Identifying the Newborns at Risk for Developing Significant ...
Identifying the Newborns at Risk for Developing Significant ...
Identifying the Newborns at Risk for Developing Significant ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ORIGINAL ARTICLEJ. Arab Neon<strong>at</strong>al Forum 2005; 2:81-85<strong>Identifying</strong> <strong>the</strong> <strong>Newborns</strong> <strong>at</strong> <strong>Risk</strong> <strong>for</strong> <strong>Developing</strong> <strong>Significant</strong>Hyperbilirubinemia by Measuring Cord Bilirubin LevelsRostami N 1 , Mehrabi Y 2Department of Pedi<strong>at</strong>rics, Taleghani Hospital, Shaheed Beheshti University of Medical Sciences , Tehran,Iran; 2 Department of Health and Community Medicine, Shaheed Beheshti University of Medical Sciences,Tehran, Iran.__________________________________________________________________________________________AbstractBackground: Jaundice is mostly benign, but because of <strong>the</strong> potential of bilirubin toxicity, neon<strong>at</strong>es should bemonitored carefully <strong>for</strong> developing severe hyperbilirubinemia. The need to recognize infants who are <strong>at</strong> risk <strong>for</strong>significant jaundice is apparent in <strong>the</strong> era of routine early discharge. The aim of this prospective study is toidentify healthy newborns <strong>at</strong> risk <strong>for</strong> developing significant hyperbilirubinemia by measuring bilirubin level incord blood. Methods: Umbilical cord serum bilirubin concentr<strong>at</strong>ion was analyzed in 643 full term infants withbirth weight ≥ 2500 grams and an Apgar score ≥ 7, born <strong>at</strong> Mahdieh Hospital, Tehran, Iran. Infants with signs ofecchymosis, cephalohem<strong>at</strong>oma, septicemia, and/or prem<strong>at</strong>ure rupture of membrane were excluded from <strong>the</strong>study. Serum bilirubin level was obtained <strong>at</strong> day three of age and total bilirubin ≥ 239µmol/l (14 mg/dl) wasdefined as significant hyperbilirubinemia. D<strong>at</strong>a were analyzed using t-test, chi-square, and Receiver Oper<strong>at</strong>ingCharacteristics (ROC) curve. Results: Mean and standard devi<strong>at</strong>ion of cord bilirubin level was 34.2 ± 15.9µmol/l (2.00 ± 0.93 mg/dl). There was a st<strong>at</strong>istically significant rel<strong>at</strong>ion between use of oxytocin and subsequentsignificant hyperbilirubinemia (p < 0.04). 92.4% of neon<strong>at</strong>es with cord bilirubin levels below 51.3 µmol/l (3mg/dL) did not develop significant hyperbilirubinemia. A cord serum bilirubin level above 51.3 µmol/l is not auseful predictor of neon<strong>at</strong>al jaundice. Conclusion: Cord serum bilirubin levels cannot identify newborns withsubsequent significant hyperbilirubinemia. Early discharged neon<strong>at</strong>es need close follow-up and use of any o<strong>the</strong>rstr<strong>at</strong>egies to identify newborns <strong>at</strong> high risk of jaundice.Keywords: Hyperbilirubinemia, cord bilirubin, neon<strong>at</strong>es.IntroductionHyperbilirubinemia is a common problem during <strong>the</strong>neon<strong>at</strong>al period and is <strong>the</strong> most common reason <strong>for</strong>readmission after early hospital discharge. It can be aphysiologic condition or a severe disease with braindamage. 1-4 Hyperbilirubinemia is quite common innewborns; it affects nearly 70% of term and 80% ofpreterm neon<strong>at</strong>es during <strong>the</strong> first week of life 5 . Theimportant risk factors most frequently associ<strong>at</strong>ed withsever hyperbilirubinemia are breast feeding,gest<strong>at</strong>ional age below 38 weeks, significant jaundicein a previous sibling, and jaundice noted be<strong>for</strong>edischarge 6 .Early newborn discharge began as a consumeriniti<strong>at</strong>edmovement and as an altern<strong>at</strong>ive to homedelivery in <strong>the</strong> 1980’s. Reports of recent experienceswith early discharge show both problems and successwith this policy. 7 A short hospital stay, <strong>for</strong> less than48 hours after birth, resulted in an increase inneon<strong>at</strong>al readmission <strong>for</strong> hyperbilirubinemia. TheAmerican Academy of Pedi<strong>at</strong>rics (AAP) recommendsth<strong>at</strong> newborns discharged within 48 hours shouldDr. Nahid Rostami, Department of Pedi<strong>at</strong>rics,Neon<strong>at</strong>ology Division, Taleghani Hospital,Shaheed Beheshti University of Medical Sciences,Evin, Tehran, 19857, Iran, E-mail:Rostami@sbmu.ac.ir , neon<strong>at</strong>al_sbmu@yahoo.com ,Phone: +98 21 2240 3583, Fax: +98 21 4417 0550have a follow up visit after 2-3 days to detectsignificant jaundice and o<strong>the</strong>r problems. 8 Bilirubintoxicity remains a significant problem despite recentadvances in <strong>the</strong> care of jaundiced neon<strong>at</strong>es. 9Kernicterus, though infrequent, is <strong>the</strong> cause of 10%of mortalities and <strong>at</strong> least 70% of long-termmorbidities among newborns. 10 Recent increases inearly hospital discharges, coupled with a rise inbreast feeding r<strong>at</strong>es, has led to a rise in <strong>the</strong> r<strong>at</strong>e ofpreventable kernicterus resulting from undetectedhyperbilirubinemia. If extreme hyperbilirubinemiacan be prevented, <strong>the</strong>n almost all cases of kernicterusare avoidable too. Asian and Middle Eastern infantsgenerally have higher total serum bilirubin (TSB)levels, and <strong>the</strong>y are more often breast-fed. There<strong>for</strong>e,it is essential to identify infants <strong>at</strong> high risk <strong>for</strong>developing p<strong>at</strong>hologic jaundice in <strong>the</strong>se regions.In recent years many ef<strong>for</strong>ts have been made toidentify infants likely to develop neon<strong>at</strong>al jaundice.Reliable str<strong>at</strong>egies can reduce hospital stay <strong>for</strong>normal babies and identify significanthyperbilirubinemia th<strong>at</strong> may happen in <strong>the</strong> future.Universal follow-up within 1 to 2 days of earlydischarge, umbilical cord bilirubin concentr<strong>at</strong>ion <strong>at</strong>birth, routine pre-discharge serum bilirubin andtranscutaneous bilirubin measurement, as well as <strong>the</strong>universal clinical assessment <strong>for</strong> risk factors ofdeveloping jaundice are various str<strong>at</strong>egies to predictsignificant hyperbilirubinemia.81
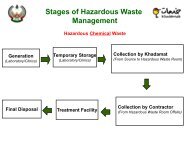
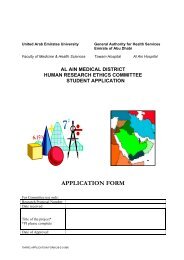
Cord bilirubin level and risk <strong>for</strong> hyperbilirubinemiaIn Iran, due to cultural issues, it is difficult to provideand monitor compliance of a follow-up program <strong>for</strong>every infant who is discharged. There<strong>for</strong>e, it isimpossible to use hour-specific bilirubin percentile topredict subsequent jaundice. The present study wasconducted to evalu<strong>at</strong>e <strong>the</strong> ability of cord bilirubinlevel in identifying healthy term infants <strong>at</strong> risk ofhyperbilirubinemia.M<strong>at</strong>erials and MethodsThe total annual numbers of births in <strong>the</strong> hospital, inTehran, and in Iran are approxim<strong>at</strong>ely 5,000, 178,100and 1,171,573 (based on <strong>the</strong> 2003 report of <strong>the</strong>St<strong>at</strong>istical Center of Iran) respectively. According toprevious studies about 18% of infants had TSB of 14and above. Assuming 3% error and 95% confidence,<strong>the</strong> sample size was worked out as 630 infants.System<strong>at</strong>ic random sampling was used to select <strong>the</strong>subjects. Over a period of 6 months 740 mo<strong>the</strong>rswere approached of whom 97 refused to particip<strong>at</strong>ein <strong>the</strong> study. The popul<strong>at</strong>ion of this study <strong>the</strong>re<strong>for</strong>eincluded 643 (343 females and 300 males) healthyfull term newborns delivered <strong>at</strong> Mahdieh Hospital,Tehran, Iran. All infants had gest<strong>at</strong>ional age of > 37weeks (based on New Ballard Score), and birthweight ≥ 2500 grams. Also <strong>the</strong>re were no signs ofcephalohem<strong>at</strong>oma, prolonged rupture of membrane(more than 24 hours), septicemia and significantillness with a fifth minute Apgar score ≥7.Frequency1008060402001471013Total Bilirubin (3rd day)Figure 1: Histogram of 3 rd day total serum bilirubinconcentr<strong>at</strong>ionSensitivity1.00.75.50161922The umbilical cord bilirubin level <strong>at</strong> birth and TSBlevels in all infants on day 3 of life were measured.In<strong>for</strong>med consent was also obtained from all <strong>the</strong>parents. Blood group and G6PD activity tests wereper<strong>for</strong>med routinely in all cases. All infants werevisited daily by a pedi<strong>at</strong>rician and were dischargedafter 72 hours. Bilirubin levels were obtained if <strong>the</strong>newborn was clinically diagnosed as being jaundicedbe<strong>for</strong>e 72 hours. <strong>Significant</strong> hyperbilirubinemia wasdefined <strong>at</strong> TSB level of ≥ 239 µmol/l (14 mg/dl) onday 3 of life. The infants were investig<strong>at</strong>ed andsupervised if <strong>the</strong>y were clinically jaundiced on <strong>the</strong>first day of life, if TSB was ≥ 205 µmol/l (12mg/dl)on day 2, and TSB ≥ 239 µmol/l (14 mg/dl) on day 3.M<strong>at</strong>ernal and neon<strong>at</strong>al d<strong>at</strong>a were also collected. D<strong>at</strong>awere analyzed using descriptive st<strong>at</strong>istics, chi-square,and t-tests. Sensitivity, specificity, and positive andneg<strong>at</strong>ive predictive values of different cut-points of<strong>the</strong> cord total bilirubin were obtained. ReceiverOper<strong>at</strong>ing Characteristics (ROC) curve analysis wascarried out to evalu<strong>at</strong>e <strong>the</strong> usefulness of cordbilirubin level <strong>for</strong> identifying neon<strong>at</strong>es <strong>at</strong> risk.ResultsA total of 643 newborns were enrolled. Baselinecharacteristics of infants and <strong>the</strong>ir mo<strong>the</strong>rs are shownin Table 1. All infants were exclusively breast-fed.<strong>Significant</strong> hyperbilirubinemia was detected in 11.8%of infants. Figure 1 shows <strong>the</strong> distribution of serumbilirubin concentr<strong>at</strong>ion on <strong>the</strong> third day..250.000.00.25.501 - SpecificityFigure 2: Receiver Oper<strong>at</strong>ing Characteristics (ROC) curveof cord bilirubin <strong>for</strong> predicting 3 rd day bilirubin(≥14). Area under curve = 0.563 (95% CI:0.490, 0.636).Bilirubin level more than 239 µmol/l (14 mg/dl) wereobserved in 16.9% of infants whose mo<strong>the</strong>rs hadreceived oxytocin during delivery, and in 10.6 % ofinfants whose mo<strong>the</strong>rs had not received it (p < 0.04).<strong>Significant</strong> hyperbilirubinemia was detected in 14.3%of G6PD deficient infants as against 11.8% of nonenzymedeficient infants, <strong>the</strong> difference not beingsignificant. The incidence of ABO incomp<strong>at</strong>ibilitywas 12%, and 15.6 % of <strong>the</strong>se infants had p<strong>at</strong>hologicjaundice. The incidence of Rh incomp<strong>at</strong>ibility was6.2% and significant hyperbilirubinemia developed in10% of infants in this group. In infants with ABO andRh incomp<strong>at</strong>ibilities, third day total bilirubin levelwas not significantly different from o<strong>the</strong>r babies of<strong>the</strong> studied group (table 2). <strong>Significant</strong>hyperbilirubinemia developed in 13.4% of boys and10.6% of girls..751.0082
J. Arab Neon<strong>at</strong>al Forum 2005; 2:81-85There were no significant rel<strong>at</strong>ions between type ofdelivery, sex, birth weight, history of jaundice ino<strong>the</strong>r siblings, instrumental delivery, parity, m<strong>at</strong>ernalage and p<strong>at</strong>hologic jaundice on 3rd day. As shown in<strong>the</strong> ROC curve (Figure 2) <strong>the</strong> cord bilirubin level isnot an appropri<strong>at</strong>e index <strong>for</strong> identifying high riskneon<strong>at</strong>es. Sensitivity, specificity, positive andneg<strong>at</strong>ive predictive values of cord bilirubin level <strong>for</strong>prediction of p<strong>at</strong>hologic jaundice are shown in Table3.DiscussionThere is a concern about an increasing incidence ofkernicterus in healthy term neon<strong>at</strong>es, andhyperbilirubinemia is one of <strong>the</strong> most commonreasons <strong>for</strong> readmission of newborns especially in <strong>the</strong>Middle East and Asia. The need <strong>for</strong> early detection ofhyperbilirubinemia in newborns discharged earlyfrom <strong>the</strong> hospital is <strong>the</strong>re<strong>for</strong>e important. Knowledgeof infants <strong>at</strong> risk of developing jaundice allowssimple bilirubin reducing methods to be implementedbe<strong>for</strong>e bilirubin levels reach critical levels. Earlyhospital discharge policy in developing countriessuch as Iran, along with limited follow up facilities,and inadequ<strong>at</strong>e communic<strong>at</strong>ion between physiciansand parents, necessit<strong>at</strong>e a prognostic test to predictand prevent a potential problem be<strong>for</strong>e it occurred.In this study, we assessed <strong>the</strong> ability of cord bilirubinlevel to be a tool <strong>for</strong> screening <strong>for</strong> <strong>the</strong> risk ofsubsequent significant neon<strong>at</strong>al jaundice.The present study shows th<strong>at</strong> 92.4% of infants withcord bilirubin level below 3 mg/dl would notpotentially develop significant hyperbilirubinemia.There are conflicting reports of <strong>the</strong> predictability ofcord blood bilirubin of l<strong>at</strong>er hyperbilirubinemia.Rosenfeld 11 showed th<strong>at</strong> infants with cord bilirubinlevels less than 34 µmol/l have only 4 percent chanceof developing hyperbilirubinemia and 1.4 percentchance of needing photo<strong>the</strong>rapy. However, infantswith cord bilirubin > 34µmol/l would have 25 percentchance of developing subsequent hyperbilirubinemia.Knudsen 12 showed if cord bilirubin was below 20.5µmol/l, 2.9% of infants developed jaundiced asopposed to 85% if cord bilirubin was above 43µmol/l. Fur<strong>the</strong>rmore, 57% of jaundiced infants withcord bilirubin above 43µmol/l required photo<strong>the</strong>rapy.In ano<strong>the</strong>r retrospective study, Jacobson et al. 13compared cord bilirubin levels of 87 neon<strong>at</strong>es whoreceived standard photo<strong>the</strong>rapy <strong>for</strong> neon<strong>at</strong>al jaundicewith <strong>the</strong> cord bilirubin levels of 95 neon<strong>at</strong>es withoutneon<strong>at</strong>al jaundice. There were no significantdifferences in <strong>the</strong> cord bilirubin levels between <strong>the</strong>two groups leading to <strong>the</strong> conclusion th<strong>at</strong> cordbilirubin levels could not predict significanthyperbilirubinemia. Simpson et al 5 reported th<strong>at</strong> cordbilirubin levels above 43µmol/l can predictdevelopment of p<strong>at</strong>hologic jaundice (TSB > 222µmol/l) with sensitivity and specificity of 71% and96% respectively, while Carbonell et al 14 showedumbilical cord bilirubin with cut-off point of 38µmol/l was not a useful predictor of neon<strong>at</strong>aljaundice.Table 1- Characteristics d<strong>at</strong>a of enrolled infants and <strong>the</strong>ir mo<strong>the</strong>rsCharacteristics3 rd day serum bilirubin< 14 ≥ 14 TotalNumber (%) 567 (88.2) 76 (11.8) 643Birth weight (mean ± sd) 3158 ± 515 3134 ± 456 3155 ± 508Cord bilirubin (mean ± sd)Total (µmol/l) 34 ± 16 37.4 ± 17 14 ± 16Direct (µmol/l) 4.6 ± 6 4.1 ± 3.2 4.4 ± 6Age of mo<strong>the</strong>r (mean ± sd ; yrs) 26.0 ± 5.7 26.6 ± 3.2 26.1 ± 5.8Parity (mean ± sd) 1.6 ± 1.5 1.4 ± 1.7 1.5 ± 1.5Table 2. Occurrence of significant hyperbilirubinemia in different groupsVariablesPercentage of significant hyperbilirubinemiaYesNoABO incomp<strong>at</strong>ibilty * 15.6 11.3Rh incomp<strong>at</strong>ibility ** 10.0 11.9G6PD deficiency 14.3 11.8History of jaundice in siblings 23.8 11.6Intran<strong>at</strong>al administr<strong>at</strong>ion of oxytocin 16.9 † 10.6Neon<strong>at</strong>al sexBoys 13.4Girls 10.6*Mo<strong>the</strong>r’s blood group O, neon<strong>at</strong>e’s blood group A or B , **Mo<strong>the</strong>r’s Rh- and neon<strong>at</strong>e’s Rh+ † P< 0.04, ‡ Caesarian section83
Cord bilirubin level and risk <strong>for</strong> hyperbilirubinemiaTable 3: Sensitivity, specificity, positive and neg<strong>at</strong>ive predictive values of cord bilirubin level <strong>for</strong> prediction of 3rd daysignificant hyperbilirubinemiaCord bilirubincut-off pointsSensitivity SpecificityPositivepredictive value1 93.4 4.1 11.5 82.11.5 85.5 20.3 12.6 91.32 59.2 48.1 13.3 89.82.5 25 84.1 17.4 89.33 18.4 92.4 24.6 89.43.5 13.2 95.9 30.3 89.24 7.9 97.7 31.6 88.8Neg<strong>at</strong>ivepredictive valueBernalda and Segre 15 reported th<strong>at</strong> bilirubin levels incord blood were significantly higher in newborns th<strong>at</strong>had required photo<strong>the</strong>rapy. The presence of ABOblood group incomp<strong>at</strong>ibility was a significantvariable in rel<strong>at</strong>ion to <strong>the</strong> need <strong>for</strong> photo<strong>the</strong>rapy. Themost useful cutoff point <strong>for</strong> unconjug<strong>at</strong>ed bilirubin incord blood was 34 µmol/l. They declared th<strong>at</strong> 53% ofnewborns who had gre<strong>at</strong>er bilirubin levels in cordblood would reach levels requiring photo<strong>the</strong>rapy by<strong>the</strong> third day of life.<strong>Risk</strong>in et al 16 st<strong>at</strong>ed th<strong>at</strong> <strong>the</strong> trained human eye canstill discrimin<strong>at</strong>e between <strong>the</strong> jaundiced and nonjaundicednewborn, and clinical impression ofjaundice remains a reliable primary screening tool <strong>for</strong>significant neon<strong>at</strong>al hyperbilirubinemia. Percentilecharts of serum bilirubin levels <strong>at</strong> different postn<strong>at</strong>alages in near-term and term infants have beenproduced. 17 An hour specific TSB, be<strong>for</strong>e hospitaldischarge, can predict newborns <strong>at</strong> high,intermedi<strong>at</strong>e, or low risk <strong>for</strong> developing clinicallysignificant hyperbilirubinemia (defined as TSB > 95 thpercentile <strong>for</strong> age in hours). Agarwal et al 18 showedth<strong>at</strong> TSB level of 103 µmol/l <strong>at</strong> 24 ± 6 hours of lifepredicts absence of subsequent hyperbilirubinemiawith high probability.A model based on several factors can be used topredict neon<strong>at</strong>al jaundice and shows a sensitivity of81% and specificity of 82.9%, a false positive r<strong>at</strong>e of80.2% and a false neg<strong>at</strong>ive r<strong>at</strong>e of 1.1%. Individualrisk assessment could be made based on day one totalserum bilirubin. L<strong>at</strong>er, Sarici et al 20 concluded anearly six-hour serum bilirubin measurement wasuseful in predicting <strong>the</strong> development of significanthyperbilirubinemia in newborns with ABOincomp<strong>at</strong>ibility. The American Academy ofPedi<strong>at</strong>rics (AAP) produced a clinical practiceguideline <strong>for</strong> <strong>the</strong> management of hyperbilirubinemiain healthy term newborns. 6 The AAPrecommend<strong>at</strong>ion requires th<strong>at</strong> every infant beassessed <strong>for</strong> <strong>the</strong> risk of developing severehyperbilirubinemia and all nurseries to establish aprotocol <strong>for</strong> assessing this risk be<strong>for</strong>e discharge from<strong>the</strong> hospital. The AAP recommends two clinicaloptions used individually or in combin<strong>at</strong>ion <strong>for</strong> <strong>the</strong>system<strong>at</strong>ic assessment of risk: pre-dischargemeasurement of <strong>the</strong> bilirubin level using TSB ortranscutaneous bilirubin level (TcB), and/orassessment of clinical risk factors. Whe<strong>the</strong>r ei<strong>the</strong>r orboth options are used, appropri<strong>at</strong>e follow-up afterdischarge is essential. TSB can be obtained <strong>at</strong> <strong>the</strong>time of <strong>the</strong> routine metabolic screen. Some authorshave suggested th<strong>at</strong> a TSB measurement should bepart of <strong>the</strong> routine screening of all newborns. Aninfant whose pre discharge TSB is in <strong>the</strong> low-riskzone is <strong>at</strong> very low risk of developing severhyperbilirubinemia. The incidence of ABOincomp<strong>at</strong>ibility in <strong>the</strong> present study was 12% whichis consistent with results from o<strong>the</strong>r studies. 20In <strong>the</strong> present study oxytocin was used in 39.4% ofmo<strong>the</strong>rs and 16.9% of <strong>the</strong>ir babies had p<strong>at</strong>hologicjaundice. There was a significant rel<strong>at</strong>ionshipbetween usage of oxytocin and p<strong>at</strong>hologic jaundice(p < 0.04). The incidence of p<strong>at</strong>hologichyperbilirubinemia was 11.8% in this study. Theseresults are in good agreement with those of o<strong>the</strong>rinvestig<strong>at</strong>ors like Alpay 21 who reported th<strong>at</strong> 12.5% ofnewborns had significant jaundice after 72 hours oflife, and Agarwal et al. who showed th<strong>at</strong>hyperbilirubinemia occurred in 10.3% of infants.In <strong>the</strong> present study, our infants were followed up <strong>for</strong>up to <strong>the</strong> third day of life. Infants without significantclinical jaundice were not followed subsequently.There<strong>for</strong>e, infants who might have developed l<strong>at</strong>ejaundice could have been missed. G6PD deficiency ismore common in <strong>the</strong> Middle East 6 but in <strong>the</strong> presentstudy G6PD deficiency was only 2.2%.ConclusionIt can be concluded th<strong>at</strong>, cord bilirubin levels can notidentify newborn infants who are <strong>at</strong> risk <strong>for</strong>developing significant hyperbilirubinemia. However,cord bilirubin level below 3 mg/dl identified thoseinfants who are not high risk to develop p<strong>at</strong>hologicjaundice.In Iran due to economical factors, early hospitaldischarge is a routine practice. TSB measurement inhealthy term newborns is not an option because84