HSB Dental Claim Form 2010 - El Paso - HealthSCOPE Benefits
HSB Dental Claim Form 2010 - El Paso - HealthSCOPE Benefits
HSB Dental Claim Form 2010 - El Paso - HealthSCOPE Benefits

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
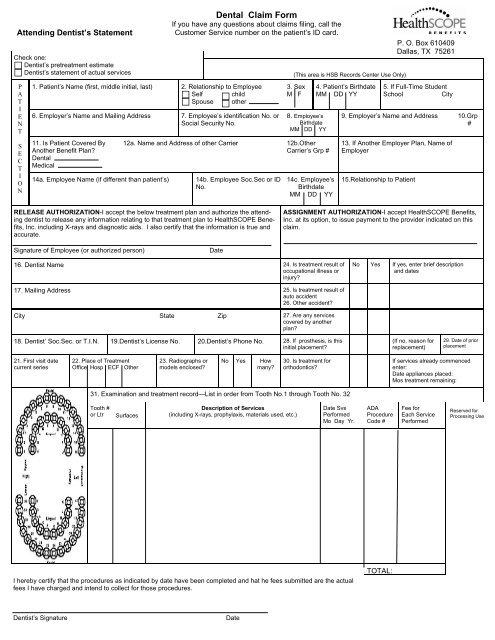
Attending Dentist’s StatementCheck one:Dentist’s pretreatment estimateDentist’s statement of actual servicesPATIENTSECTION1. Patient’s Name (first, middle initial, last)6. Employer’s Name and Mailing Address11. Is Patient Covered ByAnother Benefit Plan?<strong>Dental</strong>Medical14a. Employee Name (if different than patient’s)<strong>Dental</strong> <strong>Claim</strong> <strong>Form</strong>If you have any questions about claims filing, call theCustomer Service number on the patient’s ID card.2. Relationship to EmployeeSelf childSpouse other7. Employee’s identification No. orSocial Security No.(This area is <strong>HSB</strong> Records Center Use Only)3. SexM F8. Employee’sBirthdateMM DD YY12a. Name and Address of other Carrier 12b.OtherCarrier’s Grp #14b. Employee Soc.Sec or IDNo.14c. Employee’sBirthdateMM DD YY4. Patient’s BirthdateMM DD YYP. O. Box 610409Dallas, TX 752615. If Full-Time StudentSchoolCity9. Employer’s Name and Address 10.Grp#13. If Another Employer Plan, Name ofEmployer15.Relationship to PatientRELEASE AUTHORIZATION-I accept the below treatment plan and authorize the attendingdentist to release any information relating to that treatment plan to <strong>HealthSCOPE</strong> <strong>Benefits</strong>,Inc. including X-rays and diagnostic aids. I also certify that the information is true andaccurate.ASSIGNMENT AUTHORIZATION-I accept <strong>HealthSCOPE</strong> <strong>Benefits</strong>,Inc. at its option, to issue payment to the provider indicated on thisclaim.Signature of Employee (or authorized person)Date16. Dentist Name 24. Is treatment result ofoccupational illness orinjury?No Yes If yes, enter brief descriptionand dates17. Mailing Address 25. Is treatment result ofauto accident26. Other accident?City State Zip 27. Are any servicescovered by anotherplan?18. Dentist’ Soc.Sec. or T.I.N. 19.Dentist’s License No. 20.Dentist’s Phone No. 28. If prosthesis, is thisinitial placement?(If no, reason forreplacement)29. Date of priorplacement21. First visit datecurrent series22. Place of TreatmentOffice Hosp ECF Other23. Radiographs ormodels enclosed?No Yes Howmany?30. Is treatment fororthodontics?If services already commencedenter:Date appliances placed:Mos treatment remaining:31. Examination and treatment record—List in order from Tooth No.1 through Tooth No. 32Tooth #or LtrSurfacesDescription of Services(including X-rays, prophylaxis, materials used, etc.)Date SvsPerformedMo Day Yr.ADAProcedureCode #Fee forEach ServicePerformedReserved forProcessing UseI hereby certify that the procedures as indicated by date have been completed and hat he fees submitted are the actualfees I have charged and intend to collect for those procedures.TOTAL:Dentist’s SignatureDate
CLAIM FILING INSTRUCTIONSAny person who, with intent to defraud or knowing that he or she is facilitating a fraudagainst a benefits plan, submits an application or files a claim containing a false or deceptivestatement, is guilty of health care fraud.Help us to reduce health care costs by reporting health care fraud. Call 1-800-333-4585.TO THE MEMBER/EMPLOYEE:Complete all items in Blocks 1 thru 15 so that eligibility of the patient can be properlydetermined. (The Member/Employee’s or Authorized Person’s signature and the datesigned are required in the Release Authorization Section). After you complete the PatientSection, give the form to your dentist to fill out.If you have any questions about claims filing, call the Customer Service number onyour ID Card.TO THE DENTIST:Complete all items in Blocks 16 thru 31. (The Internal Revenue Service requires weidentify, record and report payments received from <strong>HealthSCOPE</strong> <strong>Benefits</strong>, Inc. Tocomply with this requirement, please furnish your Federal Tax Identification Number.)Mail completed claim forms to:<strong>HealthSCOPE</strong> <strong>Benefits</strong>P. O. Box 610409Dallas, TX 75261