

Community-Based Surveillance of Antimicrobial Use and ...
Community-Based Surveillance of Antimicrobial Use and ...
Community-Based Surveillance of Antimicrobial Use and ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
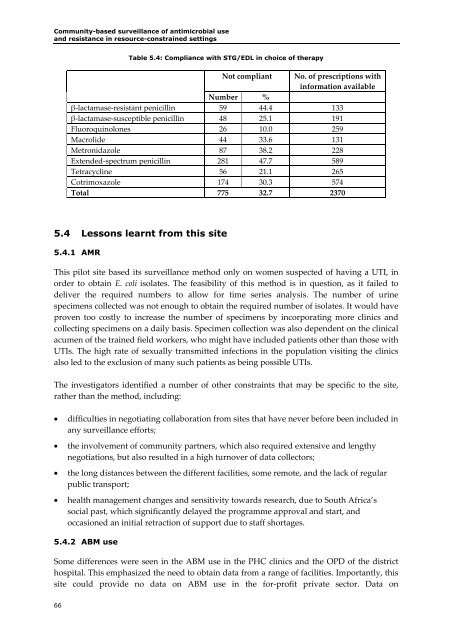
<strong>Community</strong>-based surveillance <strong>of</strong> antimicrobial use<strong>and</strong> resistance in resource-constrained settingsTable 5.4: Compliance with STG/EDL in choice <strong>of</strong> therapyNot compliant No. <strong>of</strong> prescriptions withinformation availableNumber %β‐lactamase‐resistant penicillin 59 44.4 133β‐lactamase‐susceptible penicillin 48 25.1 191Fluoroquinolones 26 10.0 259Macrolide 44 33.6 131Metronidazole 87 38.2 228Extended‐spectrum penicillin 281 47.7 589Tetracycline 56 21.1 265Cotrimoxazole 174 30.3 574Total 775 32.7 23705.4 Lessons learnt from this site5.4.1 AMRThis pilot site based its surveillance method only on women suspected <strong>of</strong> having a UTI, inorder to obtain E. coli isolates. The feasibility <strong>of</strong> this method is in question, as it failed todeliver the required numbers to allow for time series analysis. The number <strong>of</strong> urinespecimens collected was not enough to obtain the required number <strong>of</strong> isolates. It would haveproven too costly to increase the number <strong>of</strong> specimens by incorporating more clinics <strong>and</strong>collecting specimens on a daily basis. Specimen collection was also dependent on the clinicalacumen <strong>of</strong> the trained field workers, who might have included patients other than those withUTIs. The high rate <strong>of</strong> sexually transmitted infections in the population visiting the clinicsalso led to the exclusion <strong>of</strong> many such patients as being possible UTIs.The investigators identified a number <strong>of</strong> other constraints that may be specific to the site,rather than the method, including:• difficulties in negotiating collaboration from sites that have never before been included inany surveillance efforts;• the involvement <strong>of</strong> community partners, which also required extensive <strong>and</strong> lengthynegotiations, but also resulted in a high turnover <strong>of</strong> data collectors;• the long distances between the different facilities, some remote, <strong>and</strong> the lack <strong>of</strong> regularpublic transport;• health management changes <strong>and</strong> sensitivity towards research, due to South Africa’ssocial past, which significantly delayed the programme approval <strong>and</strong> start, <strong>and</strong>occasioned an initial retraction <strong>of</strong> support due to staff shortages.5.4.2 ABM useSome differences were seen in the ABM use in the PHC clinics <strong>and</strong> the OPD <strong>of</strong> the districthospital. This emphasized the need to obtain data from a range <strong>of</strong> facilities. Importantly, thissite could provide no data on ABM use in the for‐pr<strong>of</strong>it private sector. Data on66

