KGH/HDH Data Request Form for Pulling Medical Records
KGH/HDH Data Request Form for Pulling Medical Records
KGH/HDH Data Request Form for Pulling Medical Records

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
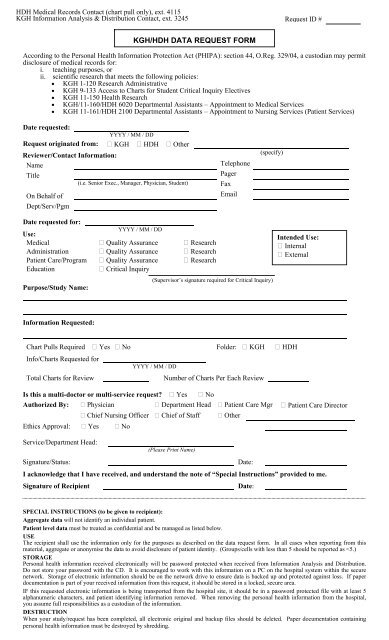
<strong>HDH</strong> <strong>Medical</strong> <strong>Records</strong> Contact (chart pull only), ext. 4115<strong>KGH</strong> In<strong>for</strong>mation Analysis & Distribution Contact, ext. 3245<strong>Request</strong> ID #<strong>KGH</strong>/<strong>HDH</strong> DATA REQUEST FORMAccording to the Personal Health In<strong>for</strong>mation Protection Act (PHIPA): section 44, O.Reg. 329/04, a custodian may permitdisclosure of medical records <strong>for</strong>:i. teaching purposes, orii. scientific research that meets the following policies:• <strong>KGH</strong> 1-120 Research Administrative• <strong>KGH</strong> 9-133 Access to Charts <strong>for</strong> Student Critical Inquiry Electives• <strong>KGH</strong> 11-150 Health Research• <strong>KGH</strong>/11-160/<strong>HDH</strong> 6020 Departmental Assistants – Appointment to <strong>Medical</strong> Services• <strong>KGH</strong> 11-161/<strong>HDH</strong> 2100 Departmental Assistants – Appointment to Nursing Services (Patient Services)Date requested:YYYY / MM / DD<strong>Request</strong> originated from: <strong>KGH</strong> <strong>HDH</strong> OtherReviewer/Contact In<strong>for</strong>mation:Name TelephoneTitlePager(i.e. Senior Exec., Manager, Physician, Student) FaxOn Behalf ofEmailDept/Serv/Pgm(specify)Date requested <strong>for</strong>:YYYY / MM / DDUse:<strong>Medical</strong> Quality Assurance ResearchAdministration Quality Assurance ResearchPatient Care/Program Quality Assurance ResearchEducation Critical InquiryPurpose/Study Name:(Supervisor’s signature required <strong>for</strong> Critical Inquiry)Intended Use: Internal ExternalIn<strong>for</strong>mation <strong>Request</strong>ed:Chart Pulls Required Yes No Folder: <strong>KGH</strong> <strong>HDH</strong>Info/Charts <strong>Request</strong>ed <strong>for</strong>YYYY / MM / DDTotal Charts <strong>for</strong> ReviewNumber of Charts Per Each ReviewIs this a multi-doctor or multi-service request? Yes NoAuthorized By: Physician Department Head Patient Care Mgr Patient Care Director Chief Nursing Officer Chief of Staff OtherEthics Approval: Yes NoService/Department Head:(Please Print Name)Signature/Status:Date:I acknowledge that I have received, and understand the note of “Special Instructions” provided to me.Signature of RecipientDate:SPECIAL INSTRUCTIONS (to be given to recipient):Aggregate data will not identify an individual patient.Patient level data must be treated as confidential and be managed as listed below.USEThe recipient shall use the in<strong>for</strong>mation only <strong>for</strong> the purposes as described on the data request <strong>for</strong>m. In all cases when reporting from thismaterial, aggregate or anonymise the data to avoid disclosure of patient identity. (Groups/cells with less than 5 should be reported as
INTERNAL USE ONLY<strong>Data</strong> Source: Inpatient ICU <strong>KGH</strong> Day Surgery Waitlist <strong>HDH</strong> Regional Decision 1 SMOL Clinic Bed Occupancy Other Emergency Provincial Operating RoomService Site: (institution the service occurred)Time Period:<strong>Request</strong>ed: Fiscal/Calendar/Other (Circle)toFrequency: AdHoc Monthly Other Yearly Quarterly (specify)Delivered On:Revised On:Method of Delivery:YYYY / MM / DDYYYY / MM / DDEmail/CD/Floppy/Other(Please Circle)Delivered To:Password:Project Date:YYYY / MM / DDReport Generated By:File Name:File Location: