimum,an acceptance of its obligations under the humanright to remedy in Haiti should require the U.N. toredouble its efforts to ensure that future sickness anddeath do not result from its action or inaction.41the u.n. has failed to respect its international human rights obligations
ConclusionMINUSTAH’s introduction of cholera into Haiti, the U.N.’s subsequent denial ofany redress to the victims, and its failure to effectively respond to the ongoinghealth crisis constitute actionable wrongs under international human rights law.The U.N.’s legal obligations under such law extend from its legal personality, itsfoundational purpose to respect, promote, and protect human rights, its liabilityunder the SOFA for MINUSTAH’s failures to respect Haitian laws, including Haitiantreaty duties, and its duties under customary international law. By failing torespect the human rights to water, health, life, and remedy of the victims of thecholera epidemic, the U.N. breached these obligations. In so doing, the U.N. hasundermined the moral authority it requires to ensure that states comply with andrespect these same human rights. These U.N. failures have serious implications forthe overall legitimacy of the U.N.’s peacekeeping authority in Haiti and elsewhere.42the u.n. has failed to respect its international human rights obligations
Chapter VThe U.N.’s ActionsViolated Principlesand Standards ofHumanitarian Relief43 section
chapter VThe U.N.’s Actions Violated Principles andStandards of Humanitarian ReliefHumanitarian principles and standards serveas important tools to evaluate the U.N.’s actionsin Haiti through its local mission. Over the pasttwo decades, humanitarian relief organizationshave established frameworks for deliveringhumanitarian assistance in emergencies thatare now widely accepted in the internationalaid community. These frameworks developed toprevent relief organizations from unintentionallyharming humanitarian aid recipients whengiving aid. Historically, the InternationalCommittee of the Red Cross (ICRC) and otherNGOs have primarily articulated these principlesand standards. Increasingly, however, otherhumanitarian actors, including U.N. bodiesand agencies, have begun to adopt and promotethem. Indeed, the latter institutions have had animportant role in developing these frameworks andhave incorporated them into their own guidanceand handbooks.Today, these principles and standards provide aset of minimum voluntary obligations that the ICRCand NGOs have pledged to observe in humanitarianrelief efforts. These frameworks for humanitarianrelief serve an important regulatory function.Reflecting a concern for the dignity of populationsreceiving humanitarian aid, they seek to bothpromote delivery of quality aid and avoid harmingpopulations in need. In addition, these principlesand standards bridge a gap. Many humanitarianactors working in emergency settings perform statelikefunctions in the absence of a strong functioningstate. Such non-governmental actors, in takingon state-like responsibility and authority, mayunintentionally inflict harms on local populations.However, they are not governed by the same legalframeworks that render states liable for inflictingthese same harms.Since its formation in 2004, MINUSTAH has hada particularly broad mandate that encompassesboth peacekeeping and humanitarian functions.Subsequent amendments to the originalMINUSTAH mandate have reflected a similarlybroad agenda for the mission. Particularly inthe months following the 2010 earthquake,MINUSTAH took an active role in deliveringhumanitarian relief in Haiti. As a humanitarianactor, MINUSTAH has often performed state-likefunctions, including building infrastructure anddelivering food aid. Such actions can potentiallyinflict unintended harm on the people receivingaid. The cholera epidemic is a tragic example of thispotential. Had MINUSTAH followed the establishedprinciples and standards of humanitarian relief, itcould have avoided causing this harm, improvedthe quality of its humanitarian assistance, andsafeguarded the dignity of the Haitian people itintended to aid.MINUSTAH’s introduction of cholera into Haitihas violated widely agreed-upon principles andstandards of humanitarian relief intervention. First,MINUSTAH has violated the “do no harm” principle.Compliance with this general principle entailsobserving minimum water, sanitation, and hygienerequirements to prevent the spread of disease. InMéyè, MINUSTAH’s poor maintenance of the base’ssewage facilities in a post-emergency situationintroduced cholera into the Haitian water system,ultimately infecting hundreds of thousands. Second,after violating the do no harm principle, MINUSTAHviolated the principle of accountability to affectedpopulations. Humanitarian relief standardshave emphasized the importance of establishingmechanisms for receiving and addressingcomplaints of those negatively affected by reliefwork. In Haiti, the U.N., which is responsible forMINUSTAH’s operations, has refused to institutesuch a mechanism.44the u.n.’s actions violated principles and standards of humanitarian relief
A. Humanitarian Organizations HaveDeveloped Principles and Standardsof Aid, Which U.N. Agencies HavePromoted, to Address the UnintendedHarms That Often Arise fromRelief Work.Humanitarian relief principles address theobligations of organizations delivering aid inconflict and emergency settings. These principlesstem from over a century of experience on the partof humanitarian actors in conflict settings andin complex humanitarian emergencies. Since thelate 19th century, independent but authoritativeorganizations like the ICRC have articulated thesehumanitarian principles, many of which havebeen codified in international law. These principleslimit how combatants may fight in war and governthe treatment of civilians, including requiringrespect for their health and security needs. Duringthe latter half of the 20th century, this focus onhumanitarian principles expanded to encompassthe obligations of relief organizations working inconflict and emergency situations. 274Humanitarian NGOs increasingly have soughtto develop frameworks that address both thecauses of unintended harmful consequences ofrelief and the lack of accountability humanitarianorganizations otherwise have to populationsreceiving assistance. 275 These frameworks not onlyestablish a broad principle of do no harm; they alsoprescribe a standard of professionalism againstwhich actions causing harm can be measured.Humanitarian actors are not responsible for everyharm caused by their presence; rather, they areaccountable only when their actions fall belowan accepted standard of professionalism. Finally,these principles hold accountability as a coreprinciple, and some set up specific processes toensure such accountability.Three humanitarian aid frameworks havebeen particularly influential: the ICRC Code ofConduct, the Sphere Project Humanitarian Charterand Minimum Standards, and the Humanitarian<strong>Accountability</strong> Partnership (HAP) Standard. TheICRC Code, Sphere Standards, and HAP Standardplay an important regulatory role in the field ofhumanitarian relief work. All three frameworksshare a common humanitarian goal of respectinghuman dignity 276 , which in turn entails acommitment to the do no harm principle and toimprovement in the quality of aid delivered. 277All three frameworks also reflect the belief thatproviding humanitarian relief requires meetingcertain minimum criteria of acceptable aid. Anumber of other humanitarian actors, includingU.N. agencies, have adopted and promoted the dono harm and accountability principles underlyingall three frameworks. 278The ICRC Code of Conduct is one of the firstcodifications by the international communityof humanitarian principles of relief response. 279Published in 1994, the ICRC Code is one partof a long history concerning the role of nongovernmentalactors in conflict and emergencysettings. This history dates back to at least as earlyas the ICRC’s founding in 1863 and is informedby over a century of successes and shortcomingsin humanitarian relief efforts. 280 The ICRC Codelays out broad principles of responsibility fororganizations delivering aid. Among these arean obligation to protect local populations—orat minimum, to do no harm to them—anda commitment to establish mechanisms ofaccountability for these populations. 281 Despitedebates about the effectiveness of the ICRCCode, today over 500 non-governmental relieforganizations are signatories to the ICRC Code andagree to abide by these principles. 282The principles articulated in the ICRCCode of Conduct are foundational to standardsof humanitarian aid developed by the SphereProject. 283 In 1996, a loose coalition of humanitarianNGOs, funders, and other actors, including theICRC, sought to develop minimum standardsof aid delivery from more general principles ofhumanitarian relief response. These actors weremotivated in part by the perceived failures of thehumanitarian NGO community in the Rwandangenocide and the Great Lakes refugee crisis of theearly 1990s. 284 In 1996, key humanitarian actorsbegan wide-ranging consultations with otherNGOs and international organizations, includingU.N. agencies, and ultimately created the SphereProject. 285The Sphere Project generated the Sphere45the u.n.’s actions violated principles and standards of humanitarian relief
Humanitarian Charter and Minimum Standardsin Disaster Response, first published in 1999and revised in 2004. 286 The Sphere Standardsare informed by international humanitarianlaw, human rights law, and guidelines fromthe U.N., other international organizations,and humanitarian NGOs. 287 Additionally, theseprinciples explicitly incorporate the ICRC Codeof Conduct. 288 The principles, in turn, inform aseries of common minimum standards and sectorspecificminimum standards in the areas of (1)water supply, sanitation, and hygiene promotion;(2) food security and nutrition; and (3) shelter,settlement, and non-food items. Today, the SphereStandards are widely recognized as minimumrequirements for organizations working in conflictand disaster relief. 289Debates over the enforceability of the SphereStandards and the humanitarian community’sperceived failures in Rwanda also gave rise to theHumanitarian Ombudsman Project and the HAP. 290Initially conceived as a watchdog for humanitarianorganizations, the Ombudsman Project was recastas a self-regulatory body that would establishstandards for accountability among humanitarianrelief organizations and certify NGOs as compliantwith those standards. From this, the HAP wasformed in 2003. 291The HAP developed a set of principles ofaccountability that emphasize a commitmentto humanitarian standards and rights as well asthe participation of all stakeholders—includingpopulations receiving aid. 292 From these principles,the HAP Standard derives six benchmarks ofhumanitarian accountability that assess (1)the establishment of a humanitarian qualitymanagement system; (2) the availability of publicinformation to all stakeholders; (3) the ability of aidbeneficiaries to participate in program decisions;(4) the capacity of humanitarian relief staff toimplement a quality management system; (5) theestablishment of complaints-handling procedures;and (6) the establishment of a process for improvingthe internal accountability framework. 293The U.N. and its agencies have played animportant role in developing and promoting allthree frameworks of humanitarian relief response.First, as noted above, U.N. agencies were involvedin the consultations that led to the development ofboth the Sphere Standards and the HAP Standard. 294Second, U.N. bodies and agencies approvinglycite to the Sphere Standards in their own internalguidelines and handbooks. The Office of the U.N.High Commissioner for Refugees Handbook forEmergencies, for instance, repeatedly cites theSphere Standards as a key reference in sectionsrelated to water, sanitation and hygiene, andhealth. 295 Similarly, World Health Organizationguidelines on solid waste management and excretadisposal in emergency settings also reference theSphere Standards. 296 Third, the U.N. Secretariathas promoted principles of accountability and dono harm through its Office for the Coordinationof Humanitarian Affairs. The Office for theCoordination of Humanitarian Affairs’ 2005Humanitarian Response Review, for instance,evaluated the international humanitarianresponses of NGOs and U.N. agencies in light ofhow accountable these organizations were to thepopulations they served. 297The ICRC Code, Sphere Standards, and the HAPStandard are critical to regulating humanitarianactors: Although humanitarian actors fulfill statelikefunctions in the basic services they provide,they are not subject to the same legal frameworks,that regulate states. As a result, humanitarianactors may face little or no consequences forinflicting great harm on the people they aim tohelp when delivering aid. Humanitarian reliefprinciples and standards bridge that gap.B. MINUSTAH’s Role in the CholeraOutbreak Should Be Evaluated byPrinciples Governing HumanitarianRelief.To the extent that the U.N. and MINUSTAH areconcerned with delivering quality humanitarianassistance and respecting the dignity of populationsreceiving aid, principles and standards ofhumanitarian relief are useful and appropriatetools for evaluating MINUSTAH’s role in thecholera outbreak. While U.N. missions are notformally bound to these frameworks, U.N. actorshave supported their development and consideredthese principles applicable to their own activities.46the u.n.’s actions violated principles and standards of humanitarian relief
Moreover, U.N. missions generally—and MINUSTAHspecifically—actively participate in humanitarianrelief work. 298 Furthermore, as is evident fromthe cholera outbreak, MINUSTAH operations canperpetrate the very harms humanitarian principlesand standards aim to prevent.MINUSTAH functions, in part, as ahumanitarian relief organization. U.N.Security Council Resolution 1542 establishedMINUSTAH and explicitly laid out obligationsfor the peacekeeping troops encompassing bothpeacekeeping and humanitarian activity. 299According to the resolution, MINUSTAH “shallcooperate with the Transitional Government [ofHaiti] as well as with their international partners,in order to facilitate the provision and coordinationof humanitarian assistance.” 300 Additionally, afterthe January 2010 earthquake, Security CouncilResolutions 1908 and 1927 explicitly tasked troopswith assisting in post-disaster relief efforts. 301MINUSTAH troops played a key role in theimmediate response to the earthquake, as wellas the longer-term humanitarian effort. 302 Untilthe beginning of the cholera outbreak, troopsperformed essential humanitarian functionsincluding clearing debris, distributing food, andrebuilding local infrastructure. 303Given MINUSTAH’s role in providinghumanitarian relief in Haiti, the mission issusceptible to harming the populations theyintend to help in ways that trigger concerns ofhumanitarian accountability. In the aftermath ofthe Haitian earthquake, MINUSTAH performedhumanitarian functions for extremely vulnerablepopulations. MINUSTAH was charged withworking with particularly vulnerable populations,such as displaced persons. 304 More generally,however, MINUSTAH was working in a countryrecently devastated by an unprecedentedearthquake and lacking in basic water, sanitation,and health infrastructure, rendering its citizensespecially vulnerable. 305 Additionally, when troopsfrom various countries with diverse exposure risksto contagious diseases enter a vulnerable countrylike Haiti, inadequate control of sanitation for thesetroops poses serious dangers. The introduction ofa foreign disease into a country with a weakenedhealth, water, and waste infrastructure system ledto devastating consequences for precisely thosepeople MINUSTAH was established to aid. Thehumanitarian role MINUSTAH played in postearthquakeHaiti, coupled with its introductionof cholera into the country, counsels in favor ofapplying principles of humanitarian relief toevaluate MINUSTAH’s harmful actions in Haiti anddevelop remedies to address them.C. MINUSTAH’s Actions in Haiti ViolatedTwo Fundamental Principles ofHumanitarian Aid and Fell BelowProfessional Standards of Relief.1. MINUSTAH’s Failure to Follow MinimumGuidelines of Adequate Sanitation at Its Campin Méyè Violated the Do No Harm Principle.MINUSTAH’s introduction of cholera into Haitiviolated the do no harm principle of humanitarianintervention. The do no harm principle includesan obligation to not expose individuals to physicalhazards, violence, or other rights abuse, includingdisease. 306 MINUSTAH violated this principle byintroducing an epidemic disease into a majorwaterway used by a vulnerable population, leadingto severe illness and death for many Haitians.MINUSTAH’s failure to observe minimumsanitation standards at the base in Méyè violatedthe do no harm principle. The Sphere Standardsspecify widely observed minimum guidelinesfor the management of excreta disposal inhumanitarian emergencies. These guidelinesaim to reduce disease transmission from humanwaste. 307 To this end, the Sphere Standardsemphasize the need to keep defecation systems ata safe distance from water sources. 308 U.N. agencieshave already recognized the importance of basicsanitation standards like those outlined in theSphere Standards, as U.N. specialized agencies havedeveloped similar standards for excreta disposalin emergency situations that also emphasize theseparation of human waste from water sources. 309Although these standards are generally designedfor excreta facilities for populations receiving aid,rather than aid workers or peacekeeping troops,the cholera epidemic in Haiti demonstrates thatif the goal of the standards is to do no harm, they47the u.n.’s actions violated principles and standards of humanitarian relief
must be observed in facilities for aid workers andpeacekeeping troops as well.Despite the U.N.’s awareness of these minimumguidelines and its role in developing and promotingthem, MINUSTAH did not observe proper excretadisposal at the camp in Méyè. As the U.N.Independent Panel of Experts noted, the base’s waterand waste pipes were haphazardly constructed. Thisled to “significant potential for cross-contaminationthrough leakage from broken pipes and poor pipeconnections.” 310 The report also observed how easilythe waterway near the MINUSTAH camp wascontaminated due to “an open drainage ditch thatr[an] throughout the camp and flow[ed] directly intothe Méyè Tributary System.” 311 Moreover, the campwas known to flood regularly, 312 leading to an evengreater likelihood of waste contaminating the watersupply. In failing to ensure that its camp followedthe most basic of sanitation guidelines and creatinga significant possibility of water contamination,MINUSTAH violated the do no harm principleand thus failed to meet professional standards ofhumanitarian relief.2. MINUSTAH Violated the Principle of<strong>Accountability</strong> to Affected Populations byFailing to Address the Claims of Victims of theCholera Epidemic.In failing to respond adequately to the claims forrelief of the many cholera victims, MINUSTAHhas not only violated legal responsibilitiesunder international law, but also the principleof accountability to populations receivingaid. 313 Broadly defined, accountability is howhumanitarian organizations answer to differentstakeholders. 314 Traditionally, humanitarianorganizations have answered mainly to donors, 315but organizations increasingly have recognized aneed to answer directly to the people affected byaid as well. 316Humanitarian organizations have voiced tworationales for holding themselves accountableto populations receiving aid. The first is moral:People receiving aid possess intrinsic humandignity, 317 and respect for human dignity requiresthat aid recipients be treated as active agentsin the humanitarian aid process rather thanas passive subjects. This, in turn, requires themeaningful participation of local populations inthe humanitarian aid process and mechanismsfor holding the humanitarian actor accountableto local populations in case of harm. 318 Thesecond rationale is practical: Feedback fromthose receiving aid is instrumentally valuable.Populations receiving aid are often more attuned tothe unintended harms of a particular interventionbecause they suffer the consequences of suchharm. Acknowledging a local population’sperspective on the relief it receives allowshumanitarian aid organizations to better tailortheir practices to community need, avoid coursesof action that may cause harm, and improve theirdelivery of aid. Thus, when local populationsparticipate in the humanitarian aid process,they can hold aid organizations accountable fortheir activities, leading to better, more effectivehumanitarian programming. 319As previously outlined in Chapters III andIV, MINUSTAH has refused to offer any remedyto the people it has harmed by bringing cholerato Haiti, and thus has violated—and continues toviolate—the accountability standards observedby most humanitarian agencies. MINUSTAHhas no effective complaints procedure available,and the U.N. has not established any otheravenue of redress, compensation, or reparationsfor the cholera victims in Haiti. 320 This failureto act not only violates the U.N.’s obligationsunder international law; it also falls short of thebasic principles and standards of humanitarianaid observed throughout the internationalhumanitarian aid community. MINUSTAH andthe U.N. thus have failed to meet the standardof accountability required of all organizationspurporting to deliver humanitarian relief.48the u.n.’s actions violated principles and standards of humanitarian relief
ConclusionThe U.N., through MINUSTAH, has provided much-needed humanitarianassistance in Haiti and, in so doing, is subject to those standards of internationalhumanitarian aid that the international relief community has agreed must guideall humanitarian intervention. By causing a cholera epidemic in a still-developingcountry, harming the people it has promised to help, and then denying those it hasharmed any redress for their injuries, the U.N. has violated fundamental principlesof humanitarian relief. The following chapter outlines how the U.N. can be heldto account for the totality of its failures under its SOFA with Haiti, internationalhuman rights law, and humanitarian principles and standards.49the u.n.’s actions violated principles and standards of humanitarian relief
Chapter VIRemedies andRecommendations50 section
Chapter VIRemedies and RecommendationsAs the previous chapters establish, MINUSTAHtroops introduced the V. cholerae bacteriuminto the Méyè Tributary, causing the largestcholera outbreak in Haiti’s history. Because ofits responsibility for the outbreak, the U.N. isresponsible for providing redress to the victims.This chapter outlines the steps the U.N. musttake, in light of that accountability, to remedy theharms it has caused in Haiti. What follows is nota comprehensive program for fighting cholera;rather, it is a framework of the minimum stepsthe U.N. must take to fulfill its contractual, legal,and moral obligations to the people it has harmedin Haiti, as explained previously in this report.Other entities, starting with the Government ofHaiti and including NGOs, foreign governments,and other intergovernmental actors, are alsokey to remediating the cholera epidemic. Theseactors must help provide direct aid to victims,infrastructural support, and adequate fundingfor the prevention and treatment of cholera.Ultimately, the Government of Haiti must be ableto ensure the health and rights of persons withinits borders. This chapter, however, focuses on theU.N.’s obligations to the victims of the choleraepidemic in Haiti because the U.N. is uniquelyaccountable for the epidemic.To fully accept its responsibility, the U.N.must vindicate the legal rights of the victims,guarantee adequate treatment for those sickened,stop the cholera epidemic, and, finally, ensure thata similar tragedy does not reoccur—either in Haitior anywhere else the U.N. sends its peacekeepingtroops or other agents. The U.N. must first providevictims with the legal recourse to which they areentitled under international law. Given the scopeof U.N. immunity in domestic courts, this recourseshould take the form of the claims commissionoutlined in and required by the SOFA. Second, theU.N. must respond to the continuing cholera crisis,most crucially by funding the plan that the MSPPand PAHO, itself a specialized agency of the U.N.,have developed. Finally, the U.N. must ensure thata similar wrong never again happens by reformingits peacekeeping procedures, particularly thoserelated to waste disposal and disease transmission,enforcing the SOFA’s requirement that a standingclaims commission be set up for all missions,and taking all necessary steps to meet its dutyto guarantee non-repetition of such harms. Thefollowing remedies are not simply charitableresponses to a humanitarian crisis; they are whatthe U.N. must do to fulfill its basic contractual,legal, and moral duties.A. Vindicating the Rights of VictimsAs this report has explained, by failing to provideany meaningful forum for victims of the choleraepidemic to seek redress, the U.N. violates itsown SOFA, human rights law, and principlesof humanitarian intervention. To remedy thisfailure, the U.N. must establish a forum in whichthe victims’ claims to relief can be heard. Thisforum could be a court of law—the U.N. couldwaive its immunity in most courts and providevictims with the right to sue under domesticand international law. Alternatively, the SOFAprovides for such a forum in the form of a claimscommission. Because the SOFA specificallycontemplates the establishment of a claimscommission for circumstances such as these, thissection focuses on how to create a commissionand provides suggestions, taken from examples ofsuccessful, large-scale claims processing bodies,for its structure and operation. The U.N. claimscommission, if established, need not be structuredexactly like these examples. Rather, the discussionof these precedents is instead intended to illustratethat creating an efficient, effective commission,even with large numbers of claimants and difficultissues of adjudication, is possible.1. A U.N. Claims CommissionThe SOFA requires that the U.N. establish astanding claims commission to hear claims of aprivate law nature like those of the victims of the51 remedies and recommendations
cholera epidemic. Thus far, despite the efforts of thevictims and their advocates, 321 the U.N. has failedto create a commission and has instead declinedany consideration of their claims by invoking theGeneral Convention.The SOFA outlines the necessary structure ofsuch a commission, requiring that it include threemembers: one appointed by the U.N., one appointedby the Government of Haiti, and a chairman jointlyappointed by both parties. 322 Thus, as a first step,either the Secretary-General or the Government ofHaiti must appoint an initial commissioner. Then,both parties can choose a chairman, or one partycan appeal to the president of the ICJ to appointthe chairman. 323 In practice, this means that theGovernment of Haiti or the Secretary-General mustappoint a commissioner to establish a commissionthat can receive the victims’ claims.The SOFA does not specify procedures thecommission should use to adjudicate claims, leavingthat decision to the commissioners. However, twohistorical instances of successful claims processingbodies—the U.N.’s own post-Gulf War compensationcommission and the United States’ post-September11 compensation fund—provide a useful guide forthe U.N. commission. These commissions set upprocedures for processing claims that were, in manyways, more difficult to adjudicate than the choleravictims’ claims.2. Historical Precedent—from the United NationsCompensation Commission to the September 11Victims Compensation Funda. The United Nations Compensation Commission(UNCC) in IraqIn the aftermath of the First Gulf War in Iraq,the U.N. set up the United Nations CompensationCommission (UNCC). The UNCC demonstratesthat the U.N. is logistically capable of establishingclaims commissions. Unlike the claimscommission proposed for cholera victims in Haiti,the UNCC was unrelated to U.N. culpability. Rather,the UNCC was designed to compensate victims ofthe Iraqi invasion and occupation of Kuwai, andfunctioned as a special organ of the U.N. that heldfunds and determined how to allocate them. 324 Thesize and scope of the UNCC were unprecedented,and in the absence of prior commissions to providea framework for adjudication, the commissionadapted procedures and structures frominternational arbitration and past post-war claimscommissions to the larger scale and differentsubject matter of the UNCC. 325The UNCC processed claims from its inceptionin 1991 until 2005, and completed compensationof victims in 2007. By 1996, the UNCC had alreadydistributed over $4 billion to claimants, dividedamong over 980,000 awards. 326 After 1996, thepace of claims processing increased, and by2007, the UNCC had paid $54.2 billion to settleover 1.5 million claims. 327 These payments weremade for a broad range of harms attributed tothe Iraqi invasion of Kuwait, including businesslosses, real and personal property losses, andpersonal injuries. 328 Payments were also made togovernments and NGOs for evacuation costs andother incidental costs of the invasion. 329 Iraq wasresponsible for paying the commission’s awards. 330The commission issued comparatively fewawards for serious bodily injury or death due tofinancial limitations and the scale of war claims. 331This highlights the critical difference betweenthe UNCC and a claims commission for thecholera epidemic in Haiti: The UNCC addresseda wide range of claims arising from war, not themore limited claims resulting from an outbreakof disease. The UNCC, however, reveals that theU.N. can successfully adapt existing proceduresand apply them to a complicated set of claimsin a newly established claims commission.Furthermore, the UNCC belies potential objectionsthat a cholera claims commission would takegenerations to complete its work, as the UNCCconcluded a much more expensive and widerangingclaims process within 14 years. 332 The factthat the UNCC compensation was paid by Iraq,of course, meaningfully distinguishes it fromthe U.N. itself compensating the victims of theepidemic in Haiti, but the source of compensationis an issue distinct from the U.N.’s proven ability toadminister a claims commission.52remedies and recommendations
. The September 11th Victims CompensationFund (VCF)Similarly, the well-regarded claims processestablished after the September 11 terrorist attacksoffers a model for how the U.N. could establishworkable standards for assessing claims in a claimscommission for victims of the cholera epidemic.Eleven days after the attacks, Congress establishedthe September 11 Victim Compensation Fund(VCF),“to provide compensation to any individual(or relatives of a deceased individual) who wasphysically injured or killed as a result of theterrorist-related aircraft crashes of September 11,2001.” 333 In total, the commission awarded over $7billion to 2,680 victims of physical injury and thesurvivors of 2,880 people who died in the attacks. 334Upon filing a claim, victims waived their rights tomost litigation arising out of September 11. 335 TheVCF was non-adversarial; the procedures did notinvolve a finding of fault regarding any party andaward computation did not depend on any suchfinding. 336 Kenneth Feinberg, the commission’sspecial master, called it “an unprecedentedexpression of empathy from the American peopletoward their fellow citizens and others who theterrorist attacks victimized.” 337A U.N. claims commission for the choleraepidemic should not be merely “an expressionof empathy” but a forum in which a wrongdoercan compensate its victims. However, a nonadversarialprocess that does not include findingsof fault might prove more politically feasible for aU.N. commission.Although the substance of the claims resolvedby VCF is distinct from those of a U.N. claimscommission for Haitian cholera victims, thestructure of the VCF is illuminating. The VCF’smethodology for determining compensationdemonstrates that consistent, pre-set formulasfor calculating awards can lead to highly efficientclaims processing. Pursuant to Congressionalauthorization, the VCF created a “presumedmethodology” for calculating an award. 338 Thepresumed methodology used the victim’s age,income, and number of dependents for thecomputation. While the income variable wouldneed to be tailored to the Haitian context, ageand number of dependents would be reasonableprima facie variables for the award calculationmethodology in a U.N. claims commission for thecholera epidemic. Furthermore, a compensationmethodology that is formula-driven, allowing forfairness and efficiency in calculation while stilltailoring awards to individual circumstances,would afford victims of the cholera epidemic ameasure of justice that U.N. immunity otherwisedenies them.B. Addressing the Public Health CrisisJust as the U.N.’s actions require it to provide legalredress for the victims of the cholera epidemic,the U.N. also must address the ongoing healthcrisis that the introduction of cholera has createdin Haiti. However, unlike its vindication of legalrights through a claims commission, the U.N. willnot, for the most part, provide direct public healthrelief. The Government of Haiti, PAHO, the CDC,and NGOs are the key providers of treatment in theongoing epidemic; the U.N.—by virtue of havingcaused the epidemic—bears the responsibilityfor ensuring the adequacy of the public healthresponse to the outbreak. Most critically, thisresponsibility requires the U.N. to ensure thatboth immediate treatment intervention and theMSPP Plan for the long-term elimination of choleraare fully funded. The U.N. and MINUSTAH mustalso provide any technical and logistical supportneeded by the key public health actors treatingcholera in Haiti.1. Immediate InterventionCholera is an ongoing health crisis in Haiti. Witheach rainy season, the Government of Haitiand international aid organizations struggle toprevent another surge in mortality. 339 As a result,preventing the spread of disease and treatingthose currently infected is a constant and urgentneed. The U.N. can best realize its responsibilityto the people in Haiti it has harmed by ensuringthat emergency efforts to treat and prevent theepidemic are properly funded.Currently, immediate intervention suffers fromsparse funding and supplies. The NGO Partners inHealth has observed nearly twice the number of53remedies and recommendations
cholera patients in its clinics this year comparedto 2012, in part due to a decrease in choleratreatment and prevention funding that has led tothe withdrawal of many other international NGOsfrom Haiti. 340 As NGOs—and their funding—leavethe country, standards of care decline. Treatmentcenters face dwindling supplies, inadequate staff,and worn-out equipment, all of which causemortality to increase. 341 Both the Government ofHaiti and non-government actors must ensurethat hospitals and CTCs are properly supplied andadequately staffed to effectively control the disease.This can be done by providing adequate funding fortreatment and prevention, creating a more efficientchain for distributing supplies, training morecommunity health workers, and promoting properhygiene and sanitation within communities.Proper surveillance systems to track diseaseoccurrence must also be maintained to helpprevent the further spread of cholera. A February2013 study detailing the implementation of theNational Cholera Surveillance System after theinitial outbreak of cholera in 2010 illustrated theeffectiveness of such surveillance measures. 342 Thestudy provided a two-year summary of data for theepidemic through October 20, 2012, and concludedthat the MSPP, by overseeing the collection andreporting of cholera-related data, established animportant precedent for a national surveillancesystem that, if continuously well-funded andproperly implemented, will effectively monitorboth cholera incidence and the impact of publichealth efforts to reduce morbidity and mortality.2. Cholera Elimination—The MSPP Plana. The Structure of the MSPP PlanThe MSPP Plan, announced in November 2012 asa comprehensive program to eliminate cholera inHaiti and the Dominican Republic, is divided intothree phases, each of which includes a target forreducing the incidence rate of cholera. First, bycontinuing the emergency measures discussedabove in Section B.1 and accelerating long-termhealth and sanitation projects, the incidence rateshould fall from 3% of the population to below0.5% by 2014. Second, by chlorinating public watersupplies and otherwise improving water andsanitation systems to the level found in other LatinAmerican and Caribbean countries, the cholerarate should fall to less than 0.1% by 2017. Finally,by dramatically increasing potable water accessand Haiti’s rates of proper sanitation and humanwaste disposal, the cholera rate should fall to lessthan .01% by 2022. The following chart outlines keydetails of each phase:Phase # and DateMetric of Success(as measured by cholera rate)Plan Details / Additional GoalsPhase 1—end of 2014Fall to at least .5%• Continue emergency cholera management until 2015.• Increase hand-washing after defecation and prior toeating in areas of Haiti where there is active transmission.• Strengthen and expand primary health care systems.• Provide simple safe-water technologies in high-risk areas.• Construct excreta disposal facilities in high-risk areas andimprove the cleaning of existing latrine pits. 34354
Phase 2—end of 2017Fall to at least .1%• Chlorinate and regularly monitor all public watersupply systems.• All national research laboratories should be functionaland gathering data.• The water and sanitation sector should be strengthenedto be comparable to those of the Latin American andCaribbean countries.• Increase efficacy and reach of primary care.• Strengthen role of the Haitian National Directorate forWater Supply and Sanitation (DINEPA) in maintenance ofsanitation and hygiene. 344Phase 3—end of 2022Fall to at least .01%• Increase access to potable water and sanitation to at leastthe average level of the countries in Latin America and theCaribbean.• Specifically, rates of access to potable water should movefrom the current 69% to 85%.• Access to adequate sanitation should sharply increasefrom the current 17% to 80%.• Risk of cross-contamination of feces and water willbe reduced as a result of the proper disposal ofhuman waste.b. Funding and implementation challengesAs the actor responsible for the cholera outbreak,the U.N. must ensure full funding of the MSPPPlan. The plan is estimated to cost approximately$2.27 billion over its ten-year span. However, todate, U.N. members have pledged only 1% of thetotal cost. 345 Security Council members shouldtake the lead in fundraising, particularly fromthose more developed countries with the strongesthistorical ties to Haiti—the United States, Canada,and France. These countries should also bothappropriate money themselves for the MSPP Planand fundraise with the U.N., doing everythingnecessary to encourage other member states todonate to ensure full funding. 346In implementing the MSPP Plan, it iscritical that international organizations areavailable to provide the technical expertise,fundraising, and lobbying necessary for theplan’s success. In particular, the CDC and PAHO/WHO have contributed to the development ofthe plan and pledged to continue to supportits implementation. 347 Inasmuch as theseorganizations and other intergovernmentalorganizations can, they should provide directbudgetary support for the MSPP Plan. They shouldalso lobby states to contribute to the plan.Finally, it is critical that the plan beimplemented by and for the communities in Haitithat the epidemic has most affected. Doing so willensure respect for the principle of accountabilityfor humanitarian aid discussed in Chapter V. Tothat end, Haitian community groups must be givenformal channels to provide input and oversight toMSPP decisionmakers. Local input is not simplyan abstract principle of development work: TheMSPP plan recommends a number of changes tosanitation practices in communities and homes,recommendations that will require changingcultural practices and ensuring sufficient knowledgeand experience of these practices to be successful. 34855remedies and recommendations
C. Dignitary JusticeThe U.N. must work to re-establish its institutionallegitimacy in Haiti. The role of the U.N. andMINUSTAH in causing the epidemic has createddeep anger among the general public in Haiti, andthe U.N.’s refusal to take any responsibility for itsactions has eroded its already fragile reputationin the country. Indeed, many have questionedMINUSTAH’s continued presence in Haiti aftercausing the epidemic.An apology by the U.N. is an essential steptoward repairing its legitimacy deficit in Haiti.Alhough MINUSTAH’s presence in Haiti wascontroversial long before the cholera epidemicbegan, 349 an apology for the cholera epidemic neednot resolve controversies about the MINUSTAHmission in its entirety. Rather, an apology wouldaddress the discrete wrong committed by the U.N.in bringing cholera to Haiti. In a report to theU.N. Human Rights Commission, Michel Forst,the U.N.’s own independent expert on humanrights in Haiti, recognized that the U.N.’s refusalto acknowledge its responsibility for the epidemicis negatively affecting the legitimacy of theorganization. According to Forst, “[S]ilence is theworst response.” 350In conjunction with the other remediesoutlined in this section, an apology is a crucialopportunity to begin repairing MINUSTAH’srelationship with the people they have harmed,the same people with whom they must live andwork as long as the mission remains in Haiti. AsChapter II illustrates, scientific consensus has longago made the U.N.’s current denial of responsibilityfor the outbreak untenable. Thus, a public apologywill not reveal anything not already publiclyknown. Given widespread knowledge of the U.N.’smalfeasance in Haiti, every simple, terse denialof responsibility it makes further diminishes itsalready weakened credibility. An apology offers theU.N. a virtually cost-free means of beginning torebuild this diminished credibility. Furthermore,to the extent that the U.N.’s current refusal topublicly take responsibility and apologize for theepidemic is designed to avoid providing victimscompensation, such avoidance will be unnecessaryonce the claims commission is established. Apublic apology would be complementary to theclaims commission’s work.Finally, the U.N. should leave its currentoutpost at Méyè and relocate. The MINUSTAHbase that introduced cholera into the ArtiboniteRiver remains within a few miles of the homesof families devastated by cholera. AlthoughMINUSTAH has rotated the Nepalese soldiers whointroduced the disease out of the mission in Haiti,the camp that they inhabited still stands. Victimsof the cholera epidemic have expressed anger athaving to walk by the MINUSTAH camp in Méyè. 351The continued presence of the base serves as apainful reminder of both the U.N.’s role in causingthe epidemic and its denial of responsibility fordoing so. After vacating MINUSTAH from the base,the U.N. should offer it to the community for useas a medical center or as a location for a victims’memorial.D. Looking toward the Future1. A Guarantee of Non-RepetitionAs discussed in Chapter IV, the guarantee ofnon-repetition is a critical component of redressunder international human rights law for certainhuman rights violations. The human rightsviolator must guarantee—and take sufficientprophylactic measures to ensure—that it will makeall necessary changes to ensure that it commits nosimilar human rights violation in the future. 352A guarantee of non-repetition cannot simplybe a general commitment to not repeat thewrongdoing. Rather, the offending party mustshow specific steps it plans to take that willprevent repetition of the violation. Guarantees ofnon-repetition have been made recently, includingby the U.N., in the form of allowing for civiliancontrol of security forces to redress Turkishviolations against Kurds living in Turkey 353 andensuring that victims, including women, are givenan opportunity to testify about state abuses againstthem during the Arab Spring to redress violationsby the former government in Tunisia. 354The cholera epidemic in Haiti presents anexceptional circumstance, as defined in theLaGrand case discussed in Chapter IV, requiring a56remedies and recommendations
guarantee of non-repetition. As with the lawlessexecution in that case, there is no prospectiverelief that will fully ameliorate the U.N.’s pastwrong of introducing cholera into Haiti. Moreover,the U.N.’s evasion of responsibility for doing soand denial of a remedy for its victims, as wellas the sheer magnitude of the injury caused,are exceptional. Finally, the U.N.’s oversight ofa number of peacekeeping missions around theworld presents the real possibility of a similarwrongdoing reoccurring. Following the ICJ’sinstruction in LaGrand, the U.N. must takes stepsto guarantee non-repetition to the victims of thecholera epidemic in Haiti.Insofar as poor supervision of peacekeepersallowed for the MINUSTAH camp to be builtwith inadequate sanitation infrastructure, theU.N.’s guarantee of non-repetition must includereform of MINUSTAH’s operational supervision.Furthermore, reforming the composition, funding,and supervision of peacekeeping missions will helpto ensure that MINUSTAH’s malfeasance is notrepeated in U.N. peacekeeping missions elsewhere.Similarly, the U.N.’s commitment to honoringthe SOFAs it signs with countries that receive itspeacekeepers and observing the limitations onits immunity under the General Convention maybe the most potent guarantees of non-repetitionavailable to the U.N.The U.N., per its letter refusing to acceptthe claims filed by approximately 5,000 choleravictims, maintains that it cannot be heldresponsible for its wrongdoing, regardless of theharms it inadvertently inflicts in the world’smost vulnerable countries. This position isnot only legally groundless; but it also distortsincentive structures guiding the U.N.’s behaviorby foreclosing external consequences for bad actscommitted by its officials. Guarantees of nonrepetitioncan correct this distortion. A guaranteeof formal, legal accountability is necessary toencourage future U.N. agents to take reasonablecare during peacekeeping missions in all of theiractivities, including managing waste disposal attheir encampments. By holding itself accountableto those it injures, the U.N. and its peacekeeperswill be less likely to harm people in the future.2. <strong>Peacekeeping</strong> Reforms to Guarantee Screeningand SanitationAs outlined in Chapter V, the U.N.’s creation of thecholera epidemic in Haiti has violated principles ofhumanitarian relief. The epidemic demonstratesthat the U.N. and its peacekeeping missions mustfollow the do no harm principle. To abide by thisprinciple, it must ensure that U.N. peacekeepingcamps have adequate sanitation infrastructure,regardless of whether the peacekeepers are likelyto transmit any specific disease. To implementthis principle, the U.N. can either adopt the SphereStandards, which articulate globally acceptedprinciples of humanitarian relief, in its oversightof peacekeeping missions or follow its own set ofprinciples consistent with the Sphere Standards.Either way, the U.N. must actually ensure thatits peacekeepers observe the existing frameworkof international humanitarian aid to ensure thattheir interventions do not cause inadvertent andavoidable harm.3. Honoring the SOFA’s StandingClaims CommissionTo effectively balance the U.N.’s interest inits immunity from suit with principles ofaccountability consistent with its human rightsobligations, the U.N. must honor the SOFArequirement that it establish a standing claimscommission, as detailed in Chapter III, at the startof every peacekeeping mission it authorizes. Themodel SOFA currently in force calls for a standingcommission for every mission; given the numberof peacekeeping missions currently in operation,this requirement may be logistically challenging torealize and may partially explain why the U.N. hasnever set up a commission for any of its missions.A revision of the model SOFA may help ensurethat the U.N. upholds its obligation to hear claimsfrom those harmed by its peacekeeping missions.In future SOFAs, the U.N. could establish onestanding claims commission—with enoughseparation from U.N. Department of <strong>Peacekeeping</strong>Operations (DPKO) to ensure objectivity—tohear claims concerning all peacekeeping57remedies and recommendations
missions. Either type of commission would needsufficient funding to speedily adjudicate claims.Furthermore, the claims commission processwould need to be accessible to people injured inpeacekeeping missions. Thus, a single standingclaims commission may need a physical presencein locations where U.N. peacekeeping troopsare deployed.Either form of claims commission, establishedprior to any potentially wrongful conduct ratherthan afterwards, would promote fair and efficientprocessing of claims. Moreover, a true standingcommission would not only avoid the need to setup a claims commission after injuries occur, butwould also encourage the U.N. to take greater carewhen deploying of peacekeepers.58remedies and recommendations
Endnotes1 MINUSTAH is the French acronym for Missiondes Nations Unies pour la stabilisation enHaïti.2 The MINUSTAH website in French is here:http://www.minustah.org/. The website inEnglish is here: http://www.un.org/en/peacekeeping/missions/minustah/.3 Robert Muggah, The Effects of Stabilisation onHumanitarian Action in Haiti, 34 Disasters S444,S446 (2010).4 U.N. Secretary-General, Rep. of the SecretaryGeneral on Haiti, 8–16, U.N. Doc. S/2004/300(Apr. 16, 2004) [hereinafter U.N. 2004 Haiti Report];S.C. Res. 1542, U.N. Doc. S/RES/1542 (Apr.30, 2004).5 U.N. 2004 Haiti Report, supra note 4, 72.6 S.C. Res. 1542, supra note 4, 5.7 Permanent Mission of Canada to the U.N.,Canadian Policy Positions: Haiti (Jan. 2, 2013),available at http://www.canadainternational.gc.ca/prmny-mponu/canada_un-canada_onu/positions-orientations/regions/haiti.aspx-?lang=eng.8 See U.N. Dep’t for <strong>Peacekeeping</strong> Operations &Dep’t of Field Support, United Nations <strong>Peacekeeping</strong>Operations: Principles and Guidelines(2008), available at http://www.un.org/en/peacekeeping/operations/principles.shtml(noting the increasingly broad nature ofpeacekeeping mandates of U.N. missions).9 Todd Howland, <strong>Peacekeeping</strong> and Conformitywith Human Rights <strong>Law</strong>, 13 Int’l <strong>Peacekeeping</strong>462, 478–469 (2006) (noting that unlike manypeacekeeping operations, MINUSTAH wasestablished in the absence of a “hot war”and was not “supported by, or grounded in, apeace accord or even a peace process”). See alsoMatt Halling & Blaine Bookey, <strong>Peacekeeping</strong> inName Alone: <strong>Accountability</strong> for the United Nationsin Haiti, 31 Hastings Int’l & Comp. L. Rev. 461,463 (2008) (discussing the exceptionality ofthe MINUSTAH mission); Bri Kouri NouvèlGaye et al., Submission to the U.N. Human RightsCouncil Twelfth Session of the Working Group onthe Universal Periodic Review, Oct. 3-13, 2011,1-6 (arguing the MINUSTAH mandate isinappropriate under Chapter VII of the U.N.Charter) [hereinafter 2011 UPR Submission].10 U.N. 2004 Haiti Report, supra note 4, 8.11 Id.12 S.C. Res. 1542, supra note 4, 1; U.N. 2004 HaitiReport, supra note 4, 9.13 S.C. Res. 1542, supra note 4, 7.14 Id. 9.15 S.C. Res. 1608, U.N. Doc. S/RES/1608 (June 22,2005); S.C. Res. 1702, U.N. Doc. S/RES/1702 (Aug.15, 2006); S.C. Res. 1743, U.N. Doc. S/RES/1743(Feb. 15, 2007); S.C. Res. 1780, U.N. Doc. S/RES/1780 (Oct. 15, 2007); S.C. Res. 1840, U.N.Doc. S/RES/1840 (Oct. 14, 2008).16 U.N. 2004 Haiti Report, supra note 4, 72–75.17 Id. 73 (describing the overall missionstructure), 94 (describing the civilian affairscomponent), 101 (describing the humanitarianaffairs component), 105 (describing themilitary component).18 Howland, supra note 9, at 471.19 See, e.g., U.N. G.A., Rep. of the Advisory Committeeon Administrative and Budgetary Questions,U.N. Doc. A/67/780/Add.5, 67th Sess. (Apr. 29,2013). (documenting staffing changes at theMINUSTAH base).20 U.N. Secretary-General, Rep. of the SecretaryGeneral on the United Nations StabilizationMission in Haiti, 2–4, U.N. Doc. S/2010/200(Apr. 22, 2010) [hereinafter MINUSTAH Apr. 2010Report]; U.N. Secretary-General, Rep. of the SecretaryGeneral on the United Nations StabilizationMission in Haiti, U.N. Doc. S/2010/200/Corr.1(Apr. 27, 2010).21 S.C. Res. 1908, U.N. Doc. S/RES/1908 (Jan. 19,2010); S.C. Res. 1927, U.N. Doc. S/RES/1927 (June4, 2010).22 S.C. Res. 1927, supra note 21, prmbl.23 See U.N. Secretary-General, Rep. of the SecretaryGeneral on the United Nations StabilizationMission in Haiti, 44–50, U.N. Doc. S/2010/446(Sept. 1, 2010) [hereinafter MINUSTAH Sept.59 endnotes
2010 Report].24 MINUSTAH Apr. 2010 Report, supra note 20, 30;MINUSTAH Sept. 2010 Report, supra note 23, 14, 57.25 MINUSTAH Apr. 2010 Report, supra note 20, 42–43.26 Id.27 2011 UPR Submission, supra note 9, 16.28 See Athena Kolbe & Royce Hutson, HumanRights Abuses and Other Criminal Violationsin Port-au-Prince, Haiti: A Random Survey ofHouseholds, 368 Lancet 864 (2006) (documentinghuman rights violations in Port-au-Princebetween 2004 and 2006).29 2011 UPR Submission, supra note 9, 16.30 Human Rights Watch, Haiti Country Summary2012 4–5 (2012), available at http://www.hrw.org.31 2011 UPR Submission, supra note 9, 33.32 Id. 37.33 Centers for Disease Control and Prevention,Update: Cholera Outbreak–Haiti 2010, 59 Morbidityand Mortality Weekly Report 1473 (2010)[hereinafter CDC Update].34 Id. See also Deborah Jenson et al., Cholera inHaiti and Other Caribbean Regions, 19th Century,17 Emerging Infectious Diseases 2130 (2011)(explaining cholera had not been observed inHaiti in over a century).35 Renaud Piarroux et al., Understanding theCholera Epidemic, Haiti, 17 Emerging InfectiousDiseases 1163 (2011). The World HealthOrganization (WHO) defines cholera as acutewatery diarrhea, with or <strong>without</strong> vomiting,in a patient aged 5 years or more. As choleraspread across the country, the Haitian Ministryof Health (MSPP) implemented the NationalCholera Surveillance System. The Systemmodified the definition of cholera to includepersons of any age in a cholera-affected department.See Ezra J. Barzilay et al., CholeraSurveillance During the Haiti Epidemic—The First2 Years, 368 New Eng. J. Med. 599, 600 (2013).36 Id.37 Id.38 Barzilay, supra note 35, at 601.39 CDC Update, supra note 33, at 1473. On October28th, 2010, as part of the National CholeraSurveillance System, the health ministrydistributed standardized reporting forms andcase definitions to all Haitian administrativedepartments. By November 10th, 2010,the MSPP was receiving daily, standardizedreports from all ten departments. See Barzilay,supra note 35, at 601.40 CDC Update, supra note 33, at 1476.41 Id.42 Id. at 1477.43 Gov’t of Haiti, Ministry of Public Health andPopulation and National Directorate for WaterSupply and Sanitation, National Plan forthe Elimination of Cholera in Haiti 16 (2013)[hereinafter MSPP Plan]. See also Center forHuman Rights & Global Justice, NYU Sch. of<strong>Law</strong> et al., Wòch Nan Soley [Rocks in the Sun]:The Denial of the Right to Water in Haiti 15(2008), available at http://www.chrgj.org/projects/docs/wochnansoley.pdf[hereinafter TheDenial of the Right to Water in Haiti].44 Pan American Health Organization & WHO,Health in the Americas 397 (15th ed. 2012).An improved sanitation system is one wherehuman excreta are effectively separated fromhuman contact.45 MSPP Plan, supra note 43, at 17. In 2009 thenational government created the NationalDirectorate for Water Supply and Sanitation(DINEPA) to coordinate and regulate waterand sanitation service providers.46 Id. at 18.47 Id. at 21.48 Id. at 28.49 Edward T. Ryan, Haiti in the Context of the CurrentGlobal Pandemic, 17 Emerging InfectiousDiseases 2175 (2011) (comparing the Haitianepidemic to other current epidemics).50 Barzilay, supra note 35, at 606.51 Centers for Disease Control and Prevention,Cholera in Haiti: One Year Later (Oct. 25, 2011),available at http://www.cdc.gov/haiticholera/haiti_cholera.htm.52 Barzilay, supra note 35, at 599.53 U.N. Office for the Coordination of HumanitarianAssistance, Haiti: Cholera Snapshot (May6, 2013), http://www.unocha.org/where-wework/haiti.60endnotes
54 Barzilay, supra note 35, at 607.55 Patrick Adams, Cholera in Haiti Takes a Turn Forthe Worse, 381 Lancet 1264 (2013).56 Id.57 MSPP Plan, supra note 43, at 39.58 Jenson, supra note 34, at 2131. This evidence isfurther discussed in Chapter II. Most studieshave identified MINUSTAH peacekeepingtroops as the source of the outbreak. There aretwo notable exceptions: First, the expert U.N.report on cholera found that the evidence wasinsufficient to determine a single cause of theepidemic. Second, a study published by Hasanet al. suggested that there may have beenadditional sources of cholera in the environment.Both of these studies have been challenged.59 Hasan et al. have claimed there were strainsof asymptomatic cholera already present inHaiti before the arrival of the Nepalese troops.However, there is no evidence these strainscaused cholera symptoms in patients. For afuller discussion of this, see Chapter II.60 Jenson, supra note 34, at 2131. The 1833 outbreakoccurred in Cuba. The 1850 outbreakaffected Jamaica, Cuba, Puerto Rico, St.Thomas, St. Lucia, St. Kitts, Nevis, Trinidad,the Bahamas, St. Vincent, Granada, Anguilla,St. John, Tortola, the Turks and Caicos, theGrenadines, and possible Antigua. The 1865outbreak hit Guadeloupe, Cuba, St. Thomas,the Dominican Republic, Dominica, Martinique,and Marie Galante.61 Id. at 2133.62 Id. at 2130–2131.63 CDC Update, supra note 33, at 1473.64 Id.65 Piarroux, supra note 35, at 1162–1163.66 Alejandro Cravioto et al., Final Report of theIndependent Panel of Experts on the CholeraOutbreak in Haiti 12 (2011), available at http://www.un.org/News/dh/infocus/haiti/UN-cholera-report-final.pdf.See also Piarroux, supranote 35, at 1162 (citing slightly different dates,October 9–16).67 Cravioto, supra note 66, at 12–13.68 Id.69 Id.at 22.70 Piarroux, supra note 35, at 1165.71 Is the UN repackaging Haiti’s cholera aid?, Al-Jazeera(Dec. 21, 2012, 1:22 PM), http://www.aljazeera.com/programmesinsidestoryamericas/2012/12/2012122113116245840.html(videoinvestigation citing earlier investigations byAl Jazeera).72 Chen-Shan Chin et al., The Origin of the HaitianCholera Outbreak, 364 New Eng. J. Med. 33(2011); Rene S. Hendriksen et al., PopulationGenetics of Vibrio Cholerae from Nepal in 2010, 2mBio 1 (2011); Anirban Dasgupta et al., EvolutionaryPerspective on the Origin of HaitianCholera Outbreak Strain, 30 Journal of BiomolecularStructural and Dynamics 338 (2012).This evidence is further discussed in ChapterII.73 See, e.g., Hendriksen, supra note 72, at 2–3.74 Id.75 Id.76 Cholera Strikes Haiti, MSF Alert Newsletter(Jan. 31, 2011).77 J.W. Tappero & R.V. Tauxe, Lessons Learnedduring Public Health Response to Cholera Epidemicin Haiti and the Dominican Republic, 17 EmergingInfectious Diseases 2087 (2013), available athttp://dx.doi.org/10.3201/eid1711.11082778 Id.79 MSPP Plan, supra note 43.80 UN launches new initiative to eliminate cholera inHaiti and Dominican Republic, U.N. News Centre(Dec. 11, 2012), available at http://www.un.org/apps/news/story.asp?NewsID=43743&Cr=cholera&Cr1=#.UN0IapPjnKB.81 Adams, supra note 55.82 For a summary of the arguments made byHaitian lawyers, see Jacceus Joseph, LaMinustah et Le Choléra (2012). For the SOFA,see Agreement Between the United Nationsand the Government of Haiti Concerning theStatus of the United Nations Operation in Haiti,July 9, 2004, 2271 U.N.T.S. 235 [hereinafterHaitian SOFA].83 Letter from Patricia O’Brien, U.N. Under-Secretary-Generalfor Legal Affairs, to Brian Concannon,Attorney for Haitian Cholera Victims(Dec. 21, 2011) (on file with Brian Concannon).(noting that as of May no standing claims61endnotes
commission has ever been established). Amore complete analysis of the obligationsunder the SOFA can be found in Chapter III.84 Letter from Newton Louis St. Juste et al., Attorneysfor Haitian Cholera Victims, to BrianConcannon, Attorney for the Haitian CholeraVictims (Dec. 21, 2011), available at http://www.touthaiti.com/touthaiti-actualites/2060-lettre-des-victimes-du-cholera-au-parlement-reclamant-l-implementation-de-l-accord-du-9-juillet-2009-avec-l-onu.85 Interview with Maître Jacceus Joseph inN.Y.C., N.Y. (Apr. 19th, 2013). Mr. Joseph is alawyer in Haiti and author of La Minustah etLe Cholera (2012).86 Denúncia à Commissão Interamericana de DireitosHumanos, Claim before the Inter AmericanCommission (Oct., 2011), available at http://www.brasilhaiti.com.87 Id. 10–11.88 Email from Professor Cristine Zanella, Attorneyfor Petitioners, to Authors (Jan. 17, 2013,13:05 EST) (on file with authors).89 Petition for Relief, MINUSTAH Claims Unit(Nov. 8, 2011), available at http://ijdh.org/archives/22916.U.N. missions have local reviewboards in the field that review third partyclaims for damages. U.N. Secretary General,Administrative and Budgetary Aspects of theFinancing of the United Nations <strong>Peacekeeping</strong> Operations:Financing of the United Nations <strong>Peacekeeping</strong>Operations: Rep. of the Secretary General, 20–37, U.N. Doc. A/51/389 (Sept. 20, 1996)[hereinafter Financing of the United NationsProtection Force].90 Petition for Relief, supra note 89, 36-37, 31-50, 105.91 Id. 102–114.92 Letter from Mario Joseph et al., Attorneys forPetitioners, to Patricia O’Brien, U.N.Under-Secretary-General for Legal Affairs(May 7, 2013).93 Letter from Patricia O’Brien, U.N. Under-Secretary-Generalfor Legal Affairs, to BrianConcannon, Attorney for the Haitian CholeraVictims (Feb. 21, 2013), available at http://opiniojuris.org/wp-content/uploads/LettertoMr.BrianConcannon.pdf.94 Id. at 2.95 Letter from Mario Joseph et al., supra note 92,at 3.96 Id.97 See, e.g., Deborah Sontag, Protest Closes NewCholera Treatment Center in Haiti, N.Y. Times(Oct. 27, 2010), available at http://www.nytimes.com/2010/10/28/world/americas/28haiti.html;Haiti: Protesters Stone U.N. Patrol,N.Y. Times (Nov. 18, 2010), available at http://www.nytimes.com/2010/11/19/world/americas/19briefs-Haiti.html;Randal C. Archibald,Haitians Train for a Future With a Military, N.Y.Times (Oct. 25, 2012), available at http://www.nytimes.com/2011/10/26/world/americas/president-michel-martelly-seeks-to-re-create-haitis-army.html?pagewanted=all;LouiseC. Ivers, Op-Ed., A Chance to Right a Wrong inHaiti, N.Y. Times (Feb. 22, 2013), available athttp://www.nytimes.com/2013/02/23/opinion/a-chance-to-right-a-wrong-in-haiti.html.98 Jenson, supra note 34.99 Id. at 2130.100 Id. at 2134.101 Id. at 2133.102 Id. at 2134.103 Cravioto, supra note 66.104 Id. at 13-14.105 Id. at 14.106 Piarroux, supra note 35.107 Cravioto, supra note 66, at 15.108 Cravioto, supra note 66, at 16.109 CDC Update, supra note 33. This same form ofdiagnosis is used in the report released by theU.N.’s Independent Panel of Experts. Cravioto,supra note 66, at 17.110 In children under five years old the two mostlikely causes of diarrhea in developing countriessuch as Haiti are Rotavirus and E. Coliinfections. Diarrheal Diseases: Factsheet No. 330,World Health Organization (Apr., 2013), http://www.who.int/mediacentre/factsheets/fs330/en/index.html.111 See CDC Update, supra note 33, at 1.112 See Piarroux, supra note 35; Jean Gaudart etal., Spatio-Temporal Dynamics of Cholera duringthe First Year of the Epidemic in Haiti, 7 PLOSNeglected Tropical Diseases 1 (2013) (mapping62endnotes
cholera cases from the start of the epidemicthrough December 2011).113 Piarroux, supra note 35, at 1162.114 Id. at 1163.115 Communes are geographical subdivisions ofthe administrative departments in Haiti.116 Piarroux, supra note 35, at 1164.117 Id. Cholera in Haiti spread spatiotemporally,with initial cases centered at the location ofthe outbreak’s explosive onset in Mirebalaisand the Artibonite Valley and later casesexpanding from that center to regions of thecountry bordering it. As discussed above, thefirst cases of the disease appeared in Méyè onOctober 14th, 2010. Shortly thereafter, fromOctober 16th-19th, cases were reported inMirebalais, just 2 kilometers north of Méyè.During October 20th-28th, the disease progressedthroughout communes in or nearthe delta of the Artibonite. The movement ofthe disease in the early days of the epidemicsuggests that the spread of cholera duringthis time period was closely linked to proximityto the Artibonite River. Cholera surfacedin the North-West Department of Haiti fromNovember 11th-29th, the West Department(where Port-au-Prince is located) from November14th-30th, and the North and North-EastDepartments from November 21st-30th. Id. at1165. The outbreak’s presence in these departmentshas been associated with the movementof individuals infected with the disease,including inhabitants of the Artibonite Deltawho fled to neighboring communes to escapeinfection, deficiencies in water, sanitation,and health care systems, and HurricaneTomas, which reached Haiti on November5th and caused rapid flooding in some areaswhere cholera had already surfaced. Guardart,supra note 112, at 5.118 Piarroux, supra note 35, at 1164.119 Cravioto, supra note 66, at 22.120 Id.121 Hendriksen, supra note 72.122 Cravioto, supra note 66, at 12-13.123 A.A. King et al., Inapparent Infections andCholera Dynamics, 454 Nature 877 (2008) (arguingthat “asymptomatic carrier[s]”—i.e.,people from cholera-endemic areas—shouldbe treated with caution because they have ahigher likelihood of being able to infect otherseven if they themselves show no symptomsof disease, and that scientific evidenceand modeling demonstrates that the cholerastrain driving the Haitian epidemic likelycame from Nepal even though none of theMINUSTAH troops themselves were visibly illwith cholera prior to their deployment).124 Cravioto, supra note 66, at 12.125 Id.126 The Nepalese Army’s Chief Medical Officer,Brig. Gen. Dr. Kishore Rana, stated that noneof the soldiers deployed as part of the MI-NUSTAH mission were tested for V. choleraeprior to entering Haiti. Haiti cholera outbreak:Nepal troops not tested, BBC News South Asia(Dec. 8, 2010, 10:48 P.M.), http://www.bbc.co.uk/news/world-south-asia-11949181. TheU.N. has not disclosed medical records for theNepalese troops.127 Toxigenic cholera strains are those thatproduce toxins that cause symptoms. Toxigenicserogroups O1 and O139 of V. choleraemay cause cholera epidemics or pandemics.Nontoxigenic strains within these serogroupsalso exist in the environment, and also somemay cause sporadic cases of disease. B. Panget al., Genetic Diversity of Toxigenic and NontoxigenicVibrio Cholera Serogroups O1 and O139Revealed by Array-Based Comparative GenomicHybridization, 189 J. of Bacteriology 4837 (2007).128 Cláudia T Codeço, Endemic and Epidemic Dynamicsof Cholera: The Role of the Aquatic Reservoir,1 BMC Infectious Diseases 1471 (2001).129 Cravioto, supra note 66, at 21. See also Piarroux,supra note 35, at 1162.130 Cravioto, supra note 66, at 21.131 Id.132 Id. at 22.133 Id.134 Id.135 Id.136 Daniele Lantagne et al., The Cholera Outbreakin Haiti: Where and how did it begin?, CurrentTopics in Microbiology & Immunology (May22, 2013); see also Mark Doyle, Haiti cholera63endnotes
epidemic caused by UN, say experts, BBC News(July 25, 2013, 11:01 PM), http://www.bbc.co.uk/news/world-latin-america-23460826;Colum Lynch, Cholera outbreak in Haiti tiedto U.N. peacekeepers, report says, Wash. Post(July 25, 2013), http://www.washingtonpost.com/world/national-security/cholera-outbreak-in-haiti-tied-to-un-peacekeepers-report-says/2013/07/25/7732341e-f552-11e2-a2f1-a7acf9bd5d3a_story.html.137 See, e.g., CDC Update, supra note 33. In November2010 the CDC tested 14 specimens isolatedfrom patients in the Artibonite Departmentduring the first month of the outbreak. Allsamples were serogroup O1, biotype El Tor, serotypeOgawa. Additionally, isolates were alsocharacterized by a pulsed-field gel electrophoresisprotocol developed by PulseNet international.All samples were PulseNet PFGE patterncombination KZGN11.0092/KZGS12.0088.138 See Chin, supra note 72; Hendriksen, supranote 72; Dasgupta, supra note 72. See also JazelDolores & Karla J. F. Satchell, Analysis of VibrioCholerae Genome Sequences Reveals Unique rtxAVariants in Environmental Strains and an rtxA-Null Mutation in Recent Altered El Tor Isolates,4 mBio 1 (2013) (documenting the increasedtoxicity of certain isolates from the Haitianepidemic).139 Dasgupta, supra note 72.140 Hendrikson, supra note 72, at 2.141 Researchers have sequenced genetic materialfrom 24 V. cholerae samples collected in differentdistricts of Nepal between July 30th andNovember 1st, 2010. Hendrikson, supra note72, at 2.142 A genetic isolate is a “population of organismsthat has minimal genetic mixing due to geographicalisolation or to other mechanismsthat prevented reproduction.” Genetic Isolates,Biology Online (Jul. 10, 2008, 8:24 AM), http://www.biology-online.org/dictionary/Genetic_isolate.143 Susceptible to tetracycline but resistant totrimethoprim-sulfamethoxazole, nalidixicacid, and with decreased susceptibility tociprofloxacin. Hendrikson, supra note 72, at 3.144 A pulsotype is a distinct genetic pattern createdby pulse field gel electrophoresis.145 Hendrikson, supra note 72, at 3.146 Author’s Note: A single nucleotide polymorphismindicates that between the two strainsof cholera, the difference was so minimal thatonly a single element of their DNA was notedto be distinctly different.147 “Phylogenetic” means “of or relating to theevolutionary development of organisms.WordNet Search – 3.1, http://wordnetweb.princeton.edu/perl/webwn?s=Phylogenetic&-sub=Search+WordNet&o2=&o0=1&o8=1&o1=1&o7=&o5=&o9=&o6=&o3=&o4=&h=.148 Hendrikson, supra note 72, at 2.149 Chin, supra note 72.150 Id.151 L.S. Katz et al., Evolutionary Dynamics of VibrioCholerae O1 Following a Single-Source Introductionto Haiti, 4 mBio 2 (2013).152 Id.153 Id. at 6.154 Id at 2. The study calculated the molecularclock based on the detected nuclear polymorphismand the observed epidemic behavior.Using an exponential model of populationgrowth, they estimated a “most recent commonancestor” date of September 28th, 2010(95% credibility interval, July 23rd, 2010-October17th, 2010). The credibility interval encompassesthe dates of the cholera outbreakin Nepal (July 28th-August 14th, 2010), the arrivalof the Nepalese soldiers in Haiti (October8th-21st, 2010), and the first reported hospitalizationof a cholera case (October 19th, 2010),further supporting the time frame mentionedpreviously by Piarroux and others.155 Id. at 4. Hendriksen, supra note 72. For additionalgenetic evidence, see R. Sealfon et al.,High Depth, Whole-Genome Sequencing of CholeraIsolates from Haiti and the Dominican Republic,13 BMC Genomics 468 (Sep. 11, 2012), availableat http://www.biomedcentral.com/1471-2164/13/468.156 N.A. Hasan et al., Genomic diversity of 2010 Haitiancholera outbreak strains, 109 PNAS 29 (Jul.17, 2012), available at http://www.pnas.org/cgi/doi/10.1073/pnas.1207359109.157 J.J. Mekalanos et al., Non-O1 Vibrio Cholerae64endnotes
Unlinked to cholera in Haiti, 109 PNAS 47 (Nov.20, 2012), available at http://www.pnas.org/content/109/47/E3206.full.158 R.R. Frerichs et al., Source Attribution of 2010Cholera Epidemic in Haiti. 109 PNAS 49 (Nov. 20,2012), available at http://www.pnas.org/content/109/47/E3208.extract.159 Id.160 Id.161 U.N. Charter art.105(1)-(2) (emphasis added).162 See Convention on Privileges and Immunitiesof the United Nations, arts. II § 2, IV § 11, Feb.13, 1946, 16 U.N.T.S. 1946-47, available at http://www.un.org/en/ethics/pdf/convention.pdf(emphasis added).163 Id. art. VII § 29.164 August Reinisch, Convention on Privileges andImmunities of the United Nations, Conventionon Privileges and Immunities of the SpecializedAgencies, United Nations Audiovisual Libraryof International <strong>Law</strong> (2009) at 2, http://untreaty.un.org/cod/avl/pdf/ha/cpiun-cpisa/cpiun-cpisa_e.pdf.165 U.N. Secretary General, Financing of the UnitedNations Protection Force, the United NationsConfidence Restoration Operation in Croatia, theUnited Nations Preventive Deployment Force andthe United Nations Peace Forces Headquarters: Reportof the Secretary-General, Mar. 19, 2001, U.N.Doc. No. A/51/389, available at http://daccessdds-ny.un.org/doc/UNDOC/GEN/N96/249/39/PDF/N9624939.pdf?OpenElement.166 Id.167 Maarten Zwanenburg, <strong>Accountability</strong> ofPeace Support Operations 36 (2005).168 Id.169 Comprehensive Review of the Whole Questionof <strong>Peacekeeping</strong> Operations in All TheirAspects: Model Status-of-Forces Agreementfor <strong>Peacekeeping</strong> Operations, Oct. 9, 1990, U.N.Doc. A/45/594, at 1 (“[T]he General Assemblyrequested the Secretary-General to preparea model status-of-forces agreement betweenthe United Nations . . . and to make that modelavailable to Member States. . . . The modelis intended to serve as a basis for the draftingof individual agreements to be concludedbetween the United Nations and countries on65whose territories peace-keeping operationsare deployed.”) [hereinafter Model SOFA].170 Id. at 1.171 Id.172 Zwanenburg, supra note 167, at 36.173 Id. at 36 n.145-146.174 See, e.g., Model SOFA, supra note 169, art. VI,§§ 24-50 (generally outlining privileges andimmunities of peacekeepers).175 Maria-Elena Kolovros & Beatrice Lindstrom,U.N. Must Take Responsibility for Haiti CholeraOutbreak, Jurist.com (Feb. 23, 2012), http://jurist.org/hotline/2012/02/kolovos-lindstrom-cholera-haiti.php.176 Model SOFA, supra note 169, at 13 (emphasisadded). The Model SOFA excepts from thisgeneral requirement arbitration proceduresunder Article 53. Article 53, which providesfor a three-member arbitration panel, applieswhen both parties jointly agree to appeal ajudgment from the claims commission orfor other disputes not covered under Article51. See id. (“Any other dispute between theUnited Nations peacekeeping operations andthe government, and any appeal that bothof them agree to allow from the award of aclaims commission . . . shall . . . be submittedto a tribunal of three arbitrators.”).177 Id.178 Haitian SOFA, supra note 82, 55.179 Id.180 Interview with Maître Jacceus Joseph, supranote 85.181 The SOFA provides, “If no agreement as tothe chairman is reached by the two partieswithin 30 days of the appointment of thefirst member of the commission, the Presidentof the International Court of Justicemay, at the request of either party, appointthe chairman.” Model SOFA, supra note 169.In other words, as soon as either the HaitianGovernment or the Secretary-General appointtheir claims commissioner, and 30 days passfollowing the appointment, the appointingparty can petition the president of the ICJto appoint a chairman. Once a chairman isappointed, the two-member quorum will besatisfied; as the SOFA specifies, “[t]he commisendnotes
sion shall determine its own procedures, providedthat any two members shall constitutea quorum for all purposes…and all decisionsshall require the approval of any two members.”Id.182 See, e.g., Richard Feinberg, Review: Fixing Haiti:MINUSTAH and Beyond, Foreign Affairs (Jan./Feb. 2012), available at http://www.foreignaffairs.com/articles/136913/fixing-haiti-minustah-and-beyond.183 Tom Dannenbaum, Translating the Standard ofEffective Control into a System of Effective <strong>Accountability</strong>:How Liability Should Be Apportionedfor Violations of Human Rights by Member StateTroop Contingents Serving as United NationsPeacekeepers, 51 Harv. Int’l L. J. 113, 126 (2010).184 See Financing of the United Nations ProtectionForce, supra note 89.185 See Amy Lieberman, Haiti Cholera Case RaisesQuestions About UN <strong>Accountability</strong>, WorldPolitics Review (Dec. 1, 2011), available athttp://www.worldpoliticsreview.com/articles/10808/haiti-cholera-case-raises-questions-about-u-n-accountability.186 Financing of the United Nations Protection Force,supra note 89, at 7.187 Id.188 Id.189 Dannenbaum, supra note 183, at 126.190 Dahpna Shraga, UN <strong>Peacekeeping</strong> Operations:Applicability of International Humanitarian <strong>Law</strong>and Responsibility for Operations-Related Damage,94 Am. J. Int’l L. 406 (2000).191 Dannenbaum, supra note 183, at 126 (“Becausethe claims review board deliberations aremade in secret, there is very little public informationavailable about the kind of claimsthey deliberate.”).192 Assistant Secretary-General, InterofficeMemorandum dated Mar. 26, 2009 from theOffice of Program Planning to the Controller,Budgets and Accounts regarding ex gratiapayment to an injured Haitian civilian,United Nations Juridical Yearbook 428-432(2009), available at http://books.google.com/books?id=upZ-WB-cUFYC&pg=PA429&lpg=PA429&dq=minustah+claims+review+board&source=bl&ots=sLSC9N-Ril&sig=AOPiCAK9tPage4cdh5VYKOVy-dY&hl=en&sa=X&ei=FxZ8UfGBFaLl4AOp-6oGAAg&ved=0CDQQ6AEwAA#v=onepage&q=minustah%20claims%20review%20board&f=false.193 Dannenbaum, supra note 183, at 126.194 Id. at 127 n.106.195 Haitian SOFA, supra note 82, art. VIII, 55.196 Petition for Relief, supra note 89, 4.197 Id. 66.198 Letter from Patricia O’Brian, supra note 93.199 See Haitian SOFA, supra note 82.200 Id. art. VIII, 55.201 See Ernest Weinrib, The Idea of Private <strong>Law</strong> 8(2012) (“On the institutional side, private lawinvolves an action by plaintiff against defendant,a process of adjudication, a culminationof that process in a judgment that retroactivelyaffirms the rights and duties of the parties,and an entitlement to specific relief or todamages for the violations of those rights orthe breach of those duties. On the conceptualside, private law embodies a regime of correlativerights and duties that highlights, amongother things, the centrality of the causationof harm of the distinction between misfeasanceand nonfeasance.”).202 See Randy E. Barnett, Four Senses of the Public-Private<strong>Law</strong> Distinction, 9 Harv. J. L. & Pub.Pol. 267, 269-70 (1986).203 See Petition for Relief, supra note 89.204 Financing of the United Nations Protection Force,supra note 89, at 6.205 See, e.g., Kristin Boon, UN Flatly Rejects HaitiCholera Claim, Opinio Juris (Feb. 22, 2013),http://opiniojuris.org/2013/02/22/un-flatly-rejects-haiti-cholera-claim/(“Many elements ofa “dispute of a private law character”, however,would appear to be present: the claim itselfwas essentially one of tort, the claimantswere private individuals (represented by anNGO), and the remedy sought was monetarycompensation.”).206 Financing of the United Nations Protection Force,supra note 89, 13.207 Id. 14.208 Brzak v. United Nations, 597 F.3d 107 (2d Cir.2010) (noting the various sources of law that66endnotes
shield the UN from immunity in Americancourts).209 See, e.g., Dannenbaum, supra note 183.210 Matt Halling & Blaine Bookey, <strong>Peacekeeping</strong> inName Alone: <strong>Accountability</strong> for the United Nationsin Haiti, 31 Hastings Int’l & Comp. L. Rev. 461,481 (2008)211 Dannenbaum, supra note 183 at 113. See alsoJordan J. Paust, The U.N. Is Bound By HumanRights: Understanding the Full Reach of HumanRights, Remedies, and Nonimmunity, 51 HarvardInt’l L. J. 301 (2010). The United Nations International<strong>Law</strong> Commission recently adopted aseries of draft articles on the responsibility ofinternational organizations for committingan “internationally wrongful act.” One generalprinciple of the draft articles is that “[e]veryinternationally wrongful act of an internationalorganization entails the internationalresponsibility of that organization.” Int’l <strong>Law</strong>Comm’n Draft Articles on the Responsibilityof International Organizations, Report of theInternational <strong>Law</strong> Commission Sixty-thirdSession, art. 3, U.N. GAOR 66th Sess., U.N. DocA/66/10, 77-88 (Apr. 26, June 3 & July 4-Aug. 12,2011 [hereinafter Draft Articles].212 See supra Chapter I.A at 5-6 for a descriptionof accusations of physical abuse and sexualexploitation committed by MINUSTAH troopsin Haiti.213 “The United Nations shall possess juridicalpersonality.” Convention on the Privilegesand Immunities of the United Nations, Feb.13, 1946, 1 U.N.T.S. 15, art. 1, § 1[hereinafterGeneral Convention].214 Reparation for Injuries Suffered in the Serviceof the United Nations, Advisory Opinion, 1949I.C.J. 174, 179 (Apr. 11).215 Id.216 U.N. Charter art. 1, para. 3.217 Financing of the United Nations Protection Force,supra note 89, 6.218 Id.219 Draft Articles, supra note 211, at 86 (quotingLetter dated 3 February 2004 from the UnitedNations Legal Counsel to the Director of theCodification Division, A/CN.4/545, sect. II.G.).220 U.N. Charter art. 55(c).221 World Conference on Human Rights, June 14-25, 1993, Vienna Declaration and Programmeof Action, 4, U.N. Doc. A/CONF.157/24 (July12, 1993).222 S.C. Res. 1927, supra note 21, prmbl.223 Legal Consequences for States of the ContinuedPresence of South-Africa in Namibia (South WestAfrica) notwithstanding Security Council Resolution276, Advisory Opinion, 1971 I.C.J. 16, 57 131.224 Haitian SOFA, supra note 82, 5.225 “Once international treaties or agreementsare approved and ratified . . . they becomepart of the legislation of the country and abrogateany laws in conflict with them.” Constitutionde la République d’Haïti 1987, art. 276-2.226 See supra Chapter IV.A.227 Customary international law includes thosehuman rights provisions of the UniversalDeclaration of Human Rights (UDHR) thathave achieved customary force. While therights that arise under customary internationallaw are evolving with practice, it isclear that the right to an effective remedy,which is found in the UDHR as well as othertreaties, has reached customary status. InternationalHuman Rights <strong>Law</strong>: Cases, Materials,Commentary 50 (Olivier De Schutter ed.,2010). See Chapter IV for a detailed discussionof the right to an effective remedy.228 Statute of the International Court of Justiceart. 38(1)(b), Apr. 18, 1946. See Frédéric Mégret& Florian Hoffmann, The UN as a HumanRights Violator? Some Reflections on the UnitedNations Changing Human Rights Responsibilities,25 Hum. Rts. Q. 314, 317 (2003). Mégret andHoffmann additionally note that, “it has beencontended that, in the case of ‘treaties thathave been drafted by representatives of nearlyall States with the intention of creatinguniversal law,’ international organizations,whose ‘constitutional roots are in internationallaw’ cannot invoke their non-partystatus.” Id. (quoting Henry G. Schermers etal., International Institutional <strong>Law</strong>: UnityWithin Diversity 824 (1995)). See also Dannenbaum,supra note 183, at 135, 135 n.161 (observingthat customary international law binds to67endnotes
the United Nations as, “a consequence of theUnited Nations’ legal personality at internationallaw,” and arguing that objections tothis application of customary internationallaw on the grounds that customary internationallaw is tailored to States “is significantlymitigated by the qualifier that customary lawapplies to the United Nations only mutatismutandis,” that is, with consideration for therespective differences between States and theUnited Nations).229 Mégret & Hoffmann, supra note 228.230 The Restatement (Third) of the Foreign Relations<strong>Law</strong> of the United States notes thatcustomary international law, in contrast totreaties, “results from a general and consistentpractice of states followed by them froma sense of legal obligation.” § 102(2) (1987).231 Id. at § 102(3), cmt. f; § 301(1).232 See supra note 228 and accompanying text.233 As noted in supra note 230, customary internationallaw applies to the U.N. only mutatismutandis, or only as is consistent with itsnature as an entity. Hence, where the standardin question is one that the UN as aninternational entity has already committeditself to, holding the U.N. to its dictates doesnot run afoul of concerns that customary lawis tailored to states, not international organizations.The right to remedy which notes thatremedies under the General Convention mustbe consistent with the access to courts rightfound in human rights treaties), is one suchinstance of the appropriate application of customaryinternational law to the UN. For anobjection to the application of customary lawto the UN on the grounds that its rules aremeant for states, see Judith G. Gardam, LegalRestraints on Security Council Military EnforcementAction, 17 Mich. J. Int’l L. 285, 319 (1996);J.E. Alvarez, Memo: ILC’s Draft Articles on theResponsibility of International Organizations(June 21, 2010), http://www.law.nyu.edu/ecm_dlv2/groups/public/@nyu_law_website__faculty__faculty_profiles__jalvarez/documents/documents/ecm_pro_066900.pdf.234 U.N. Charter prmbl.235 In 1993, it created the Office of the High Commissionfor Human Rights, which is mandatedto, among other things, prevent humanrights violations, secure respect for all humanrights, and promote international cooperationto protect human rights. Who We Are: Mandate,Office of the High Commissioner for HumanRights, http://www.ohchr.org/EN/AboutUs/Pages/Mandate.aspx. In 2006, the GeneralAssembly established the Human RightsCouncil, the responsibilities of which include“promoting universal respect for the protectionof all human rights” and “address[ing]situations of violations of human rights.” G.A.Res. 60/251, U.N. GAOR, 60th Sess., U.N. Doc.A/Res/60/251, 2 (Apr. 3, 2006).236 José Ayala Lasso, Human Rights in the UnitedNations: The Achievements So Far and ChallengesAhead, 1 Int’l J. of Peace Studies (1996).237 G.A. Res. 64/292, U.N. GAOR, 64th Sess., U.N.Doc. A/RES/64/292, 2 (Aug. 3, 2010). Althoughthe Resolution does not itself establish a rightto water binding on the states, it draws fromthe right of children, women, and peoplewith disabilities to clean water that has beenrecognized in the Convention on the Rightsof the Child (CRC), Convention on the Eliminationof All Forms of Discrimination againstWomen (CEDAW), and Convention on theRights of Persons with Disabilities (CRPD),all treaties to which Haiti has either accededor ratified. Convention on the Rights of theChild art. 24(2)(c), opened for signature Nov.20, 1989, 1577 U.N.T.S. 3 (ratified by Haiti onJune 8, 1995) [hereinafter CRC]; Conventionon the Elimination of All Forms of Discriminationagainst Women art. 14(2)(h), opened forsignature Mar. 1, 1980, 1249 U.N.T.S. 13 (ratifiedby Haiti on July 20, 1981) [hereinafter CEDAW];Convention on the Rights of Persons withDisabilities art. 28(2)(a), opened for signatureMar. 30, 2007, 2515 U.N.T.S. 3 (acceded to byHaiti on July 23, 2009) [hereinafter CRPD].238 Human Rights Council, Human rights andaccess to safe drinking water and sanitation, 15thSess., Sept. 24, 2010, U.N. Doc. A/HRC/15/L.14.The right to an adequate standard of living iscodified in Article 25 of the Universal Declarationof Human Rights and Article 11 of the68endnotes
International Covenant on Economic, Social,and Cultural Rights. Universal Declaration ofHuman Rights art. 25, G.A. Res. 217, U.N. GAOR3d Sess., U.N. Doc. A/810 (1948) [hereinafterUDHR]; International Covenant on Economic,Social, and Cultural Rights art. 11, opened forsignature Dec. 19, 1966, 993 U.N.T.S. 3 (ratifiedby Haiti on Feb. 2, 2012) [hereinafter ICESCR].The rights to the highest attainable standardof health and life are discussed in infra ChapterIV.C.2 and C.3, respectively.239 Sawhoyamaxa Indigenous Community v.Paraguay, Merits, Reparations and Costs,Inter-Am. Ct. H.R. (ser. C) No. 146, 168, 178(Mar. 29, 2006).240 International Covenant on Economic, Socialand Cultural Rights: The Right to Water,Comm. on Economic, Social and CulturalRights, 29th sess., gen. cmt. 15, 12, U.N. Doc.E/C.12/2002/11 (Jan. 20, 2003) [hereinafter TheRight to Water].241 Id. at 42, 44.242 Id. 17.243 See Cravioto, supra note 66.244 See, e.g., Constitution de la République d’Haïti1987 arts. 253, 258 (forbidding “any practicesthat might disturb the ecological balance” ofthe environment and prohibiting the introductionof “wastes or residues of any kindfrom foreign sources” into the country).245 Paul Farmer, former U.N. Deputy SpecialEnvoy for Haiti and current Special Advisorto the U.N. Secretary-General for Community-basedMedicine and Lessons from Haiti,described Haiti as the “most water insecure”country in the world in 2011. AP Interview: Expertsays Haiti has worst cholera, The Guardian(Oct. 18, 2011), available at http://www.guardian.co.uk/world/feedarticle/9902077.246 The Denial of the Right to Water in Haiti,supra note 43.247 Brian Concannon Jr. & Beatrice Lindstrom,Cheaper, Better, Longer-Lasting: A Rights-BasedApproach to Disaster Response in Haiti, 25 EmoryInt’l L. R. 1145, 1168 (2011).248 UDHR, supra note 238, art. 25(1).249 ICESCR, supra note 238, art. 12(b)-(c).250 CRC, supra note 237, art. 24; CEDAW, supra note237, art. 12(1); International Convention on theElimination of All Forms of Racial Discrimination,art. 5(e)(iv), opened for signature Dec. 21,1965, 660 U.N.T.S. 195 (ratified by Haiti on Dec.19th, 1972) [hereinafter CERD]; CRPD, supranote 237, art. 25.251 American Declaration on the Rights and Dutiesof Man art. XI, O.A.S. Res. XXX, adopted bythe Ninth International Conference of AmericanStates, Bogota, Colombia, Mar. 30-May 2,1948, OEA/Ser. L./V/II.23/doc. 2 rev. 6 (1979).252 ICESCR, supra note 238, art. 12(2)(b)-(c).253 CRC, supra note 237, art. 24(c).254 International Covenant on Economic, Socialand Cultural Rights: The right to the highestattainable standard of health, Comm. on Economic,Social and Cultural Rights, 22d sess.,gen. cmt. 14, 4, U.N. Doc. E/C.12/2000/4 (Aug.11, 2000).255 Id. 39, 59.256 Id. 40.257 See supra Chapter III.C.258 International Covenant on Civil and PoliticalRights: The right to life, Human RightsComm., 16th Sess., gen. cmt. 6, 5, U.N. Doc.HRI/GEN/1/Rev. 9 (Apr. 30, 1982) [hereinafterICCPR].259 Digital record of the UDHR, Office of the HighCommissioner for Human Rights (Feb., 2009),available at http://www.ohchr.org/EN/NEW-SEVENTS/Pages/DigitalrecordoftheUDHR.aspx.260 Id. (“The UDHR was proclaimed by the GeneralAssembly on 10 December 1948, and sincethen is widely regarded as forming part ofcustomary international law.”)261 UDHR, supra note 238, art. 8. Scholars haveargued that the U.N.’s legal personality rendersit legally accountable under customaryinternational law, including the UDHR.262 International Human Rights <strong>Law</strong>: Cases, Materials,Commentary, supra note 227.263 American Convention on Human Rights art.25(1), OAS Official Records, OEA/Ser.K/XVI/1.1,Doc. 65, Rev. 1, Corr. 1 (1970).264 ICCPR, supra note 258, art. 2(3); CERD, supranote 250, art. 6; CRC, supra note 237, art. 39.In recognizing a right to water within the69endnotes
ICESCR, the UN Committee on Economic, Social,and Cultural Rights has also noted thatvictims of a violation of this right “should beentitled to adequate reparation.” The Right toWater, supra note 240, 55.265 International Covenant on Civil and PoliticalRights: The Nature of the General LegalObligation Imposed on States Parties to theCovenant, Human Rights Comm., 80th Sess.,gen. cmt. 31, 16, U.N. Doc. CCPR/C/21/Rev.1/Add.13 (May 26, 2004).266 Basic Principles and Guidelines on the Rightto a Remedy and Reparation for Victims ofViolations of International Human Rightsand Humanitarian <strong>Law</strong>, G.A. Res. 60/147, U.N.GAOR, 60th Sess., U.N. Doc. A/RES/60/147, 18 (Mar. 21, 2006). Restitution “includes, asappropriate, restoration of liberty, enjoymentof human rights, identity, family life andcitizenship, return to one’s place of residence,restoration of employment and return ofproperty.” Id. at 19. Compensation “shouldbe provided for any economically assessabledamage, as appropriate and proportional tothe gravity of the violation and the circumstancesof each case . . . such as: (a) Physical ormental harm; (b) Lost opportunities, includingemployment, education and social benefits;(c) Material damages and loss of earnings,including loss of earning potential; (d) Moraldamage; (e) Costs required for legal or expertassistance, medicine and medical services,and psychological and social services.” Id.at 20. Rehabilitation “should include medicaland psychological care as well as legaland social services.” Id. at 21. Satisfactionshould include “[e]ffective measures aimed atthe cessation of continuing violations . . . [v]erification of the facts and full and public disclosureof the truth . . . [a]n official declarationor judicial decision restoring the dignity, thereputation and the rights of the victim and ofpersons closely connection with the victim. . . [p]ublic apology, including acknowledgementof the facts and acceptance of responsibility. . . [j]udicial and administrative sanctionsagainst persons liable for the violations. . . [c]ommemorations and tributes to thevictims . . . [i]nclusion of an accurate accountof the violations that occurred in internationalhuman rights law and internationalhumanitarian law training and in educationmaterial at all levels.” Id. at 22. Guaranteesof non-repetition should include “[e]nsuringeffective civilian control of military andsecurity forces . . . [p]roviding, on a priorityand continued basis, human rights and internationalhumanitarian law education to allsectors of society and trainng for law enforcementofficials as well as military and securityforces . . . [p]romoting the observance of codesof conduct and ethical norms, in particularinternational standards, by public servants . .. [r]eviewing and reforming laws contributingto or allowing gross violations of internationalhuman rights law and serious violations ofinternational humanitarian law.” Id. 23.267 Id. 15.268 Id. at 4.269 LaGrand (Ger. v. U.S.), 2001 ICJ Rep. 466.270 La Cantuta v. Peru, Inter-Am. Ct. H.R., (ser. C)No.162 201 (Nov. 29, 2006).271 The U.N.’s refusal to remedy the harms it hascaused in Haiti is discussed in Chapter I; thelegal basis of its obligation to provide such aremedy is detailed in Chapter III.272 The Final Report of the Independent Panelof Experts on the Cholera Outbreak in Haiti,released by the UN in 2011, issued sevenrecommendations to the UN for responding tothe outbreak, including providing UN personneland emergency responders traveling fromcholera-endemic areas with prophylactic antibioticsand screening personnel and emergencyresponders for asymptomatic carriageof cholera bacteria prior to departure, immunizingpersonnel and emergency respondersagainst cholera, and treating waste at worldwideUN installations using on-site treatmentsystems maintained by trained and qualifiedstaff or by local providers with adequate UNoversight. Cravioto, supra note 66, at 30; seealso Physicians for Haiti, Protecting Peacekeepers& Their Public: A report card on UNimplementation of their recommendationsfor cholera in Haiti (May 2013), available at70endnotes
http://physiciansforhaiti.org/wp-content/uploads/2013/05/P4H-UN-report-card-wo-PR.pdf.As of May 2013, the UN had only fully implementedtwo of the seven recommendations,and none of those listed above. Physiciansfor Haiti, supra. Notably, the unimplementedrecommendations “would have prevented UNintroduction of cholera into Haiti and wouldprevent similar introduction in the future . .. [and] could be implemented at either no orminimal cost to the UN.” Id. The recommendationsthat were completely implemented,according to Physicians for Haiti, “rel[ied]heavily on action and funding outside UNagencies.” Id.273 See supra Chapter III for further discussion.274 Nicholas Leader, The Politics of Principle: ThePrinciples of Humanitarian Action in Practice, inOverseas Development Institute--HumanitarianPolicy Group 5-6 (2000). available at http://www.odi.org.uk/sites/odi.org.uk/files/odi-assets/publications-opinion-files/311.pdf275 Id. at 5. See also Dorothea Hilhorst, Dead letteror living document? Ten years of the Code of Conductfor disaster relief, 19 Disasters 351 (2005);Nicholas Leader, Proliferating Principles; or Howto Sup with the Devil <strong>without</strong> Getting Eaten, 22Disasters 288, 289 (1998).276 International Committee of the Red Cross,Code of Conduct for the International Red Crossand Red Crescent Movement and Non-GovernmentalOrganizations in Disaster Relief art. 10 (1994)[hereinafter ICRC Code of Conduct], available athttp://www.icrc.org (noting the concern totreat disaster victims as dignified humans,not hopeless objects); Sphere Project, HumanitarianCharter and Minimum Standards inDisaster Response 5 (2004 ed.) [hereinafterSphere Project 2004 ed.] (stating Sphere is basedon two base concepts a concern with alleviatingsuffering and recognizing those affectedby a disaster have a right to life with dignity);HAP International, The Guide to the HAPStandard: Humanitarian <strong>Accountability</strong> andQuality Management 4–5 (2008) [hereinafterGuide to the HAP Standard] (explaining theHAP Standard seeks to protect the dignity ofthose affected by disasters).71277 ICRC Code of Conduct, supra note 276, arts. 8, 9(expressing a commitment to reduce futurevulnerability to disaster and ensuring appropriatemonitoring of aid); Sphere Project 2004ed., supra note 276, at 13 (affirming Sphere’scommitment to the quality of aid), Guide tothe HAP Standard, supra note 276, at 13 (notingthe HAP Standard’s concern with improvingthe quality of aid).278 See, e.g., Constanza Adionolfi et al., Office forthe Coordination of Humanitarian Affairs,Humanitarian Response Review 10, 20 (2005)(noting the widespread acknowledgement ofthe importance of the ICRC Code of Conduct,the Sphere Standards, and the HAP Standardamong humanitarian organizations, includingU.N. agencies).279 ICRC Code of Conduct, supra note 276, art. 9.280 Leader, supra note 275, at 275.281 Id. at 296. See also, ICRC Code of Conduct, supranote 276, arts. 1, 9. The ICRC’s Code of Conductdoes not include a formal do no harm principle.However, the “humanitarian imperative”articulated in Article 1 of the Code hasbeen understood to encompass a principle ofnon-maleficence. For the accountability principle,see Article 9 of the Code.282 International Committee of the Red Cross,Code of Conduct for the International Red Crossand Red Crescent Movement and NGOs in DisasterRelief List of Signatories (2012), available at http://www.ifrc.org/; Hilhorst, supra note 275, at363–367.283 Peter Walker & Susan Purdin, Birthing Sphere,24 Disasters 100, 101 (2004).284 Id. at 102. For the original evaluation of the responseof humanitarian organizations duringthe Rwandan genocide, see John Eriksson etal., The International Response to Conflictand Genocide: Lessons from the Rwanda Experience(Mar. 1996), available at https://www1.oecd.org/derec/sweden/50189495.pdf.285 Id. at 108.286 The Sphere Standards were also revised in2011, but this report discusses only the 2004edition, as this was the edition in use duringthe 2010 cholera outbreak. Notably, however,the revisions make even clearer the fundaendnotes
mental obligations of protection. The 2011edition incorporates a series of protectionprinciples to: (1) avoid exposing people to furtherharm; (2) ensure access to impartial assistance;(3) protect people from harm arisingfrom violence and coercion; (4) assist peopleto claim their rights and access remedies. SeeSphere Project, Humanitarian Charter andMinimum Standards in Disaster Response 28(2011 ed.).287 Sphere Project 2004 ed., supra note 276, at 16-17.288 Id. at 16.289 Lotus McDougal & Jennifer Beard, RevisitingSphere: New Standards of Service Delivery for NewTrends in Protracted Displacement, 35 Disasters87, 90 (2010).290 Margaret L. Satterthwaite, Indicators inCrisis: Rights-based Humanitarian Indicators inPost-Earthquake Haiti, 43 N.Y.U J. of Int’l L. &Pol. 865, 887–888 (2011).291 Id. at 888. HAP functions as a self-regulatorybody seeking to promote good accountabilitypractices among NGOs that offer humanitarianrelief. The organization has 68 full membersand 19 associate members ranging fromagencies working in emergency relief to institutionaldonors. Additionally, HAP has itsown General Assembly, Board, and Secretariat.Together, these different bodies functionto promote the HAP standards and principles,and assist members to find solutions wherecomplaints are raised. See About us, Hap Int’l(2013), http://www.hapinternational.org/about.aspx.292 HAP International, HAP 2007 Standard in Humanitarian<strong>Accountability</strong> and Quality Management5 (2007) [hereinafter Hap 2007 Standard].The HAP Standard was revised in 2010, butthis report discusses only the 2007 edition,as this was the edition in use during the 2010cholera outbreak.293 Id. at 11.294 Walker & Purdin, supra note 283, at 102 (discussingthe Sphere Project consultations);Satterthwaite, supra note 290, at 897 (discussingthe HAP Standard consultations).295 U.N. High Commissioner for Refugees, Handbookfor Emergencies 262 (2007 3rd ed.), availableat, http://www.unhcr.org [hereinafter UNHCRHandbook]. See also U.N. High Commissionerfor Refugees, Excreta Disposal in Emergencies:A Field Manual 197 (2009), available at, http://www.unhcr.org (incorporating Sphere indicatorsin the excreta disposal guidelines)[hereinafter UNHCR Disposal in Emergencies],296 World Health Organization & Water, Engineeringand Development Centre at LoughboroughUniversity, Technical Notes onDrinking-Water, Sanitation and Hygiene inEmergencies 7.1, 7.4, 13.2, 13.1 (2011). See alsoUnited Nations Children’s Fund, Handbook onWater Quality 129–130 (2008) (also citing theSphere Standard as a key reference).297 Adionolfi, supra note 278, at 8, 20.298 U.N. Under-Secretary-General for <strong>Peacekeeping</strong>Operations, United Nations <strong>Peacekeeping</strong>Operations: Principles and Guidelines23 (2008), available at http://www.un.org/en/peacekeeping/operations/principles.shtml(noting the changing nature of peacekeepingmandates of U.N. missions).299 S.C. Res. 1542, 8–9, U.N. Doc. S/RES/1542(Apr. 30, 2004).300 Id. 9.301 S.C. Res. 1908, U.N. Doc. S/RES/1908 (Jan.19, 2010); S.C. Res. 1927, 5–8., U.N. Doc. S/RES/1927 (June 4, 2010).302 MINUSTAH Apr. 2010 Report, supra note 20, 2–4; MINUSTAH Sept. 2010 Report, supra note23, 44–50.303 MINUSTAH Apr. 2010 Report, supra note 20, 14,57; MINUSTAH Sept. 2010 Report, supra note 23, 30.304 See, e.g., MINUSTAH Apr. 2010 Report, supra note20, 10; MINUSTAH Sept. 2010 Report, supranote 23, 24.305 MSPP Plan, supra note 43. See also The Denialof the Right to Water in Haiti, supra note 43.306 In the peacekeeping context, the principleis not absolute, but rather weighted againstthe operational necessity of a particularobjective. Likewise, the recognition of responsibilityfor damages to third partiesapplies a broader principle of accountabilityto affected populations. See Dapnha Shraga,U.N. <strong>Peacekeeping</strong> Operations: Applicability of72endnotes
International Humanitarian <strong>Law</strong> and Responsibilityfor Operations-Related Damage, 94 Am. J. ofInt’l L. 406, 409 (2000). For more on the principlegenerally, see Hugo Slim, Doing the RightThing: Relief Agencies, Moral Dilemmas and MoralResponsibility in Political Emergencies and War, 21Disasters 244, 244 (1997). For an early articulationof the principle, see Mary B. Anderson,Do No Harm: How Aid Can Support Peace—OrWar (1999). See also Mary B. Anderson, Aid: AMixed Blessing, 10 Development in Practice 495(2000). The negative impacts of humanitarianoperations have been well documented andrange from creating dependency on aid, tounknowingly shifting balances of power ina host country, to spreading disease amongvulnerable populations. See, e.g., Aid Action,Real Aid: Ending Aid Dependency (2010); Alexde Waal, The Humanitarians’ Tragedy: Escapableand Inescapable Cruelties, 34 Disasters S130, S131(2010). Some of these phenomena have alreadybeen documented in Haiti. Matthew AaronMoore, Do No Harm and the Convergence ofRelief Development & Conflict Resolution 68(2012) (unpublished M.S. dissertation, GeorgeMason University) (on file with George MasonUniversity).307 Sphere Project 2004 ed., supra note 276, at 71–75.308 Id.309 See, e.g., Peter Harvey, United Nations Children’sFund et al., Excreta Disposal in Emergencies:A Field Manual 2 (2007), available athttp://www.unicef.org; UNHCR Handbook,supra note 295, at 295; UNHCR Disposal inEmergencies, supra note 295, at 197.310 Cravioto, supra note 66, at 21.311 Id. at 21.312 Id.313 See, e.g., Humanitarian <strong>Accountability</strong> Partnership,The 2010 HAP Standard in <strong>Accountability</strong>and Quality Management 1 (2010);Sphere Project 2004 ed., supra note 276, at 41.314 Humanitarian <strong>Accountability</strong> Partnership,supra note 313, at 1.315 Id. See also Overseas Development Institute,Promoting Mutual <strong>Accountability</strong> in Aid Relationships1 (2006) (recognizing the traditionalpower imbalance between donors and aidrecipients)..316 Id.317 Austen Davis, Humanitarian Practice Network,Concerning <strong>Accountability</strong> of HumanitarianAction 4 (2007), available at http://www.odihpn.org/index.php?option=com_k2&view=item&layout=item&id=2867.318 Id. at 1.319 Paul Know-Clarke & John Mitchell, Reflectionson the <strong>Accountability</strong> Revolution, 52 HumanitarianExchange 3 (2011).320 See Chapter VI for a complete elaboration offorms of effective remedy.321 See Chapter I for a detailed discussion of theadvocacy effort to hold the U.N. accountablefor the cholera epidemic.322 Haitian SOFA, supra note 82, at 55.323 Id.324 Elyse J. Garmise, The Iraqi Claims Process andthe Ghost of Versailles, 67 N.Y.U. L. Rev. 840, 842(1992). Note that the UNCC was also createdto compensate governments and corporationsfor harms suffered in the war, but theseclaims were processed in separate categoriesfrom those by victims. See The Claims, UnitedNations Compensation Commission, http://www.uncc.ch/theclaims.htm.325 See, e.g., David J. Biederman, The United NationsCompensation Commission and the Traditionof International Claims Settlement, 27 N.Y.U. J.Int’l L. & Pol. 1, 2 (1994); John F. Murphy, ForeignClaims, 31 Int’l <strong>Law</strong> 579, 586 (1997).326 Id. at 587.327 The UNCC At a Glance, United Nations CompensationCommission, http://www.uncc.ch/ataglance.htm.328 The Claims, United Nations CompensationCommission, http://www.uncc.ch/ataglance.htm.http://www.uncc.ch/theclaims.htm.329 Id.330 S.C. Res. 687 19, U.N. Doc. S/RES/687 (Apr. 8,1991).331 Murphy, supra note 325, at 587.332 A cholera claims commission would needto develop policies and procedures for choleracases arising after the commission wasestablished that are still traceable to theU.N. While these procedures might make73endnotes
this commission more open-ended than theUNCC, the UNCC still provides a window intohow long the cholera claims commissionwould take to complete the core of its work.333 Air Transportation Safety and System StabilizationAct, 49 U.S.C. §40101 et seq. (2001).334 Id. at 52.335 Air Transportation Safety and System StabilizationAct at §405(c)(3)(B).336 Kenneth Feinberg, et al., Final Report of theSpecial Master for the September 11th VictimCompensation Fund of 2001 1, 4-13 (2004) [hereinafterFinal Report], available at http://www.justice.gov/final_report.pdf.337 Kenneth Feinberg, Compensating the Familiesand Victims of September 11th: An Alternative tothe American Tort System, in Redressing InjusticesThrough Mass Claims Processes 235, 236(International Bureau of the Permanent Courtof Arbitration, ed., 2006).338 Final Report, supra note 336, at 241.339 Adams, supra note 55.340 Id.341 Id.342 Barzilay, supra note 35, at 599-609.343 MSPP Plan, supra note 43, §7.3.344 Id. §7.4.345 Center for Economic and Policy Research,Cholera Eradication Plan Announced, But FundingStill in Question (Feb. 27, 2013), http://www.cepr.net/index.php/blogs/relief-and-reconstruction-watch/cholera-eradication-plan-announced-but-funding-still-in-question346 Decreasing funds for cholera response andprevention is a growing challenge faced byGovernment of Haiti and the humanitariancommunity in combating the cholera epidemic.The Haiti Consolidated Appeal Process(CAP) for 2012, which underlined choleraresponse as a key priority, was revised fromUS$231 million to $128 million at the Mid-YearReview in July. It was again revised upwardsto US$151 million in December to address theimmediate needs of Haitians in the wake ofHurricane Sandy. As of December 11th, theAppeal has only been funded at 41 per centor about US$61 million, making it one of themost under-funded CAPs worldwide. Thecritical Health and WASH response plans arefunded at 47 per cent and 38 per cent, respectively.U.N. Haiti Factsheet on Cholera Preventionand Response (Dec. 2012), available at http://www.un.org/News/dh/infocus/haiti/Haiti%20Cholera%20Factsheet%20Dec%202012.pdf.347 MSPP Plan, supra note 43. See, e.g., PanAmerican Health Organization, PAHO/WHO calls for new international funding ofHaiti cholera plan (Feb. 27, 2013), http://www.paho.org/hai/index.php?option=com_content&view=article&id=7117%3Alops-fait-appel-au-financement-international-pour-le-nouveau-plan-contre-le-cholera-en-haiti&catid=674%3Ahai.-press-releases&Itemid=255&lang=en.348 World Health Organization, Water, Sanitationand Health §6 (2013), available at http://www.who.int/water_sanitation_health/sanitproblems/en/index5.html.349 See Todd Howland, <strong>Peacekeeping</strong> and Conformitywith Human Rights <strong>Law</strong>: How MINUSTAH FallsShort in Haiti, 13 Int’l <strong>Peacekeeping</strong> 462 (2006).See also OAS rights commission hears testimonyabout situation in Haiti, Associated Press (Mar.6, 2006).350 Michel Forst, Report of the independent experton the situation of human rights in Haiti, Feb. 7,2013, U.N. Doc. A/HRC/22/65.351 Consultation with Victims of the Cholera Epidemic,in Meye, Haiti (Mar. 20, 2013).352 See generally James Crawford et al, The <strong>Law</strong>of International Responsibility, ch. 39 (2010);Christian J. Tams, Recognizing Guarantees andAssurances of Non-Repetition, 27 <strong>Yale</strong> J. Int’l L.441 (2002).353 Dilek Kurban, Reparations and Displacement inTurkey, Brookings Project on Internal Displacement(2012).354 United Nations Office of the High Com’r forHuman Rights, Statement by the United NationsSpecial Rapporteur on the promotion of truth, justice,reparation and guarantees of non-recurrence(Nov. 16, 2012), available at http://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx-?NewsID=12800&LangID=E.74endnotes