

Volume 2 - Issue 1 (Nov-Jan) - IJMD
Volume 2 - Issue 1 (Nov-Jan) - IJMD
Volume 2 - Issue 1 (Nov-Jan) - IJMD

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
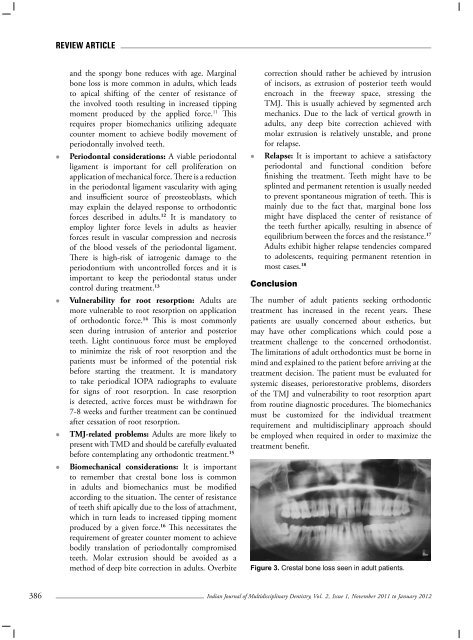
Review Articleand the spongy bone reduces with age. Marginalbone loss is more common in adults, which leadsto apical shifting of the center of resistance ofthe involved tooth resulting in increased tippingmoment produced by the applied force. 11 Thisrequires proper biomechanics utilizing adequatecounter moment to achieve bodily movement ofperiodontally involved teeth.• Periodontal considerations: A viable periodontalligament is important for cell proliferation onapplication of mechanical force. There is a reductionin the periodontal ligament vascularity with agingand insufficient source of preosteoblasts, whichmay explain the delayed response to orthodonticforces described in adults. 12 It is mandatory toemploy lighter force levels in adults as heavierforces result in vascular compression and necrosisof the blood vessels of the periodontal ligament.There is high-risk of iatrogenic damage to theperiodontium with uncontrolled forces and it isimportant to keep the periodontal status undercontrol during treatment. 13• Vulnerability for root resorption: Adults aremore vulnerable to root resorption on applicationof orthodontic force. 14 This is most commonlyseen during intrusion of anterior and posteriorteeth. Light continuous force must be employedto minimize the risk of root resorption and thepatients must be informed of the potential riskbefore starting the treatment. It is mandatoryto take periodical IOPA radiographs to evaluatefor signs of root resorption. In case resorptionis detected, active forces must be withdrawn for7-8 weeks and further treatment can be continuedafter cessation of root resorption.• TMJ-related problems: Adults are more likely topresent with TMD and should be carefully evaluatedbefore contemplating any orthodontic treatment. 15• Biomechanical considerations: It is importantto remember that crestal bone loss is commonin adults and biomechanics must be modifiedaccording to the situation. The center of resistanceof teeth shift apically due to the loss of attachment,which in turn leads to increased tipping momentproduced by a given force. 16 This necessitates therequirement of greater counter moment to achievebodily translation of periodontally compromisedteeth. Molar extrusion should be avoided as amethod of deep bite correction in adults. Overbitecorrection should rather be achieved by intrusionof incisors, as extrusion of posterior teeth wouldencroach in the freeway space, stressing theTMJ. This is usually achieved by segmented archmechanics. Due to the lack of vertical growth inadults, any deep bite correction achieved withmolar extrusion is relatively unstable, and pronefor relapse.• Relapse: It is important to achieve a satisfactoryperiodontal and functional condition beforefinishing the treatment. Teeth might have to besplinted and permanent retention is usually neededto prevent spontaneous migration of teeth. This ismainly due to the fact that, marginal bone lossmight have displaced the center of resistance ofthe teeth further apically, resulting in absence ofequilibrium between the forces and the resistance. 17Adults exhibit higher relapse tendencies comparedto adolescents, requiring permanent retention inmost cases. 18ConclusionThe number of adult patients seeking orthodontictreatment has increased in the recent years. Thesepatients are usually concerned about esthetics, butmay have other complications which could pose atreatment challenge to the concerned orthodontist.The limitations of adult orthodontics must be borne inmind and explained to the patient before arriving at thetreatment decision. The patient must be evaluated forsystemic diseases, periorestorative problems, disordersof the TMJ and vulnerability to root resorption apartfrom routine diagnostic procedures. The biomechanicsmust be customized for the individual treatmentrequirement and multidisciplinary approach shouldbe employed when required in order to maximize thetreatment benefit.Figure 3. Crestal bone loss seen in adult patients.386Indian Journal of Multidisciplinary Dentistry, Vol. 2, <strong>Issue</strong> 1, <strong>Nov</strong>ember 2011 to <strong>Jan</strong>uary 2012













