Patient Demographic Sheet - St. Joseph Medical Center
Patient Demographic Sheet - St. Joseph Medical Center
Patient Demographic Sheet - St. Joseph Medical Center

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
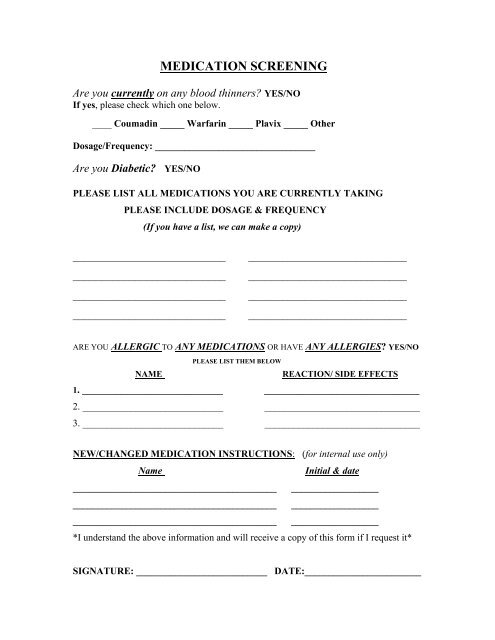
MEDICATION SCREENINGAre you currently on any blood thinners? YES/NOIf yes, please check which one below.____ Coumadin _____ Warfarin _____ Plavix _____ OtherDosage/Frequency: _________________________________Are you Diabetic? YES/NOPLEASE LIST ALL MEDICATIONS YOU ARE CURRENTLY TAKINGPLEASE INCLUDE DOSAGE & FREQUENCY(If you have a list, we can make a copy)____________________________________________________________________________________________________________________________________________________________________________________________________________________________ARE YOU ALLERGIC TO ANY MEDICATIONS OR HAVE ANY ALLERGIES? YES/NOPLEASE LIST THEM BELOWNAMEREACTION/ SIDE EFFECTS1. _____________________________ ________________________________2. _____________________________ ________________________________3. _____________________________ ________________________________NEW/CHANGED MEDICATION INSTRUCTIONS: (for internal use only)NameInitial & date__________________________________________ ____________________________________________________________ ____________________________________________________________ __________________*I understand the above information and will receive a copy of this form if I request it*SIGNATURE: ___________________________ DATE:________________________