CHAPTER 3 Infection <strong>and</strong> Inflammation 27tissue. Normally, the intact sulcular <strong>and</strong> junctionalepithelium serves as an effective naturalbarrier that keeps the bacteria from enteringhost tissues. However, severalperiodontopathogens (e.g., P. gingivalis, A.actinomycetemcomitans) have been shownto invade <strong>and</strong> transverse epithelial cells togain access to the connective tissue. Moreover,bacterial components (e.g., LPS, PGN)<strong>and</strong> products (e.g., proteases, toxins) that areeither shed or secreted can also diffusethrough the epithelial junctions to the connectivetissue. 9Bacteria in Connective TissueBacteria <strong>and</strong>/or their virulence factorsfound in the connective tissue directly stimulatehost cells residing in this area, includingleukocytes, fibroblasts, mast cells, endo -thelial cells, dendritic cells <strong>and</strong> lymphocytes.Neutrophils, macrophages, fibroblasts <strong>and</strong>mast cells release more proinflammatory cytokines(TNF-, IL-1, IL-6, IL-12), chemoattractants(IL-8, MIP-1- , MIP-2, MCP-1,MCP-5) <strong>and</strong> PGE 2in the connective tissue.In addition, degranulation of mast cells resultsin the secretion of histamine <strong>and</strong>leukotrienes further amplifying the inflammatorycascade. 10,11Mediators that are secreted from activatedhost cells (e.g., IL-1, TNF-, PGE 2,<strong>and</strong> histamine) will further assist bacterialvirulence factors in the activation of endo -thelial cells. This leads to secretion of morechemokines (IL-8, MCP-1) <strong>and</strong> expressionof adhesion molecules on the surface of endothelialcells, which are important forleukocyte extravasation (P- <strong>and</strong> E-selectinsas wells as ICAM-1 <strong>and</strong> -2). 12 Specifically,P- <strong>and</strong> E-selectins interact with glyco proteinson leukocytes allowing the cells to adhere reversiblyto the vessel wall, causing circulatingleukocytes to appear to “roll” along theactivated endothelium. Then, IL-8 <strong>and</strong> otherchemokines, bound to proteoglycans on thesurface of leukocytes, trigger a conformationalchange of integrins (LFA-1, CD11b:CD18). As a result, adhesive properties increasedramatically <strong>and</strong> leukocytes attachfirmly to ICAM-1 expressed on endothelialcells. TNF-, PGE 2<strong>and</strong> histamine increasevascular permeability, allowing leukocytesto squeeze between the endo thelial cells,thereby entering the connective tissue ina process known as diapedesis. Finally,chemokines, such as IL-8 that are producedat the site of infection <strong>and</strong> bind to proteoglycansof the extracellular matrix, alongwith bacterial chemo-attractants (fMLP,fimbriae) form a concentration gradient thatguides the leukocytes to migrate to the focusof infection.The Inflammatory CascadeNeutrophils are the first leukocytes toarrive followed by mononuclear phagocytesthat subsequently differentiate into macro -phages. The interaction of these cells withbacterial virulence factors induces further activation,which enhances their phagocytic activityby increasing the production of nitricoxide (NO) <strong>and</strong> the expression of complementreceptors (CR3). If the innate immuneresponse is successful, the bacteria are eliminated<strong>and</strong> resolution of inflammation follows.However, persistence of bacteria leadsto a chronic response characterized by extracelluarrelease of neutrophil granule contents,including degradative enzymes <strong>and</strong> reactiveoxygen species that spill into the extracellularmilieu, leading to local tissue damage <strong>and</strong>amplification of acute inflammatory signals. 13Pro-inflammatory cytokines (TNF-,IL-1, IL-6) from the site of inflammationenter the circulation <strong>and</strong> reach the liverwhere they activate hepatocytes. This leads,among other events, to the synthesis ofplasma proteins known as acute-phase proteins,including LPS binding protein (LBP)<strong>and</strong> CD14, which are important for therecognition of bacterial virulence factors.Complement proteins <strong>and</strong> C-reactive protein
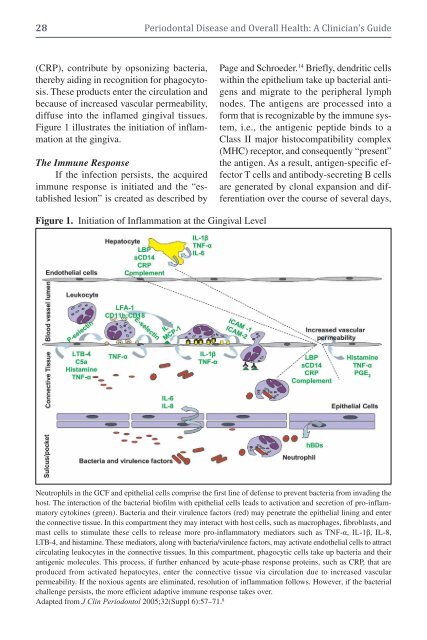
28 <strong>Periodontal</strong> <strong>Disease</strong> <strong>and</strong> <strong>Overall</strong> <strong>Health</strong>: A <strong>Clinician's</strong> <strong>Guide</strong>(CRP), contribute by opsonizing bacteria,thereby aiding in recognition for phagocytosis.These products enter the circulation <strong>and</strong>because of increased vascular permeability,diffuse into the inflamed gingival tissues.Figure 1 illustrates the initiation of inflammationat the gingiva.The Immune ResponseIf the infection persists, the acquiredimmune response is initiated <strong>and</strong> the “establishedlesion” is created as described byPage <strong>and</strong> Schroeder. 14 Briefly, dendritic cellswithin the epithelium take up bacterial antigens<strong>and</strong> migrate to the peripheral lymphnodes. The antigens are processed into aform that is recognizable by the immune system,i.e., the antigenic peptide binds to aClass II major histocompatibility complex(MHC) receptor, <strong>and</strong> consequently “present”the antigen. As a result, antigen-specific effectorT cells <strong>and</strong> antibody-secreting B cellsare generated by clonal expansion <strong>and</strong> differentiationover the course of several days,Figure 1. Initiation of Inflammation at the Gingival LevelNeutrophils in the GCF <strong>and</strong> epithelial cells comprise the first line of defense to prevent bacteria from invading thehost. The interaction of the bacterial biofilm with epithelial cells leads to activation <strong>and</strong> secretion of pro-inflammatorycytokines (green). Bacteria <strong>and</strong> their virulence factors (red) may penetrate the epithelial lining <strong>and</strong> enterthe connective tissue. In this compartment they may interact with host cells, such as macrophages, fibroblasts, <strong>and</strong>mast cells to stimulate these cells to release more pro-inflammatory mediators such as TNF-α, IL-1β, IL-8,LTB-4, <strong>and</strong> histamine. These mediators, along with bacteria/virulence factors, may activate endothelial cells to attractcirculating leukocytes in the connective tissues. In this compartment, phagocytic cells take up bacteria <strong>and</strong> theirantigenic molecules. This process, if further enhanced by acute-phase response proteins, such as CRP, that areproduced from activated hepatocytes, enter the connective tissue via circulation due to increased vascularpermeability. If the noxious agents are eliminated, resolution of inflammation follows. However, if the bacterialchallenge persists, the more efficient adaptive immune response takes over.Adapted from J Clin Periodontol 2005;32(Suppl 6):57–71. 8