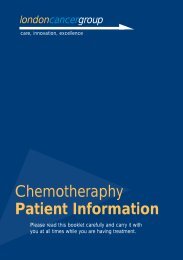
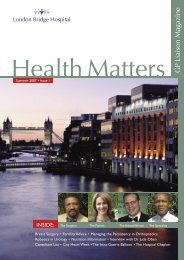
Breast Deformity | CholecystectomyTubular BreastDeformityMr Roy Ng is a consultant plastic surgeon at Guy’s and StThomas’ <strong>Hospital</strong>s NHS Trust, and at <strong>London</strong> <strong>Bridge</strong> <strong>Hospital</strong>.He has extensive experience in reconstructive and aestheticsurgery of the breast, including postmastectomy, developmentaland postpregnancy deformities. He has a particular interestin the developmental problem of Tubular Breasts. Here, hedescribes the condition and approaches to its management.The diagnosis of Tubular Breast Deformity can go unrecognisedby patients and some doctors, with the condition simplyassumed to be ‘small’ breasts. However, it is a specificdevelopmental abnormality that can cause great distress to theindividual and impact greatly on their psychosocial functioning.The characteristic features of this deformity are a narrow breast base associatedwith a large and herniated nipple-areola complex. As a consequence, the shapeof the breast resembles more a ‘tube’ than a mound. Other terms that have beenapplied to this condition include ‘tuberous breast’, ‘constricted breast’ and even‘Snoopy breast deformity’. There is a spectrum of severity, and one proposedclassification by Heimburg et al 1 is illustrated in Figure 1.Figure 1. Classification of Tuberous Breast DeformityCounselling and TreatmentNew techniquefor operation ofCholecystectomyMr Marshall, a laparoscopic and Upper GIsurgeon, who has been with NewhamUniversity <strong>Hospital</strong> NHS Trust for threeyears, has pioneered a new technique forCholecystectomy operations over the last18 months. An honorary Consultant Surgeonwith Bart’s and <strong>London</strong> Trust, and HonorarySenior Lecturer at the Institute of Cancerat Charterhouse Square, Mr Marshall hasrecently joined the <strong>London</strong> <strong>Bridge</strong> <strong>Hospital</strong>and will be offering this procedureto patients who require aCholecystectomy.The technique employs an ultrasonicdissector (or Harmonic scalpel) asthe sole instrument for dissectionand sealing of the cystic artery andduct. The operation is performed ina retrograde, or fundus first, mannerwhich enhances the display of the anatomyand allows the surgeon to see the operativefield more clearly. The use of the Harmonicscalpel eliminates the need for electrosurgeryin this operation; which is a further benefit tothe patient because of the concerns regardinginadvertent injury to abdominal structuresand ‘smoke’ production. The techniqueenables more than 90% of patients who haveundergone this type of Cholecystectomy, togo home the same day as their surgery. As aresult of this rapid recovery, the techniquehas been selected for presentation at threeinternational meetings over the last 12 months.This unique operative technique hasPatients with Tubular Breast Deformity are often extremely self-conscious at thetime of examination, and must be handled with great sensitivity and patience.They are often relieved when informed that there is a specific diagnosis, andoverjoyed when informed that effective treatment is possible.The deformity is readily corrected surgically. By means of a periareolar incision,the breast base is widened, volume is increased by insertion of a breast implant,and the nipple-areola herniation is corrected by a ‘doughnut’ mastopexy. Thescars are confined to the areolar border, and therefore quite inconspicuous(Figure 2).significantly improved the recoveryperiod and improved the patients’experiences during this historicallyunpleasant procedure. Mr Marshall is anexperienced laparoscopic surgeon; using thisdynamic technique for hernia repairs, bothinguinal and incisional, surgery for refluxdisease, bowel surgery and obesity treatment.The Department of <strong>Health</strong> has picked upon this technique and is looking to useit as the standard for ‘best practice’ forCholecystectomy surgery.Images: Ethicon Endo-Surgery, a divisionof Johnson & Johnson Medical Limited hasprovided the supporting images. However,it is not responsible for any editorial material.8Figure 2. Preoperative and postoperative photographs of a patient withBilateral Tubular Breast Deformity, left more severe than the right.References1Heimburg v.D., Exner K., Kruft S. and Lemperle G. The Tuberous Breast Deformity:Classification and Treatment. British Journal of Plastic Surgery (1996), 49, 339-345.Mr Roy L. H. Ng, MA DM FRCS (Plast)Consultant Plastic Surgeon<strong>London</strong> <strong>Bridge</strong> <strong>Hospital</strong>www.royng.co.ukMr Marshall
A liver resection is anoperation to remove a partof your liver. It is usuallyperformed because the liverhas one or more tumours init. The liver is one of the feworgans in the body that is ableto re-grow. Up to 80% of theliver can be removed, and thehealthy liver will re-grow inapproximately 8-12 weeks.Mr Parthi SrinivasanLaparoscopic Liver SurgeryLiver Surgeryat <strong>London</strong> <strong>Bridge</strong> <strong>Hospital</strong>Why do I need this operation?You need this operation because it is the mosteffective way of removing the tumour(s) in yourliver.What are the likely benefits?Surgical removal of the tumour(s) offers the onlypotential cure. The intended benefit is that theoperation will extend your life expectancy; thatis, you will live longer having had the operationthan if you do not.How is the operation performed?Liver surgery is traditionally performed by anopen operation through an incision that oftenspreads across both sides of the upper part ofthe abdomen. We first disconnect the bloodsupply to the part of the liver that carries thetumour(s). We then cut through the liver usingspecial devices that help us minimise the bloodloss during the surgery, although sometimes ablood transfusion may be required.More recently, liver tumours have been safely andsuccessfully removed by ‘keyhole’ (laparoscopic)surgery. However, laparoscopic surgery is notsuitable for all patients. This is for a number ofreasons including, not all tumours can be removedby laparoscopic surgery, you may have othermedical conditions or you may have had previousabdominal surgery.In principle, laparoscopic liver resection is thesame as an open operation, but is performedthrough smaller cuts. Whenever we do alaparoscopic operation, however, there is a chancethat we may need to convert to a traditional openoperation, if faced with a difficulty that we cannotovercome by laparoscopic surgery. The chance ofa conversion to open surgery may be as highas 1 in 10 patients (10%). Laparoscopic surgeryis carried out through a few small cuts on theabdomen, with the use of gas (carbon dioxide)to inflate the abdomen. The operation is thenperformed using a special camera to visualise theliver, and special instruments. Sometimes, one ofthe cuts is made longer than others in order forthe surgeon to place one hand in the abdomento help with the surgery (this is called hand-assistedlaparoscopic surgery) and through which thesurgeon finally removes the resected part ofthe liver.For both types of liver surgery, after the tumourshave been removed a glue-like substance is usuallypoured or sprayed onto the liver to help preventbleeding after the operation. Everything is carefullychecked and then the incision is closed with severallayers of stitching.Before any surgery, open or laparoscopic, theteam will assess your clinical condition and reviewyour scans to determine how your tumour(s)could be best removed. All your tests andscans will be reviewed by a team of doctors(the multidisciplinary team), which includesyour consultant. The team will recommend thetreatment it feels will be best for you. Obviously,this recommendation will be thoroughly discussedwith you before a final decision about treatmentis made.If it was not clear from your radiology test orother scans, whether the tumour is removable,your surgeon may carry out a diagnostic test calleda laparoscopy (key-hole operation) to evaluatethe tumour further. If this shows that the tumourhas spread outside of the liver or bile ducts, thesurgeon will not carry out the formal resection.What are the risks?Some risks are common to all operations, suchas chest infection and blood clots forming in yourveins (DVT) or in the lungs (pulmonary embolus).However, there are also specific risks associatedwith liver surgery:1. Bleeding: the liver is well supplied with bloodand one of the major risks of liver surgeryis bleeding. You will lose blood during theoperation and this will be replaced with bloodtransfusions as required. Occasionally, bleedingcan occur after the operation and a furtheroperation may be necessary to stop this.Specific blood will be kept ready for you,should you need a transfusion.Transfusion itself carries some risks and wouldnot be given, except when absolutely necessary.If you have any objections to receiving bloodor blood products (such as platelets), it isessential that you inform your surgeon and/oranaesthetist before your operation.2. Bile leak: the liver can leak bile from whereit has been cut. If your liver does leak bile inthis way, then other procedures may berequired to control this. The reconnections(or anastomoses) that the surgeon createsduring the operation can sometimes leak,and if this happens, then further drains (todrain the leaking fluid to the outside) maybe necessary. If this happens, you may needto return to theatre for further surgery,although this is rarely necessary.3. Liver decompensation: if your tumour(s) arelarge or dispersed within the liver, then a largepart of your liver may have to be removed.This will leave your body with a much smalleramount of liver. As explained earlier, in timethis liver will re-grow to take the place of theliver that has been removed. However, in theshort-term after the operation, your smallerliver may struggle to do all that it is meant to.The symptoms of this can be jaundice (yourskin becomes yellow) and a build up of fluidin your abdomen. These problems will usuallysettle down after a week or two. In a very smallnumber of patients, this may be associated withother organs not functioning properly, such aslow blood pressure, pneumonia and kidneyfailure.4. Infection: this may involve the wound, the drainsites or the inner organs. Antibiotics will be givento you at the time of surgery to try to preventan infection developing.5. Advanced disease: as noted earlier, sometimesit is not clear from radiology or other scanswhether or not the tumour is removable. It maynot be until you are actually on the operatingtable that it is discovered that the tumourcannot be removed.What happens before the operation?Once surgery has been agreed with you as thefavoured option, you will be asked to attend a preassessmentclinic to assess your fitness for surgeryand answer questions. This usually takes half a day;during this, the operation will be explained in detailand informed consent will be taken from you forthe procedure. An anaesthetist will explain theanaesthetic process and discuss the post-operativepain relief options. This is usually in the form ofepidural analgesia, where a small tube is insertedinto your back to deliver the pain relieving drugs.Alternatively, a patient control analgesia pump (orPCA) will be offered. A PCA allows you to controlyour own dosage of pain relief, delivered througha drip in your arm, by pressing a small button.Please use this opportunity to ask the surgeons,nurses or anaesthetists any questions that you have.On admission, you will be given information aboutthe expected date of your discharge from hospital.This is to help you, and the staff caring for you, toplan and prepare for your return home.The day before the operation, you must not eator drink anything after midnight as your stomachneeds to be as empty as possible for the generalanaesthetic you will be given for this operation. Thismay be given to you when you are in the operatingtheatre itself, so don’t worry if you are still awakewhen you are first taken into the theatre.If you have any further queries, please do nothesitate to contact me on: 020 7234 2730Mr Parthi Srinivasan, Consultant Liver andPancreatic Surgeon, <strong>London</strong> <strong>Bridge</strong> <strong>Hospital</strong>.9