Still Not Enough Nurses Campaign - Ontario Nurses' Association
Still Not Enough Nurses Campaign - Ontario Nurses' Association
Still Not Enough Nurses Campaign - Ontario Nurses' Association
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
ONA MEMBERS ACROSS ONTARIOONA members help drive the Safer Needles campaignWith a push from ONA members, the Safer Needles campaignpetition has been a huge success so far.The petition, with well over a thousand signatures to date, wasread twice in the <strong>Ontario</strong> Legislature, in November and December2005, once by NDP Health and Long-Term Care Critic ShelleyMartel and once by NDP MPP Andrea Horwath (Hamilton East).The petition calls for the provincial government to pass a regulationrequiring mandatory use of safety-engineered needles andother sharps in all workplaces where workers are exposed to bloodbornepathogens. We are asking each of you to sign the petitionon-line at www.saferneedles.ca.Correction notice and an updateon Local 100 efforts to improveworkload/patient careA photo caption illustrating a story on an IndependentAssessment Committee (IAC) award for the London Health SciencesCentre, ONA Local 100, was misidentified. The article and photo(shown here) ran on page 41 of the Winter 2006 ONA Vision.The caption should have said, “Members from Local 100 andan ONA staff member who fought for improved workloads andpatient care.” Our sincere apologies for the error.Since the IAC report was released in September, there havebeen three meetings involving the Local and employer todiscuss implementation of the recommendations. While theemployer has stated it fully endorses the IAC’s report, implementationhas been proceeding slowly. Local 100 members saythe employer seems to be willing to make significant changesand to involve them in the process.Local 100 members say they will continue to apply pressureto ensure the recommendations are implemented.“It is critically important to the nurses and patients thatthese recommendations are implemented,” said former Local100 Coordinator, Vicki McKenna, RN, now serving as ONA’sFirst Vice-President.“Our members still have a lot of work to do, but they arehopeful the issues can be resolved.”The petition is just one component of an ongoing province-widepublic awareness campaign for safety engineered needles and othersharps that includes billboards, radio, newspaper and subway advertising.ONA is working with SEIU and OPSEU on the campaign.“The lives of <strong>Ontario</strong> nurses and other health care workers are beingput at risk because the government hasn’t mandated the use of safetyneedles. <strong>Ontario</strong> needs to follow the lead of Manitoba and Saskatchewan,which are legislating the requirement for all health-care facilities to usesafety-engineered devices,” said ONA President Linda Haslam-Stroud,RN. Manitoba’s legislation came into effect on January 1, 2006, andSaskatchewan’s legislation becomes effective on July 1, 2006.British Columbia and Manitoba are also considering legislation tomandate the use of safer needles.“Safe needles save lives and it’s time to make them mandatory in<strong>Ontario</strong> workplaces,” said Shelley Martel, who introduced a PrivateMembers’ Bill on November 15 aimed at preventing accidental injuriesand infections from hypodermic needles and other medical sharps.Sharp medical devices such as syringes, IV catheters, blood collectionneedles, suture needles, lancets and scalpels, put health care workersand the public at risk of injury and/or infection. An estimated 33,000needlestick injuries occur each year in <strong>Ontario</strong>’s health care system.As part of the campaign, a newspaper ad ran in major dailies andcommunity newspapers in 34 markets across <strong>Ontario</strong> (see below).The radio ad also was aired in select cities. To hear the ad, visit thecampaign website at www.saferneedles.ca.If we could prevent33,000 injuries,shouldn’t we?It happens 33,000 times a year in <strong>Ontario</strong>: a health-careworker injured by a needle, exposed to possible HIV orhepatitis infection.Safety needles prevent these injuries. If we make themthe law in <strong>Ontario</strong> – like in other provinces – we cansave lives, save money and create a safer environmentfor health care workers.You can help make it happen.Visit www.saferneedles.caLet’s make safety needles the lawONTARIO NURSES’ ASSOCIATION 5
ONA MEMBERS ACROSS ONTARIORunning for College Council and committees –You can make a difference!It’s almost election time again for the College of <strong>Nurses</strong> of<strong>Ontario</strong> (CNO) Council and committees.In April 2006, RNs and RPNs from the Southwestern and CentralWestern districts, and RPNs from Central/Toronto, will elect newCouncil and committee members for a three-year term ending inJune 2009. Results of the election will be published on the CNOwebsite at www.cno.org on May 12 and in the College Standard magazinein June.ONA encourages and supports our members who run for theCNO. If you are a candidate in future CNO elections, you are invitedto submit information to be published in an ONA membership publication.Fax your information to Public Relations Team Intake at(416) 964-8891, or e-mail to PRTEAM@ona.org.What is the CNO Council and committees?Since 1963, the CNO has been a self-regulating college, with nursesregulating nurses. Council is responsible for governance at theCNO, setting the overall direction for the College and establishingregulatory policy. <strong>Nurses</strong> form the majority of the governing Council,comprised of 14 RNs, seven RPNs and 18 public members appointedby the provincial government. The CNO committees are: Discipline,Fitness to Practice, Complaints, Registration, Client Relations andQuality Assurance. Each Council member sits on one of the committees.What is the process to run?The process for running for Council or committees is the same. Anelection is held each year in different districts within the province fora three-year term. You run in the district where you work. You canrun for two terms. Check the CNO website for all election informationat www.cno.org.What are the qualifications to be a candidate?Your wealth of nursing experience, as well as a genuine interest andopen-mindedness qualify you to run for the CNO Council or committees.Your professional opinions and perspectives as front-lineunionized staff nurses are important. Contact the CNO for specificinformation on eligibility criteria to vote or run in a CNO election.What happens at Council meetings?The best way to find out what goes on is to attend a meeting. Councilmeetings are held quarterly and are open to the public. Check theCNO website at www.cno.org for meeting dates in 2006.What is the time commitment?A fair amount of time is required to participate on the Council,including reading the materials and attending the two-day quarterlymeetings. The time commitment varies for committees, dependingon how often they meet.Great! You’ve decided to run! Now what?• Contact Jenna Hofbauer, CNO Council Affairs Coordinator, atelect@cnomail.org or by phone at (416) 963-7566 (direct) ortoll-free in <strong>Ontario</strong> at 1-800-387-5526, ext. 6302. Jenna willsend you out an information package to get started. She can alsoanswer any of your questions on the process for getting elected.The deadline for nomination packages to be sent to the Collegeregistrants for the 2006 election was December 1, 2005, but it’snever too early to start thinking about the next election.• Inform your employer that you are running to ensure his/hersupport. The College will mail out your candidate information(including an election flyer) to all employers to advertise onyour behalf.• Make sure your flyer emphasizes how the public can benefitfrom your professional input and focus on your perspective ofhealth care.• Take advantage of ONA’s membership publications to advertiseyour candidacy to your union colleagues.• Develop a network, starting at your place of employment,where the nurses know you.• Attend ONA Area Coordinator Conferences (ACCs) to furtherexpand your network.• Tap into the internet. It’s a great networking vehicle and youcan set up your own webpage or site to provide information onyour candidacy.ONA candidates vie for CNO Counciland CommitteesThe following two candidates have notified ONA they arerunning for College of <strong>Nurses</strong> of <strong>Ontario</strong> (CNO) Committeesin the Central Western District election in April.• Usha R. Arora, RN, Local 25E-mail: usharm542004@yahoo.ca• Julie Flokstra-Plas, RN, Local 70E-mail: plaskj@yahoo.caYou can read about both candidates in the Members’Section of ONA’s website at www.ona.org.Any other ONA candidate who wishes to make informationavailable on ONA’s website should submit an article andphoto to Karen Rheault of the Public Relations Team, atprteam@ona.org.ONTARIO NURSES’ ASSOCIATION 7
ONA MEMBERS ACROSS ONTARIOTime to stop the violenceDear ONA,It’s no secret the death of Lori Duponthas devastated the nursing profession,especially the nurses here in Windsor.Violence in the workplace (hospitals)is a common occurrence. It is abouttime the administrators and governmentofficials who have taken on the responsibilityfor making difficult decisions toMAKE THEM!!!!As a nurse, I feel we need to honourand show our deepest sympathy to ourcolleague. I feel perhaps something similarto a “black ribbon” campaign or anational day of mourning is in order. Dowe not remember and honour the femaleengineers murdered in Montreal?It’s time to stop the violence beforeanother tragedy takes place.Paula Vincelli, RN, BScNONA Local 11,Windsor Regional HospitalWindsor, <strong>Ontario</strong>Vigil against violenceLetters highlight ONA’s strong call for protectionsfrom violence for all <strong>Ontario</strong> womenONA President Linda Haslam-Stroud, RN, had letters published in three newspapers in<strong>Ontario</strong> in recent months on the issue of violence against nurses, following the tragicmurder of ONA member Lori Dupont, RN. The following are excerpts from her letters:From the Eganville Leader (November 2005)Re: “System failure”“ONA agrees with you that the legal system failed to protect Lori Dupont. Her death has devastatedher family, friends, colleagues and ONA’s 51,000 members. They have rallied togethersince Lori’s death to press for tougher laws to protect women – all women – from violence …Our members – 94 per cent of whom are women – are even more sensitive to violence againstwomen, as nurses face incidents of violence in the workplace from patients and their families,and even their own colleagues, on such a widespread basis. They are writing to their MPPsand lobbying for amendments to legislation that will make women safer everywhere. Noneof us wants to see another woman lose her life because of the justice system.”From the Peterborough Examiner (December 2005)Re: “Man charged with assaulting nurse”“<strong>Nurses</strong> in this province are three times more likely than any other professionals to bethe victims of violence in the workplace – whether physical, verbal or sexual abuse. Asurvey of ONA members revealed that 36 per cent have experienced physical violencein the workplace (most being attacked by their patients); 67 per cent of those surveyedreported being the target of verbal abuse (most from patients and doctors); and 11 percent report they’ve been the target of sexual abuse in the workplace – most often bypatients and doctors. To say that sexual assault is a rare occurrence is misleading at best,and hurtful to the registered nurses who face threats to their safety on a daily basis asthey provide care for their patients.”From the Windsor Star (December 2005)Re: “Dupont probe launched: Hospital initiates review intonurse’s slaying”ONA is very pleased that Hotel-Dieu Grace Hospital’s board has made the (belated) decisionto review its role and responsibility in the events that led to the horrific murder of LoriDupont, RN … ONA is appalled at the lack of response from the Ministry of Labour, thehospital and the Coroner’s office to our repeated calls for investigations into Lori’s workplacemurder by anesthetist Marc Daniel. While the hospital review is a start, the announcementin no way absolves the Ministry of Labour of its responsibility to conduct a fatalityinvestigation into this case ... ONA will continue to follow developments in Windsor andwill continue to press for a fatality investigation into our member’s tragic murder.ONA members joined other unions in a vigil on the National Day of Action on ViolenceAgainst Women on December 6, 2005, commemorating the murder of 14 women in Montreal and women who are victims of domesticviolence. ONA Region 5 Vice-President Jeanne Soden, RN, (left) holds up a sign bearing the name of Lori Dupont, RN, an ONA member fromHotel Dieu-Grace Hospital in Windsor, Local 8, who was killed by a former partner and colleague while working. Holding a sign in memoryof worker Jessica Nethery is Irene Harris, Secretary-Treasurer of the <strong>Ontario</strong> Federation of Labour.8 VISION, SPRING 2006
ONA MEMBERS ACROSS ONTARIOActions have consequencesTo the Hon. Dalton McGuinty,Premier of <strong>Ontario</strong>I have been a registered nurse for 26 years and have seen manychanges in health care during my career, all of course dependant onthe government of the day. I have always been a strong believer invoting on Election Day ... if you don’t vote, you have no say, etc.I did put my X beside Mike Harris’s name and lived to regretthat choice as he slashed and burned his way through healthcare “reform” during his term in office. So, I voted for your partythis last election thinking to myself, “Well, they can’t be anyworse than the Conservatives!!!” Little did I know my wordswould turn out to be prophetic.The recent announcement that our new hospital to be builthere in North Bay will be privately funded is absolutely horrific!What are you thinking? I realize the budget is the bottom line,but you’re putting the weight of a balanced budget squarely onthe backs of every single taxpayer in <strong>Ontario</strong>, while at the sametime pushing adequate health care further and further away fromtheir reach. Private-Public Partnership (P3) hospitals fundamentallygo against everything our health care system in this provinceand country stands for. Did you not campaign vehementlyagainst privatization of hospitals?We here in North Bay are in a deplorable situation – the site isselected for the new hospital, the land is prepared, it’s even goneto tender ... meanwhile, we are working out of two aging buildingsthat costs us more than $2 million (over budget) per yearto operate, and then we are punished because we can’t balanceour budget. We, the employees at North Bay General Hospital,have been told by our senior administration that if they don’tsubmit a balanced budget, the funding will not be there for ournew hospital!So, they slash and burn (sound familiar???), staff is being cut,hours are reduced for part-time workers, and now it is announcedthat funding will be private. I don’t mean this to sound hostile, butas a front-line nurse I can tell you things are not good!As a parent, I try and teach my children that actions have consequences... well Mr. McGuinty, I’d like to give you that messagetoo! Health care is currently at a dangerous level – staffing hasbeen cut, and 30-50 per cent of nurses in the province are eligibleto retire in the next 3-5 years. Your government keeps statingyou’re going to hire thousands of nurses to all these positions.There are NO NURSES out there waiting for you to hire them!I urge you to seriously reconsider your position regarding privatefunding for these seven new hospitals. Remember, actionshave consequences. Whoever will I vote for next election?Demand for balanced budget costseveryoneReprinted from the St. Catharines Standard (June 2005)Re: The editorial, “Hospital workers union should takethe long view.”I would like to clarify the perspective of the <strong>Ontario</strong> <strong>Nurses</strong>’<strong>Association</strong> regarding the Niagara Health System’s (NHS) planto deal with the provincial government’s demand for a balancedhospital budget by 2006-07.For years, successive provincial governments have ignoredthis community’s unique needs for additional hospital funding.The expectation that our hospitals can live within these insufficientbudgets, and balance, is madness. This has meant a constantfinancial struggle that impacts on everything – includingnursing resources.St. Catharines is about to lose some bed capacity, almostimmediately, to help comply with the government’s requirementsto balance the bottom line. Bed closures are a blow toany community. <strong>Nurses</strong> believe closures must never come at theexpense of safe quality health care. Managing “utilization” inthe hospital setting means preventing delays in care and treatment,getting patients treated quickly and completely, and homesafely to stay. Streamlined processes, improved inpatient careand outpatient supports can save hospital “bed days,” but if it isnot done right, it will not be safe or sustainable.ONA Local 26 represents the registered nurses in the hospitalsector in Niagara. No nurse wants to see bed cuts, but for us,there is no choice but to take a “long view” in all of this. Andthat view is extremely perplexing. Our region’s hospital nursingworkforce is now stretched beyond our capacity. There are currentlydozens of nursing positions at NHS which are unfilled– vacant – with no applicants. This is reflective of a provincewidenursing shortage.Across <strong>Ontario</strong> and in Niagara, nurses are experiencing difficultand stressful working conditions due to excessive workloads.Working overtime is necessary just to provide ongoingnursing coverage. With shortened hospital stays and so manyelderly in Niagara, our patient population is more acute andmore complex, requiring a greater degree of nursing care.Research has shown that hospitals with a full complement ofthe correct classifications of registered nursing personnel operatemore efficiently, and have better patient outcomes.We are depending on the NHS to address the nursing shortagein Niagara by making sure we are running efficiently, staffedappropriately and have working conditions that will attractnurses to Niagara. This also means having contracts in place thatvalue and respect nurses for the work they do.Leslie Manary,RNONA Local 20,North Bay General Hospital, North Bay, <strong>Ontario</strong>Heather Cross, RNBargaining Unit President, ONA Local 26,Niagara Health Systems, St. Catharines, <strong>Ontario</strong>ONTARIO NURSES’ ASSOCIATION 9
CEO’s messageONA MEMBERS ACROSS ONTARIOLesley Bell, RNONA Chief Executive OfficerHealth and safety legislation requires immediatechanges to protect workers from violenceONA is seekingan amendment toSection 43 of the<strong>Ontario</strong> Healthand Safety Act(OHSA) and itspolicies, whichwould make thethreat of violencea right-to-refuseworkplace hazard.<strong>Ontario</strong> law must be changed to protect ONAmembers, and in fact all women in this province, frombecoming victims of violence. The failure of the <strong>Ontario</strong>legal system and existing legislation to prevent the kindof senseless tragedy that befell two of our members in2005, Lori Dupont, RN, and Lorraine Egan, RN, is disgraceful!Lori Dupont was murdered while carrying out herduties in the recovery room of Hotel-Dieu GraceHospital in Windsor. Her former partner, an anesthetistat the same hospital, stabbed her to death in front of herhorrified colleagues. She had been seeking protectionfrom her attacker for months, but faced delays becauseof backlogs in the courts and appeals from herattacker.The hospital had an outstanding order from theMinistry of Labour (MOL) re workplace violence thatwas to be met by October 28. Lori Dupont died onNovember 12, when the hospital had yet to meet therequirements of the MOL order.In the spring of 2005, Lorraine Egan, a nurse atBluewater Health in Sarnia, was murdered by her stepbrother.He had been stalking her for some time and shehad obtained a restraining order against him, but it didnot protect her from being brutally murdered.These two tragedies underscore the need for immediateand aggressive changes to legislation in this province.Almost 10 years ago, an inquest into the murder ofanother woman – Theresa Vince, killed by her boss in aChatham Sears store in June, 1996 – resulted in the juryrecommending sexual harassment be included in theprovincial Occupational Health and Safety Act (OHSA).This recommendation has still not been implemented,and yet it would have given Lori Dupont’s employer thepower to dismiss the man who took her life, and wouldhave provided more options for Lori to safeguard herpersonal safety. For instance, Lori could have absentedherself from the workplace without financial penaltyduring the legal process.ONA is leading the call for legislative change in<strong>Ontario</strong> to ensure tragedies like these do not happenagain to any ONA member, or any woman in this province.It is unacceptable that the provincial governmenthas failed to expedite this legislative change, whilewomen remain vulnerable to violence by men whostalk, threaten or harass them.Specifically, ONA is seeking an amendment to Section43 of the OHSA and its policies, which would make thethreat of violence a right-to-refuse workplace hazard.<strong>Nurses</strong> are vulnerable in the workplace. They arethree times more likely to suffer violence than any otherprofessional group. Our own membership surveyrevealed stunning statistics:• 36 per cent of our members have experiencedphysical violence in the workplace, the majoritybeing physically attacked by patients.• 67 per cent reported they had been the target ofverbal abuse in the workplace. Patients and doctorsare the most-reported source of the verbalabuse.• 11 per cent reported they had been the target ofsexual abuse in the workplace. Patients and doctorsare the most reported source of the sexualabuse.In our view, by choosing to wait until a police andcoroner’s inquest was complete, the Ministry of Labouris spending too much time deciding to investigate LoriDupont’s murder to determine whether measures shouldhave been taken to protect her in the workplace. Timelyaction must be taken, and efforts need to be coordinatedwith the police to ensure a complete investigation isundertaken in any event like this.The tragic murders of Lorraine Egan and Lori Dupont,and the daily abuse and hazards nurses face as they carefor their patients, underscore the need for tougherlaws.ONTARIO NURSES’ ASSOCIATION 11
Un mot de la PrésidenteLinda Haslam-Stroud, inf. aut.Présidente de l’AIIORapport spécial de la présidente sur l’état des négociations :La nouvelle ronde de négociations sera d’une importance cruciale, au momentoù le secteur des soins de santé en <strong>Ontario</strong> connaît des changements majeursNous devons tirerparti de nosgains… nousdevons nousappuyer sur labase que nousavons établiepour les atteindreau cours de laprochaine ronde.L’encre a à peine eu le temps de sécher sur nosnouveaux contrats que nous nous préparons pour unenouvelle ronde de négociations. Bien que, en fin d’année2005, nous ayons reçu les décisions arbitrales finales etque nous les ayons fait connaître à nos membres tant dusecteur hospitalier que des maisons de soins infirmiers,l’AIIO cherche toujours à résoudre certaines questionsqui demeurent en suspens depuis les dernières rondes.<strong>Not</strong>amment, les questions reportées à la suite de la décisiond’arbitrage Keller pour les hôpitaux (voir l’articletraitant de l’augmentation de 2 % pour les infirmières enmilieu hospitalier ayant 25 ans d’expérience à la page **). Veuillez communiquer avec votre présidente d’unité denégociation si vous avez des questions au sujet de la miseen application de cette augmentation.Nous avons réalisé un de nos objectifs clés pour nosmembres des secteurs des foyers pour personnes âgées etdes organisations caritatives, soit la parité salariale pourtoutes. Nous cherchons à poursuivre notre percée enmatière de parité salariale pour les membres du secteurdes maisons de soins infirmiers; un objectif qui tarde àêtre atteint pour cet important secteur.Quoique que nous ayons fait progresser certains secteursen 2005, il reste beaucoup de travail à faire. Nous devonstirer parti de nos gains. En ce qui concerne les objectifsque nous n’avons pas atteints, nous devons nous appuyersur la base que nous avons établie pour les atteindre aucours de la prochaine ronde. Les questions prioritairestelles que les prestations de retraite et la parité dans lesmaisons de soins infirmiers ne peuvent tout simplementplus être mises de côté; fait que le gouvernement et lesemployeurs doivent reconnaître et accepter.Le travail syndical est incessant puisque nous pouvonstoujours aller plus loin dans notre quête de contrats quivalorisent le travail des 51 000 infirmières et infirmiersdu système des soins de santé de l’<strong>Ontario</strong>. Il s’agira denotre objectif de négociation cette année.Comme le titre du présent document le suggère, cetteronde de négociations sera cruciale pour nos membres.La pénurie de personnel infirmier s’accentue de plus enplus, le système d’assurance-maladie continue d’êtreremis en question, la charge de travail au sein de la professionmet en danger les infirmières et les patients, toutcomme la santé et la sécurité au travail. Le projet de loiRLISS proposé rend l’avenir très incertain pour les travailleusesdes soins de santé de la province, alors quenous faisons face à une nouvelle restructuration massivedu système de santé ontarien.Un nouveau cycle s’amorce donc; nous avons retroussénos manches et sommes prêtes à partir en quête de meilleuresconditions de travail pour tous nos membres.La nouvelle équipe centrale de négociation des hôpitauxest maintenant en place, et nous prévoyons que l’équipecentrale de négociation des maisons de soins infirmiers seraégalement prête lorsque vous lirez ces lignes. Nous examinonsle protocole d’entente sur les conditions des négociationsconjointes pour chacun de ces secteurs. Il s’agit de lastructure du processus de négociation, qui comprend lescalendriers de négociation et d’arbitrage, et le cas échéant,des processus de négociation central et local.La session d’orientation de l’équipe centrale de négociationdes hôpitaux s’est terminée à la fin janvier.L’équipe débutera les négociations pendant la semaine du26 février et devrait avoir fini durant la semaine du 3avril. Si aucune entente n’est conclue, le service de conciliationoffert par le ministère du Travail de l’<strong>Ontario</strong>sera utilisé pendant la deuxième semaine de négociations.En cas d’impasse des négociations, on fera appel àla médiation-arbitrage pour la résorber tel que la loi lerequiert. Dans le cadre de la dernière ronde, la médiationet l’arbitrage ont été assurés par le conseil Keller. Cettefois-ci, nous avons convenu de séparer les processus etd’utiliser un médiateur et un conseil d’arbitrage distincts.Nous espérons ainsi obtenir des résultats positifs.Nous nous servirons d’un style plus traditionnel denégociation pour la ronde du secteur hospitalier et nousn’utiliserons pas le processus de négociation axé sur lesintérêts favorisé au cours des trois dernières rondes.Nous espérons que, de cette façon, le processus progresserabeaucoup plus rapidement et que nous seronsconfrontées à moins d’obstacles que lors de la dernièresuite en page 1412 VISION, SPRING 2006
Message de la directrice generaleLesley Bell, inf. aut.,Directrice généraleUne réforme immédiate aux Lois sur la santé et la sécurité autravail est requise pour protéger les travailleuses contre la violenceL’AIIO cherche àfaire amenderl’article 43 de laLoi sur la santé etsécurité au travail(LSST) et sespolitiques,amendement quidonnerait undroit de refus detravailler face à lamenace deviolence.La loi ontarienne doit être réformée pour protégerles membres de l’AIIO, et en fait toutes les femmes de laprovince, pour éviter qu’elles ne soient victimes de violence.Il est scandaleux que ni le système juridiqueontarien ni les lois existantes n’aient pu empêcher quedes crimes gratuits soient perpétrés en 2005 contredeux de nos membres, soit Lori Dupont, IA, et LorraineEgan, IA.Lori Dupont a été assassinée au cours de l’exercice deses fonctions dans la salle de réveil de l’hôpital Hôtel-Dieu Grace, à Windsor. Son ancien conjoint, un anesthésistetravaillant au même hôpital, l’a poignardée àmort sous les yeux horrifiés de ses collègues. Elle cherchaità se protéger de son agresseur depuis plusieursmois. Des retards au chapitre des procédures judiciaireset les recours en appel de son agresseur ont compliquéla situation.L’hôpital faisait l’objet d’une ordonnance en cours duministère du Travail relativement à la violence en milieude travail; ordonnance à laquelle il devait se soumettreau plus tard le 28 octobre. Lori Dupont est morte le 12novembre, alors que l’hôpital n’avait toujours pas satisfaitaux exigences de l’ordonnance du ministère duTravail.Au printemps 2005, Lorraine Egan, une infirmière àl’hôpital Bluewater Health, à Sarnia, a été assassinée parson demi-frère. Il la traquait depuis un certain temps etelle avait obtenu contre lui une ordonnance d’interdictionde communiquer, cela ne l’a cependant pas suffisammentprotégée de son assassin.Ces deux tragédies démontrent que la réforme immédiateet exhaustive de la législation provinciale estessentielle.Il y a presque dix ans, à la suite de l’enquête sur lemeurtre de Theresa Vince, tuée par son patron dans lemagasin Sears de Chatham en juin 1996, le jury arecommandé que le harcèlement sexuel soit inclus à laLoi sur la santé et sécurité au travail (LSST) provinciale.Cette recommandation n’est toujours pas en vigueur,pourtant celle-ci aurait permis à l’employeur de LoriDupont de congédier l’homme qui a assassiné cettedernière, et à Madame Dupont d’avoir différents recourspour se protéger. Par exemple, Madame Dupont auraitpu s’absenter de son travail sans sanction pécuniairependant les procédures judiciaires.L’AIIO mène la demande de la réforme de la loi en<strong>Ontario</strong> pour empêcher que d’autres tragédies semblablesne se reproduisent au sein de l’AIIO ou de laprovince. Il est inacceptable que le gouvernement provincialn’ait pas réussi à faire adopter cette réforme,alors que les femmes demeurent vulnérables à la violencequi leur est faite par des hommes qui les traquent,les menacent ou les harcèlent.Plus particulièrement, l’AIIO cherche à faire amenderl’article 43 de la LSST et ses politiques, amendement quidonnerait un droit de refus de travailler face à la menacede violence.Les infirmières sont en position de vulnérabilité autravail. Elles sont trois fois plus à risque d’être victimesde violence que les membres de tout autre groupe professionnel.Un sondage auprès de nos membres s’estavéré fort révélateur. Voici quelques statistiques :• 36 pour cent de nos membres ont été victimes deviolence au travail; de ce pourcentage, la plupartd’entre elles ont été agressées physiquement pardes patients.• 67 pour cent ont déclaré avoir été victimes d’abusverbal au travail. L’abus verbal provient principalementdes patients et des médecins.• 11 pour cent ont indiqué avoir été victimes d’abussexuel au travail. L’abus sexuel provient principalementdes patients et des médecins.Selon nous, en choisissant d’attendre que l’enquêtedu coroner et de la police soit close, le ministère duTravail a mis trop de temps à décider d’enquêter sur lemeurtre de Lori Dupont pour déterminer si des mesuresauraient dû être prises afin de la protéger dans sonmilieu de travail. Lorsqu’un tel événement se produit, ilfaut intervenir rapidement et joindre nos efforts à ceuxde la police pour s’assurer qu’une enquête soit ouverte.Les meurtres tragiques de Lorraine Egan et de LoriDupont, ainsi que l’abus et les dangers quotidiens auxquelsfont face les infirmières en prenant soin de leurspatients, témoignent de la nécessité de renforcer la loi.ONTARIO NURSES’ ASSOCIATION 13
President’s messageUn mot de la Présidentesions, vacations, leave issues, job securityand workload/staffing continue to be the toppriority issues.Some of the prevailing issues to be addressedinclude the nursing shortage, the impact ofLocal Health Integration Networks (LHINs)and abolishment of mandatory retirement.In terms of LHINs, we will be looking athow we can include language to protect ourmembers when legislative changes gothrough revamping workplaces and administrativestructures. We expect a major transformationon how health care is delivered in<strong>Ontario</strong> in all sectors.Of particular note will be the impact onmembers if the provincial government doesindeed move to adopt the competitive biddingprocess for the provision of health sercont.from page 10Special report on bargaining from the President:vices, in view of how much this has negativelyimpacted on our members in the communitysector.In terms of the removal of the mandatoryretirement age of 65, scheduled to kick in onJanuary 1, 2007, ONA maintains the positionthat members have the right to extend theircareers if they so wish. Currently employershave the right to require members to retire atage 65. That all ends on January 1, 2007.While members will now be able to workbeyond age 65, we will need to ensure thatthose who do continue to enjoy all of thebenefits of the collective agreement – and donot suffer a loss of benefits or other hardearned rights.With a current average retirement age of57 years, we don’t see the end of mandatoryretirement as the answer to the nursingshortage. In fact, given the demanding natureof nursing employment, ONA is even moredetermined to negotiate pensions and benefitsthat would allow our members to retirewith dignity and financial security at theearliest age possible.Advancing the social, economic and generalwelfare of our members is ONA’s reasonfor being. Your elected teams will certainlybe a strong voice representing our frontlineinterests. Our vision is: <strong>Ontario</strong> <strong>Nurses</strong>’<strong>Association</strong>: Our Union. Respected, Strong,United. Committed to members who care forpeople. As I commence my second term asyour President, I will continue to bring yourvoice to all discussions as we seek to improveour working lives and provide quality care toour patients.suite de la page 12Rapport spécial de la présidente sur l’état des négociations :ronde, ce qui se traduira par la négociationponctuelle de la convention collective.S’ils s’avèrent nécessaires, nous nous attendonsà ce que la médiation ait lieu en mai etl’arbitrage en juin. Scénario qui dépendra de ladisponibilité des arbitres; puisque les meilleursarbitres dans ce domaine sont habituellementceux dont le calendrier est le plus chargé.Votre équipe de négociation des hôpitauxétudient les questions prioritaires de négociationpour la nouvelle ronde d’après lesréponses au questionnaire « Exprimezvous» envoyé à tous les membres en règlecet automne. Les propositions et les objectifspour chacune des rondes sont en grandepartie fondés sur les réponses recueilliesdans ces questionnaires. Le salaire, les avantages,les dispositions relatives à la retraite,les vacances, les congés de maladie, la sécuritéd’emploi et la charge de travail ainsi quel’affectation du personnel demeurent lesquestions prioritaires.Parmi les questions urgentes à régler, onnote la pénurie de personnel infirmier,l’impact des réseaux locaux intégrés de servicesde santé (RLISS) et l’abolition de laretraite obligatoire.En ce qui a trait aux RLISS, nous essayonsde déterminer comment nous pouvons intégrerdes clauses pour protéger nos membreslorsque des modifications législatives sontapportées pour réorganiser les structuresadministratives et en milieu de travail. Nousnous attendons à ce qu’il y ait un changementmajeur dans la façon de dispenser lessoins de santé en <strong>Ontario</strong>, dans tous lessecteurs concernés.Il serait intéressant de voir quel seraitl’impact sur les membres si le gouvernementprovincial allait de l’avant et adoptait le systèmede demande de soumissions concurrentiellespour la prestation de soins desanté, quand on pense à l’impact négatifqu’un tel système a eu pour nos membres dusecteur communautaire.Quant à l’abolition de la retraite obligatoireà 65 ans, en vigueur à compter du 1erjanvier 2007, l’AIIO est toujours convaincueque les membres ont le droit de prolongerleur carrière s’ils le veulent. Les employeurspeuvent actuellement exiger que les membresprennent leur retraite à l’âge de 65 ans.Ce ne sera plus le cas à partir du 1er janvier2007. Maintenant que les membres pourronttravailler bien qu’ils aient atteint l’âge de 65ans, nous devrons nous assurer que ceux quichoisissent de le faire continueront de bénéficierde tous les avantages que leur confèrela convention collective et qu’ils ne perdrontaucun des avantages et des droits difficilementacquis.Comme l’âge moyen de la retraite est de 57ans, nous ne nous attendons pas à ce quel’abolition de la retraite obligatoire remédie àla pénurie de personnel infirmier. En fait,comme la profession d’infirmière est exigeante,l’AIIO est plus résolue que jamais ànégocier des pensions et des avantages quipermettront à nos membres de se retirerdignement et de profiter d’une certaine sécuritéfinancière le plus tôt possible.L’avancement social et économique, ainsique le bien-être général de nos membres,sont la raison d’être de l’AIIO. Les équipesélues constitueront certainement des forcesmajeures pour représenter nos intérêts depremière ligne. <strong>Not</strong>re vision est : l’<strong>Association</strong>des infirmières et infirmiers de l’<strong>Ontario</strong> : unsyndicat respecté, fort et uni. Dévouée à sesmembres qui prennent soin des gens. Dans lecadre de mon second mandat à titre de présidente,je continuerai, à l’occasion de toutesles conférences-discussions, de faire part devos opinions alors que nous tentonsd’améliorer notre vie professionnelle et laqualité des soins à nos patients.14 VISION, SPRING 2006
Patients Matter<strong>Still</strong> <strong>Not</strong> <strong>Enough</strong><strong>Nurses</strong> <strong>Campaign</strong> –What it’s all about!ONA embarked on a province-wide public affairs and lobbying campaign in 2004 to alert thepublic and health care decision-makers to the devastating impact of the ongoing nursingshortage on the provision of health services in <strong>Ontario</strong>. The “<strong>Still</strong> <strong>Not</strong> <strong>Enough</strong> <strong>Nurses</strong>! Actnow! Patients can’t wait” campaign has received intensive media attention province-wideand has gained support from many groups and individuals, who believe the key to resolvingthe challenges of <strong>Ontario</strong>’s health care services is to ensure there are enough nurses workingin the system and that the nursing workforce is stabilized. ONA’s campaign intensifies in2006, with major television advertising and the continued roll out of regional events. Thefollowing feature section explains why ONA felt it necessary to undertake this comprehensivecampaign – the most ambitious and far-reaching campaign by ONA in its 32-year history.Much of the material in this article and the accompanying sidebars are contained inliterature that was produced for the campaign. You can read much more about it on thecampaign website at www.stillnotenoughnurses.ca.ONTARIO NURSES’ ASSOCIATION 15
Patients MatterThe roots of a health care problem and how to alleviate itMost Ontarians are aware therearen’t enough nurses working inthis province. Yet these same citizenscould well be puzzled over the causes ofthe problem. For years they have been bombardedwith the message that health carespending by government is enormous, growingand probably unsustainable. If so muchmoney is being directed at health care, theywonder, what explains the insufficient numberof nursing professionals in the system?Health spending in <strong>Ontario</strong> is inadequatewhile the public’s needs remain unmetThe truth is that public spending on healthin <strong>Ontario</strong> has been insufficient for sometime – and inadequately accounted for. Whileit is the case that health care currentlyaccounts for 40 per cent of the provincialbudget, the whole story is more complicated.As a percentage of provincial Gross DomesticProduce (GDP), expenditure by 2004 was infact below the six per cent mark recorded adecade earlier. In Canada as a whole, spendinghas followed a similar pattern.Health spending by government per residentin <strong>Ontario</strong> dropped from approximately$1,900 in 1992 to $1,750 in 1997 and thenstagnated until almost the end of the decade.Provincial spending on hospitals, after risingsteadily since the mid-1970s, actuallydeclined in absolute terms during a sevenyearstretch. The latter part of the 1990s sawregistered nurses (RNs) fired, as budgetarytargets rather than patient needs determinedstaffing decisions. Those who remained sawtheir workloads increase substantially. Overall,according to data from the College of <strong>Nurses</strong>of <strong>Ontario</strong> (CNO), the decade of the 1990ssaw a drop in the ratio of working RNs toOntarians from almost eight per 1,000 to lessthan seven. By the early years of the new millennium,<strong>Ontario</strong> placed ahead of only BritishColumbia in this category.At the same time, the government decidedthat more health services should be deliveredat home and in long-term care establishments,such as nursing homes, where workersgenerally earn lower salaries than inhospitals. The result was predictable: as theproportion of RNs working in a hospital settingfell sharply between 1992 and 2002,many also left the profession. Meanwhile,young women and men of university agesteered clear of a career that in the MikeHarris years promised little in the way of jobsecurity or satisfaction. Enrolment in <strong>Ontario</strong>nursing schools dropped dramatically.The implications of understaffed hospitals:overworked professionals, higher mortalityThe provincial Liberal Party took office in2004 promising to add some 8,000 full-timenurses over the course of its first mandate. Asurvey released by the Registered <strong>Nurses</strong>’<strong>Association</strong> of <strong>Ontario</strong> (RNAO) in June 2005suggested that approximately 1,500 RNsmay have been hired province-wide by thatpoint – even as the government recognizedthat 757 others could be laid off by hospitalsstriving to balance their books. In January,the chair of the <strong>Ontario</strong> Hospital <strong>Association</strong>(OHA) had announced that without “a significantlyrevised multi-year funding plan,”hospitals “would have no choice” but toeliminate up to 8,700 jobs in 2006 – some3,500 of these positions corresponding tonurses. As late as September 2005, abouthalf-way through its mandate, the government’sown data indicated that barely 2,000new, permanent nursing jobs existed.According to ONA President Linda Haslam-Stroud, RN, who doubts Queen’s Park isgoing to achieve its hiring target, hospitalsare also trying to save money by lowering theskill level of their workforce. Increasingly,“they are going to erode registered nurses andreplace them with less-skilled, cheaper workers.As you reduce the expertise of front-linehealth care providers, you produce an accompanyingdecline in care. Patients don’t receivethe more complex care that an RN provides.”Numerous studies have in fact concluded16 VISION, SPRING 2006
that there is a direct correlation betweenrecovery rates and staffing. An insufficientnumber of qualified nurses in hospitals, forexample, results in more frequent medicationerrors as well as a greater incidence ofpneumonia, ulcers, post-operative infectionsand urinary tract infections. One investigationeven concluded that in-hospital mortalityclimbs by seven per cent for each patientadded to an average nursing workload!Unfortunately, there is even more ominousnews. As the Nursing Effectiveness,Utilization, and Outcomes Research Unit(NRU) at the University of Toronto recordedin a study released in the fall of 2003, the agestructure of <strong>Ontario</strong>’s nursing workforce isextremely worrisome. Some 66 per cent ofemployed nurses are over 40 years of age, upfrom 58 per cent a decade previous. Especiallytroublesome is the fact that 17 per cent of<strong>Ontario</strong> RNs are older than 55 and thuslikely to retire soon. In the high-stress worldof nursing, 56 is a far more typical retirementage than 65. If predictions are correct, morethan 20,000 registered nurses will leave thesystem imminently, considerably more thancan be replaced, under any realistic scenario,in the short term.The looming gap is an unpleasant one tocontemplate.What can be done to address this issue?Advocates of publicly-funded health care proposea series of measures that could, over thecourse of a decade, go some way to alleviatingthe worst effects of a growing shortage.To begin with, losses of nurses alreadyemployed in the system could be curbed(though not, of course, eliminated) byencouraging a larger percentage of the workforceto continue working until age 65. Asidefrom bolstering total numbers, this approachhas the merit of retaining more experiencedprofessionals in the <strong>Ontario</strong> health care system.These workers, provided they have thepaid time to do so, could also play an invaluablerole in mentoring younger nurses.As Haslam-Stroud acknowledges, fundinghas been directed to objectives of this type,with some late-career nurses benefiting fromreduced workloads and assignment to “specialprojects.” But ONA’s president arguesthat so far, such initiatives have been “stopgapand temporary in nature.” Considerablymore financial commitment on government’spart is required. Sue Matthews, ProvincialChief Nursing Officer, responds that additionalfunds for this initiative will be madeavailable as its benefits become apparent.Improving working conditions and safety sothat nurses stay on the jobAs it stands, nurses tend to leave their jobswell before mandatory retirement age preciselybecause their work is dangerous,increasingly difficult, physically demandingand insufficiently rewarding.When it comes to violence in the workplace,for example, health care employees arein the least enviable position of any professionalset. And when this fairly broad categoryof workers is broken down, there is littledoubt that nurses – those who have the mostONA’S 12 Proposals1. Add RNs and other healthprofessionals so that hospitals, longtermcare facilities and home careproviders serve patients better. Don’treplace RNs with less-skilled workers.2. Increase base funding to health careinstitutions to enable more RNs toprovide patient care.3. Invest as necessary to make thehealth system work. Patients areworth the expense.4. Keep late-career nurses in the systemby improving working conditions,raising safety standards andreducing workload. By encouragingthese professionals to stay in theworkforce, younger colleagues willalso have access to much-neededmentoring.5. Aim for no fewer than 12,000 new,permanently-funded nursing positionsby 2008.6. Improve scheduling for fulltimenurses so they can betterbalance professional and privatecommitments. To the extent this isaccomplished, more part-time RNssay they will favour full-time work.7. Offer full-time jobs to all working andgraduating nurses who desire them.Turn overtime into new jobs.8. Improve care and staffing by givingnurses more of a say in health carefacilities.9. Invest the funds necessary to improveinfrastructure at nursing schools andreplenish the ranks of instructors,so that future supplies of nursingprofessionals are abundant.10. In the case of home care, put an endto the system of competitive biddingand for-profit services. Neitherpatients nor workers have been wellserved.11. Fund public health units adequately,so they can fulfill their mandate.12. Preserve Medicare as a “one-tier”system for all. That’s what Ontarians– and Canadians – want.ONTARIO NURSES’ ASSOCIATION 17
direct contact with patients – are among thosemost at risk. Obviously, violent workplacesproduce physical injury as well as emotionalsuffering. To make the nursing profession amore attractive and rewarding one, to encourageseasoned professionals to remain in thefield longer while attracting new nurses, it isnecessary to eliminate violence in hospitals,home care and long-term care facilities wherefeasible, and to reduce it to an absolute minimumin other cases.<strong>Nurses</strong> need contracts and legislation thatspell out employers’ obligations around safetyissues. They require adequate support inthe event they are assaulted, including leave,legal assistance and counselling. Such measureswill help make nurses feel they arerespected, valued and protected.On-the-job injury unrelated to violence alsoplagues nurses to an alarming degree. In fact,nurses make two times as many injury claimsas others employed in health care institutions.According to one study, 40 per cent of nursesreport suffering from pain due to workplaceincidents at least some of the time, while ashocking one-quarter say they experience muscleor bone discomfort most or all of the time.Needles present another significant healthrisk to nurses, with accidental puncturesconstituting a substantial number of on-thejobinjuries. ONA applauds the fundingprovided to purchase safety-engineered needlesbut believes the province must mandatethe use of these improved devices.One way that hospitals have responded toreduced resources is by requiring employees18 VISION, SPRING 2006to work additional hours. Indeed, between1997 and 2002, the estimated number ofnurses working extra time doubled. Totalsvary from year to year, but studies suggestthat the equivalent of between 7,000 and8,600 full-time jobs Canada-wide is beingperformed by nurses working overtime!While hospital administrators may congratulatethemselves on their efficient use oflabour, the productivity gains are illusory. Asit turns out, there is almost a perfect correlationbetween overtime and sick time; additionalhours worked are later taken off. Overthe course of a year, some 16 million nursinghours are lost to injury and illness in Canada,a total that is itself the equivalent of about9,000 full-time jobs. Clearly, nurses cannotstand up under the strain.Acquiring a meaningful say for nurses inhospitals and staffingFinally, there are issues of politics and influenceto address. According to Linda O’Brien-Pallas, professor of nursing at the Universityof Toronto and Chair of the NRU, she andher colleagues “are trying really hard to educateCEOs and hospital boards about theimportance of increasing staff and not tryingto constantly squeeze more out of the currentworkforce.” Yet, she acknowledges thatthe mere fact decision-makers have to belobbied for such a strategy, speaks to the difficultyRNs have in getting their voicesheard. <strong>Nurses</strong>, as professional workers indispensableto the proper functioning of hospitals,require greater input.Raising the level of patient care in long-termcare institutions and in the communityHomes for the aged, nursing homes andpatients’ homes are the workplaces wherenumerous nurses carry out their tasks.<strong>Ontario</strong> governments have for years favoureda shift of health care delivery away from hospitalsand into the community. But thesegovernments have not made this policy effectiveand fair for all concerned.As already noted, nurses working in theseareas of health care earn less than their colleaguesemployed in a hospital setting. Theirbenefits package is also lower. A higher proportionof nurses in non-hospital workplacesare also employed on a part-time or casualbasis.The latter 1990s saw Community CareAccess Centres (CCACs) boost their patronageof for-profit agencies by some 265 percent as a market-driven system became therule in home care provision. The result wasnot a positive one for health professionals, asunionized employers like the Victorian Orderof <strong>Nurses</strong> (VON) were pushed out by firmspaying lower salaries. And while the currentprovincial government has pumped morethan $100 million into home care with theobjective of boosting staff levels, evidencesuggests the proportion of full-time employmentis not improving.Nor have patients been well-served. Forprofitfirms offer less continuity of care; underthe current scheme, as contracts are won andlost by different agencies, patients see differentnurses. Dollars that could be directed to
Patients Matterimproving care end up as private profits.“Case managers tell me they only have somuch money to spend. The result is that thesickest patients are given priority while the‘less sick’ are left with basically no care,” saysHaslam-Stroud.Meanwhile, nurses in long-term care institutionsare also under increasing pressure.Recent years have seen some 10 per cent ofpatients in acute care hospitals moved tolong-term settings. Even in cases where caregivers’patient workload has not increasednumerically, today’s residents have morecomplex health needs than ever before. ONAargues that residents in long-term care settingsshould have at least 3.5 hours of caredaily, of which 35 minutes should be suppliedby an RN. This is far from standardpractice in the sector.RNs working in <strong>Ontario</strong>’s 37 public healthunits also need more support. In June 2004,following recommendations contained in theCampbell and Walker reports on the impactof the SARS outbreak, the <strong>Ontario</strong> governmentlaunched a substantial, three-year publichealth action plan. But ONA is concernedthat precisely because of the prevailing financialarrangement for public health in theprovince, according to which cash-strappedmunicipalities have to provide 45 per cent offunding (according to government plans, thiswill decline to 35 per cent in 2006 and then25 per cent by 2007), nurses and other professionalsemployed in this sector find it difficultto fulfil their provincially mandated obligations.Shared funding, ONA believes, underminesthe financial base of public health andlimits the capacities of those assigned to provideit. In ONA’s view, the province shouldassume 100 per cent of the cost.Educating a new generation of nurses, andfinding them full-time jobs in <strong>Ontario</strong>Obviously, training new nurses is at least asimportant as encouraging larger numbers ofmore experienced professionals to remain inthe workforce for an extended period of time.According to Professor O’Brien-Pallas, severalnursing schools across the province havehit the ceiling in terms of new enrolments.Now, additional investment is specificallyrequired to expand infrastructure (labs, forexample), as well as hire professors. At theUniversity of Toronto, for example, a specialtwo-year fast-track program, designed to educate90 nurses, was created for holders of aBachelor of Science degree. At the government’srequest, 150 students were enrolled.Retirement projections and the nursing workforceA study conducted by the Nursing Effectiveness, Utilization and Outcomes Research Unit (NRU),University of Toronto, employs two methods to gauge the impact of provincial nursing attritionin the years leading up to 2008. Looking at retirement patterns and the age structure of thecurrent workforce, the authors of Stepping to Success and Sustainability estimate that between15,000 and 30,000 RNs will leave the profession by 2008, depending on whether they retire at55 or at 65.The authors also take population growth projections into account in order to predict howmany nurses will be required in order to meet the population’s hospitalization needs alone.Under this model, hospitals will be short anywhere from 5,000 to 6,000 full-time RNs. But thisis a misleadingly optimistic figure. Factoring in the growing complexity of the cases of thosepatients who stay in hospital (the acuity factor), the authors identify a nursing shortage in acutecare institutions of between 12,000 and 13,000 by 2008.In June 2005, <strong>Ontario</strong> Chief Nursing Officer Sue Matthews questioned whether retirementnumbers would in fact attain the levels predicted in the NRU study. Official data for 2004 wasnot however yet available.A copy of the Stepping to Success document can be downloaded from the McMaster Universitywebsite at http://www.fhs.mcmaster.ca/nru/documents/Stepping to Success and Sustainability2003.pdf.ONTARIO NURSES’ ASSOCIATION 19
Stories: The public and nurses talk about nursing in <strong>Ontario</strong><strong>Nurses</strong> touch the lives of almost all Ontarians. Many people have stories aboutnurses who made a difference, went the extra mile or eased some pain. These aresome of the stories collected on the <strong>Still</strong> <strong>Not</strong> <strong>Enough</strong> <strong>Nurses</strong> campaign website atwww.stillnotenoughnurses.ca.11/28/05RN<strong>Ontario</strong>I internationally trained, registered with theCollege of <strong>Nurses</strong> of <strong>Ontario</strong> and am job seekingat the moment, which seems to be futile. The funnything is there seems to be everyone saying there isshortage of nurses, but no one is hiring. I wouldthink employers would have been happy to grabnurses available, train them in their shortage areasand fill the gap instead of having that vacancy onhold all the while. For me investing in getting registeredin Canada is not worth it as you have to bea permanent resident, citizen or have permissionto work and employers hate waiting the long processto have a work permit. Is this country tryingto get nurses or chase them to the U.S. and othercountries? I would sure like to know.11/22/05MikeDundalk, <strong>Ontario</strong>Over the past 10 years, my wife had a major caraccident resulting in three months in Sunnybrookat all levels from ICU down, and four months atSt John’s rehab. I had heart surgery at TorontoGeneral with two stays at Orangeville hospitaltwo years ago. Over this time we met many greatnurses who went beyond their job descriptions tocare for us. We never forget them. I have noticedover this time the increased workload the nurseshave been subjected to, but in spite of all this theycontinue to provide me with the same high standardof care and the little acts of kindness that areso important when facing the prospect of a seriousoperation. Thanks to all of you who cared for me.Our hospitals need more FULL-TIME nurses.Write or e-mail your MPP or health minister andtell him.11/21/05Alicia, RNHamilton, <strong>Ontario</strong>I have been working for two years at a Hamiltonas a registered nurse. I have been working parttime without benefits and get called in as required.(sometimes one hour before shift). I am afraid toleave my house for more than one day because Imight miss a shift. I don’t always get enough shiftsto pay my rent, bills and student loans. There isno indication that I will be hired on full time in thefuture (they just cut back on beds on my ward). Ilike my job and enjoy my work but if things don’timprove I will be forced to look at other options.(There is no point moving to another hospital inCanada / others tell me they are all the same.)9/23/05TiberiusToronto, <strong>Ontario</strong>My story is similar to other nurses. I take solacein the fact that I’m not the only one in this situation.I am an RN who immigrated to Canada. Idid everything I had to, in the first year, to becomeregistered with College of <strong>Nurses</strong> of <strong>Ontario</strong>.And now... where is the job? I have applied to allof the hospitals in Toronto, and I didn’t get evenONE reply. I even went looking for the recruitersin person at the hospital, and I was told theywere unavailable because “they were in Englandto recruit nurses.” Is this a joke???? But it’s aboutpeoples’ lives...living a life for a new future. Ofcourse, like many others I have to reconsider mycareer, moving either to US, or back to Europe.The hospitals there will do anything to recruit RNs.The thing is that I love Canada.9/22/05I was a part time RN for many years. 3-1/2years ago I took a full-time position the hospitaloffered me. Now due to funding, I’m being reassignedto another site and my part-time co-workersare staying where I wanted to be the rest ofmy nursing career...9/21/05Lynn, RNPeterborough, <strong>Ontario</strong>I am an RN. Graduated 2004 and work in thecommunity as a visiting nurse for a nursingagency. I’m not new to the system, as I worked asan RPN for the same agency for 15 years. I amincreasingly seeing patients with more complex,acute needs resulting in longer time per visits, andmore need for advanced nursing skill and assessment.This environment has become more difficultto work in for the above mentioned reasons, aswell as the frustrating fact that our services areobtained through a Request for Proposal (RFP)process tendering out services, which causes biddingwars with other agencies. Add in the demographicsand geography involved in the community,the escalating price of gas, the price of vehicles,and it only adds to the failure to retain and recruithighly-trained nurses who are so desperately neededto care for our patients in the community. I seeexcellent nurses working in the community whocan’t take it anymore. We need more nurses, butconsidering what we are up against, as well as theshortage of nurses overall, I have a feeling thingsare not going to change anytime soon. It takes apassion and certain devotion to be a home carevisiting nurse, but that’s not even enough to get youthrough anymore. We are burned out.9/18/05Kelly, RNI am an RN and have been working in the nursingprofession for 16 years. I remember, not two yearsago when I would get up in the morning and lookforward to going to work. A few months ago I wasdriving to work and all that was going through myhead was “I hate my job.” I then thought, “Whathas happened in the last two years to drasticallychange my outlook?” Understaffing, increased acuityof patients with no change in patient to nurseratio, no appreciation of a job well done (but besure if anything was wrong you would hear aboutin a second), tired of being told by your boss whenunderstaffed to “just do the basics.” I don’t thinkthe boss or the public realizes the basics are allwe are able to do on a regular basis now. I used toknow all my patients’ names, and now all I knowis their room numbers. Many years ago when Iused to hear the term “burnout,” I thought “Well,that will never be me, I love my job.” Today I thinkI am only a few steps away from being burned out.This makes me very sad and very scared for thefuture of health care in <strong>Ontario</strong>.20 VISION, SPRING 2006
Patients MatterBut there isn’t room for any more, saysO’Brien-Pallas, without expanded capacity.Sue Matthews hesitates to generalize aboutthe problems confronting nursing schools,arguing that capacity isn’t exhausted provincewide. In any given year, she points out,some classrooms may be less than crowdedfor the simple reason that schools don’treceive an optimal number of qualified applicants.But <strong>Ontario</strong>’s top nursing bureaucratdoes acknowledge that arranging clinicalplacements for students is a problem everywhere.She also admits that faculty is aging;lack of professors, she says, is indeed a pressingissue, before adding that the governmentis attempting to address this matter by providingtuition incentives to RNs who elect topursue graduate degrees and teach.Financial resources to improve staffing inhospitals and in other health care facilitiesNaturally, government can recognize thestaffing shortage in the system, assert it isdoing what it can to alleviate the situation,and then declare that money simply isn’tavailable to hire all the nurses (and otherstaff) necessary.But like other unions, ONA is skepticalabout fiscal strategies that make deficitreduction the chief budgetary priority. Thegovernment’s current budget deficit of lessthan $2 billion is hardly alarming. <strong>Ontario</strong>could allow it to grow somewhat in order toensure that its health care system is properlystaffed and equipped – without generatingadverse economic effects.So what should be done? ONA will makeits case to the government as effectively as itcan. But nurses need individual citizens,community groups and other unions to joinin a common campaign. The public must letQueen’s Park know that certain measuresmust be taken immediately in order to staveoff the worst effects of a nursing shortage.Politicians, pressured by a variety of interests(some far more committed to cutting spendingand privatizing services than ensuringquality health care for all), will undoubtedlyneed a strong push in the right direction. Tothat end, it is time for Ontarians to exerttheir collective energy.Employment prospects for recent gradsBy September 2004, according to an interim McMaster University report, of the 41 per cent ofthat year’s nursing graduates who had found employment, only 36.5 per cent had full-time jobs,although the vast majority wanted this type of work.Graduates’ impressions of the job market were telling: many regarded <strong>Ontario</strong> as offeringplenty of nursing opportunities to those willing to take part-time contracts and casual arrangements.Indeed, data from the College of <strong>Nurses</strong> of <strong>Ontario</strong> reveal that fewer than 60 per cent ofprofessionals presently working in the province have a full-time job.Meanwhile, the United States is seen as the country where desirable employment is available;more than one-quarter of the McMaster respondents declared their readiness to seek and acceptwork there. Of the 82 graduates who identified the U.S. as their preferred employment destination,more than 80 per cent were already working full-time in that country.In short, Educated and Underemployed: the Paradox for Nursing Graduates, suggests there issome truth in the suggestion that provincial nursing schools are serving as suppliers for Americanhospitals. Most (not all) <strong>Ontario</strong> grads want to work here. But the doors to full-time employmentin <strong>Ontario</strong> seem ajar at best.ONTARIO NURSES’ ASSOCIATION 21
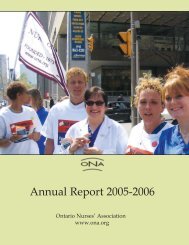
Patients Matter74.7Ratio of Registered<strong>Nurses</strong> to Ontarians69.51994 year200430,000What you can do to help• Learn about nurses’ status and the state of our health care systemin general.• Write a letter to your MPP, to the Premier or to the Minister ofHealth and Long-Term Care.• Write to your local newspaper supporting the campaign for morenurses now.• Sign a <strong>Still</strong> <strong>Not</strong> <strong>Enough</strong> <strong>Nurses</strong> postcard or an e-postcard on thecampaign website at www.<strong>Still</strong><strong>Not</strong><strong>Enough</strong><strong>Nurses</strong>.ca• Click on the section of the website that has stories and commentsfrom nurses and the public. Post your own story andcomments about what it’s like to work in the <strong>Ontario</strong> health caresystem under current conditions.• Put on a campaign button or stick the message on your car.• Attend an ONA rally, public forum or other <strong>Still</strong> <strong>Not</strong> <strong>Enough</strong><strong>Nurses</strong> event.• Let your employer know about your concerns.• Talk to your friends and co-workers about what can be done toimprove your working conditions.• Encourage your family and friends to follow all the steps outlinedabove, including wear a campaign button, write letters insupport of nurses to their local newspapers and elected representatives,and post their own stories in support of nurses onthe campaign website.Predicted numberof Registered<strong>Nurses</strong> leavingthe workforce in<strong>Ontario</strong>10,000113,000Predicted shortageof nurses in Canada78,0002006 year20082011 year2016SOURCE: CIHI, Health Indicators and the <strong>Ontario</strong> College of <strong>Nurses</strong>.<strong>Ontario</strong>’s health spending gapAccording to economist Armine Yalnizyan, Queen’s Park will, over afour-year period (2005-2008), take in slightly more than $20 billion inrevenues available for health care – fully $9.3 billion from the provincialhealth premium.But spending during this time-frame, including totals detailed in the2004 budget, last autumn’s Economic Outlook and Fiscal Review andthe 2005 budget, is just over $19 billion, leaving a “gap” of $1.14billion.ONA fears that, under current plans, an important amount of moneywill not be used as it should be – to improve <strong>Ontario</strong>’s health caresystem.22 VISION, SPRING 2006
First Vice-President’s MessageVicki McKennaONA First Vice-PresidentUnions’ “Stop LHINs” campaign goes full speed aheadONA and three other major provincial unions have reaffirmedtheir commitment to stop the <strong>Ontario</strong> government’s implementationof Local Health Integration Networks (LHINs) legislation as currentlydrafted.ONA, CUPE, SEIU Local 1.on and OPSEU, representing more than200,000 workers across <strong>Ontario</strong>’s health care spectrum, met in earlyJanuary to cement a coalition and to plan activities around their “StopLHINs” campaign.The gist of the campaign is this: We will not let the provincial governmentdestroy our health care system and take our jobs.The unions are alarmed at the <strong>Ontario</strong> government’s determinationto rush through legislation, possibly as soon as March, that ultimatelywill diminish access to local health care and community-based socialservices, threaten stability for thousands of health care workers andopen the door to private for-profit corporations and reduced localcontrol.Integrating health services should lead to better coordination,reduced wait times, improved access to appropriate health servicesand providers, reduced costly government bureaucracy, and safe,quality health care, but the government’s LHIN plan is deeply flawedand will cause chaos in the health care system. The government’splan is about rationing patient care and saving money.In ONA’s view, the government’s approach:• lacks comprehensive planning to deal with employees in a waythat protects jobs and improves patient care.• threatens access to local health services.• reduces accountability by placing decision-making at arm’slength from the government.• ignores the role of doctors as “gatekeepers” of the system.• takes away local control; allows no input from front-line staff.• could extend the disastrous competitive-bidding model nowused in home care to the entire health care system.• is driven by the bottom line, not health care concerns.Under the Local Health Integration Act (Bill 36), LHINs appoint 14regional boards to spend two-thirds of the province’s health care budget– about $20 billion. These hand-picked boards are appointed andaccountable to the McGuinty government – not the community.The Ministry of Health will have total control in every <strong>Ontario</strong>community. Instead of funding badly needed front-line workers inhealth care, the legislation creates a massive and expensive bureaucracy.LHIN boards have the authority to transfer, merge, amalgamate or“wind up” services, or the government will step in and do it for them.This means the future loss of more services and more jobs.Despite claims it will better “align” health services, many criticalparts of the health care system are left outside the new structure,including physicians and some laboratories, public health and ambulances.The government also intends to offer many health and socialservices for tender – much in the way the disastrous competitive biddingprocess is applied in home care – with the private sector invitedto bid for these services.Competitive bidding in home care has dramatically increasedcosts, diminished quality care and driven workers out of the sectorbecause of lower wages, fewer benefits and a lack of job security. Ithas put non-profit providers like St. Elizabeth Visiting <strong>Nurses</strong> and theVictorian Order of <strong>Nurses</strong> out of the business of providing in-homenursing services in many communities, because they can’t competewith the underbidding of for-profit corporations. This has severelyimpacted on many of our community-based home visiting nurses.The 2006 phase of the LHIN campaign began with 17 meetingsacross <strong>Ontario</strong> in January to educate grassroots membership in allfour unions on the impact this legislation will have on job securityand patient care. Media conferences were held in each city prior tothe meetings to talk about the LHIN campaign.Other activities included:• A pamphlet was developed detailing the unions’ concernsabout LHINs.• ONA led meetings in Windsor and Ottawa, and at least oneONA Board member attended each of the 17 meetings.• ONA made presentations at the four public hearings held inJanuary and February by the province’s Standing Committee onSocial Policy looking at Bill 36.• Information pickets were held across the province on February14.• ONA held a special meeting on January 13 for LocalCoordinators and Bargaining Unit Presidents to discuss thecampaign.• Representatives from the four unions, including ONA ChiefExecutive Officer Lesley Bell, RN, met with the editorial boardof the Toronto Star to talk about the issues.For more information, visit the campaign website at www.stoplhins.ca.This fight is just heating up!ONTARIO NURSES’ ASSOCIATION 23
QUEEN’S PARK UPDATEONA participates in provincialFinance roundtableONA President Linda Haslam-Stroud, RNjoined a round table discussion with <strong>Ontario</strong>Finance Minister Dwight Duncan and over100 other interest groups in December 2005,in preparation for the Spring provincialbudget. Haslam-Stroud spoke on a varietyof issues, such as: linking economic growthand productivity in the industrial sector tohealth care, with safe working environmentsleading to healthier and more productiveworkers, and cost savings; the high cost ofill and injured nurses; utilization rates fornurses, i.e., a 93 per cent workload capacityleads to increased illness and injury; the needfor legislation mandating the use of safetyneedles and other sharps; strengtheningoccupational health and safety regulations;the need to protect nurses and other healthcare workers from violence in the workplace;external challenges facing health careworkers, i.e., SARS/flu pandemic, the needto appropriately fund and be proactive in thearea of public health regarding preventionof illness/disease and public education;accountability and transparency with respectto targeted funding, i.e. Fiscal AdvisoryCommittees not functioning; the need fortargeted funding for recovery room, surgicaland operating room nurses to increase ORcases and decrease wait times; it is nowbeing realized that RNs provide good valuefor money, after the period in the 90s whenrestructuring meant nursing layoffs, withresearch strongly indicating that appropriatenurse staffing levels mean reduced morbidityand mortality rates; retention and recruitmentof nurses will provide a solid base forproviding health care.<strong>Ontario</strong> CCACs to align withLHIN boundariesThe provincial government is proceedingwith its controversial plan to introduce 14Local Health Integration Networks (LHINs),which will determine and eventually fundthe delivery of health care services in<strong>Ontario</strong>. Introduced on November 24, 2005by Health Minister George Smitherman,Bill 36, the Local Health System IntegrationAct (2005), also realigns the 42 existingCommunity Care Access Centres (CCACs)with the boundaries of the 14 LHINs. Thegovernment has indicated all existing CCACoffices will remain open and that CCACboards will again be permitted to select theirboard members, rather than being appointedby government. ONA represents membersin 32 CCACs and although the offices willremain open, our members’ employers maychange. ONA is awaiting the final dispositionof the proposed legislation to assessthe labour relations issues that will have tobe addressed to insure a smooth transitionfor ONA members. In January 2006, ONAmade oral presentations to the StandingCommittee on Social Policy regardingamendments to Bill 36, and followed theoral presentations with a written submissionto the Committee. The legislation is multifacetedand will have a far reaching affecton health care in <strong>Ontario</strong>. Refer to the FirstVice-President’s column in this issue of ONAVision on paage 23 for an update on all ofONA’s activities regarding LHINs. For moreinformation on LHINs, visit the government’swebsite at www.lhins.on.ca. You can also readmore about ONA’s position on our website atwww.ona.org.<strong>Ontario</strong> Health Coaltion tochallenge private clinicsThe <strong>Ontario</strong> Health Coalition (OHC) ofwhich ONA is an active member, is mountinga challenge to private clinics opened in earlyJanuary by Copeman Healthcare Inc. Theclinics will charge OHIP, as well as additionalout-of-pocket initiation fees of $1,200,plus $2,300 annual dues, for enhanced or“boutique health services.” Private clinicsviolate principles of Medicare, cost more andtake doctors away from the public healthcare system.Mandatory retirement billpassesBill 211, legislation amending the <strong>Ontario</strong>Human Rights Code and other Acts to endmandatory retirement, received RoyalAssent on December 12, 2005. It comesinto effect one year later, on December 12,2006. The transition period is designed togive employers time to adapt their humanresources policies and practices to complywith the law. Until the law comes into effect,current rules regarding mandatory retirementremain in place, and employers can requireemployees to retire at age 65. The law amendsthe Human Rights Code to protect employeesaged 65 or older from being forced to retire,except in those cases where mandatoryretirement could be justified as a “bonafide occupational requirement” determinedunder the Code. ONA will monitor the effectsof this legislation on members. In a positionstatement developed in October 2004, theONA Board of Directors indicated ONAopposes any action or initiative on the partof employers or government that is intendedto force nurses to work beyond normalretirement age, including any increase to theminimum age to qualify for social securityand other retirement benefits. ONA’s positionstatement is on our website at www.ona.org.Government consolidatescataract surgeryThe provincial government announcedon January 9 that 1,700 annual cataractprocedures will be moved from UniversityHealth Network, Mount Sinai, St. Michael’sand Sunnybrook to the Kensington EyeInstitute. As well, the new facility is expectedto perform 5,000 additional routine cataractsurgeries annually. The Kensington EyeInstitute is a not-for-profit corporationlicensed as an independent health facility,with operating funding in the amount of$5 million annually provided by thegovernment. ONA is keeping a close eye ondevelopments that move acute care servicesout of hospitals and into the community.24 VISION, SPRING 2006
QUEEN’S PARK UPDATEFunding to expand CommunityHealth CentresTwenty-two new Community HealthCentres (CHCs) and 17 new satellite CHCswill receive $74.6 million in funding overthree years. Currently, there are 54 existingCHCs and 10 satellites across <strong>Ontario</strong>.In addition, existing CHCs will receiveextra funding for staffing and programenhancements, including ONA-representedsites.Long-term care beds added toease pressures on hospitalsThe provincial government is awardingan additional 204 interim long-term carebeds across <strong>Ontario</strong> to expand services topeople who no longer need acute hospitalcare and relieve pressure on hospitals.The interim beds complete the McGuintygovernment’s $29.2-million AlternativeLevels of Care strategy commitment of 500interim long-term care beds announced inFebruary 2005.Wait times targets set; fundingfor equipment flowsThe provincial government has set waittimes targets in five areas: cancer surgery,cardiac bypass surgery, cataract surgery, hipand knee replacement, and MRI/CT scans.Details on the wait times are availableat www.ontariowaittimes.com. To supportthese wait times targets, $74 million hasbeen committed to cancer radiation anddiagnostic equipment, and an additional$83.5 million in other diagnostic and medicalequipment. The funding is part of the$198.3 million in federal funding providedto <strong>Ontario</strong> for 2005-06. These funds includea further $29 million for the purchaseof mechanical patient/resident bed lifts inhospitals and long-term care homes. ONAis working with <strong>Ontario</strong>’s Chief NursingOfficer to review how previous funding forpatient lifts and safety-engineered medicaldevices has been implemented.Funding to upgrade and repair public hospitalsPublic hospitals have been promised $60 million in capital funding in 2005-06 for highpriority upgrades and repair projects. Flowing from the government’s Health InfrastructureFund, the minimum grant will be $150,000 per site of all public hospitals. Examples of thetypes of repairs to be funded include: building and fire code upgrades, structural repairs,upgrading heating and ventilations systems, and upgrading back-up generators. These repairswill also improve health and safety conditions for ONA hospital members, however they needmore than bricks and mortar.“Capacity review” to assess effectiveness of public health servicesThe provincial government has released an interim report of the Capacity ReviewCommittee looking at the delivery of public health services in <strong>Ontario</strong>. The review wasset up in January 2005 by the provincial Chief Medical Officer of Health to undertake a“comprehensive assessment” of public health in <strong>Ontario</strong>, with a view to possible restructuring.Areas under review include core capacities at the local level; staffing (recruitment, retention,education and professional development); governance, operation and systemic issues; andmechanisms to improve systems, programs and financial accountability. ONA is developingstrategies to deal with public health restructuring, which is currently not covered under Bill36, Local Health Integration Networks (LHINs) legislation.ONA to co-manage provincial nursing trust fundto help keep hospital nurses working longerONA will be co-managing a new $40-million trust fund for hospital nurses,announced on January 26 by the Ministryof Health and Long-Term Care (MOHLTC).ONA will form a management committeewith the Registered <strong>Nurses</strong> <strong>Association</strong>of <strong>Ontario</strong> (RNAO) and the RegisteredPractical <strong>Nurses</strong> <strong>Association</strong> of <strong>Ontario</strong>(RPNAO) to administer the funding. ONAPresident Linda Haslam-Stroud, RN, andChief Executive Officer Lesley Bell, RN,will sit on the board for ONA.“We’re very pleased the Ministry issupporting the retention of nurses inhospitals across <strong>Ontario</strong>,” said Haslam-Stroud.“This is a concrete step that will assist inproviding quality care for our patientsduring <strong>Ontario</strong>’s nursing shortage. Wehope this funding will support nurses ifthey don’t have the skills, qualificationsor training to attain employment in aspecialty or other areas.”The funding will:• provide opportunities for nursesto expand their knowledge andtraining so they can work in otherclinical areas or nursing roles withintheir hospital when there arevacancies.• be available for both registerednurses and registered practicalnurses.• reimburse hospitals for costsincurred for up to six months oforientation, training and educationthat increases the clinical skills andexpertise of nurses.The funding aims to stabilize the nursingprofession by improving access to fulltimeemployment opportunities andenhancing working conditions for nursein <strong>Ontario</strong> hospitals.The first step will be to develop anapplication process and criteria forhospitals wanting to access the fund.ONTARIO NURSES’ ASSOCIATION 25
Understanding the 2% wage increase forhospital nurses with 25 or more years of serviceThe Keller award for ONA members working in the hospital sector brought nurseswith 25 years of service a 2-per-cent wage increase, effective January 1, 2006.This new inclusion in the central hospital collective agreement has sparkedquestions from ONA senior nurses, particularly in terms of what the 25-yearexperience rate is based on, and how they calculate their years of service.The information here will help clarify the issue. If you have further concerns orquestions on this issue, contact your bargaining unit president.BackgroundONA requested clarification from the KellerArbitration Board concerning the new 2-percentincrease for nurses with 25 years experience.Arbitrator Brian Keller advised theparties, both ONA and the <strong>Ontario</strong> Hospital<strong>Association</strong> (OHA), that his intention was tocreate a new 25-year rate as part of the existingsalary grid structure.<strong>Nurses</strong> would advance on the grid in themanner currently set out by the collectiveagreement in Article 19.05, which is a combinationof current service with the hospitaland recognition of experience prior to thenurses’ hire date.Keller acknowledged that proving past experiencewould be problematic for many nurses,and indicated the determination should bebased on the best evidence available.Determining who qualifiesKeller made it clear that only those nurseswho are currently at the maximum rate onthe salary schedule would qualify for the new25-year rate. In other words, if an employeehad 25 years of experience but was currentlyat the “after 2 years” rate, she or he wouldnot qualify for the extra 2 per cent.While ONA hopes it is not common tofind 25-year nurses being paid at the 2-yeargrid level, Article 19.05 does leave open thatpossibility. This is because the employerhas the discretion to recognize, or not recognize,the experience of nurses returningto employment who have been out of theworkforce for two or more years.26 VISION, SPRING 2006This is one of many areas the new HospitalCentral Negotiating Team (HCNT) willexamine in the next round of negotiations.Neither ONA nor the OHA proposed the25-year rate, but rather it was the arbitrator’sprovision. Keller was clear he intended thisto be a “retention” provision. Retention was,and continues to be, a priority for ONA.How the new rate is administeredONA believes the only practical way toadminister the new provision is to base experiencesolely on each nurse’s year of graduation.That would circumvent the problemsthat nurses have in obtaining proof of theirexperience.Although Keller claimed to understandthis verification problem, he rejected thisposition and instead suggested it be based onthe best proof available.The following is a list of possible proof ofexperience that may be used in some circumstancesby members: statement of experience;application for employment; application fora job posting; resumé; tax records; pensionrecords; letters of employment; letters of reference;RN regulatory body records.In ONA’s view, this should include takingthe nurse’s word for the fact that she or hehas that level of experience. This will beanother bargaining issue to be dealt with inthe upcoming round, as ONA wants to avoidputting nurses through the frustrating andsometimes demeaning task of verifying theirservice record.Getting the employer to complyProceeding to arbitration can lead to unexpectedconsequences. The 25-year rate is agood example, perhaps, of good intentionsgone awry. It also reconfirms the adage thata negotiated deal is always preferable to onethat is imposed by an arbitrator. However, ittakes two to bargain, and the OHA was not awilling partner in the last round.Fortunately, the employer does not have thelast word on whether members will or will notbe paid at the 25-year rate. We have a grievanceand arbitration system that can forcethe employer to comply. If your employer isnot applying the agreement, including Article19.05, in a consistent, fair or proper manner,you need to bring this to the attention of yourBargaining Unit President and commence thegrievance process.The HCNT will consider feedback andquestions from members on this issue asbackground and support for negotiations inthe next round.For more information on this issue,visit ONA’s website at www.ona.org in theMembers’ Section, and click on the link,“Hospital Sector Award FAQs.”
AWARDS AND DECISIONS SUMMARYRights Arbitration AwardsLaying off RNs to hire RPNs not consistent with quality careONA & The Scarborough Hospital(Keller, November 17, 2005)The employer announced it was implementing“skill mix changes” on variousunits. On one unit in particular, thismeant laying off registered nurses (RNs)and introducing registered practical nurses(RPNs). Applying Article 10.12(a), thearbitrator ruled that the assignments“might be appropriate,” in the sense thatthey were within the RPNs’ scope of practice.However, the employer must alsoprove that the reassignment was “consistentwith quality patient care.”A study presented in evidence by theemployer was given little considerationsince it was general in nature; those whoprepared it spent only 2.5 hours on the unitin question. The employer appeared to havemade its decision based on the situation onother floors, and did not make an in-depthHealth unit’s flu policy is subject to Charter of RightsONA & Eastern <strong>Ontario</strong> Health UnitPreliminary award (Chodos, October 25, 2005)ONA planned to rely on the Charter ofRights and Freedoms in this grievance of theemployer’s policy concerning staff immunizationagainst influenza. Typically, theCharter does not apply to ONA employers;it only applies if the employer can be characterizedas “government.” In this groundbreakingpreliminary decision, the arbitratorreviewed several court decisions, statutesand other factors, and concluded that thehealth unit is an arm of government and istherefore subject to the Charter. The arbitratorwill now continue to consider whetherthe policy violates our members’ rights tosecurity of the person under Section 7 of theconsidered study of this unit and the effectit would have on the quality of patient care.ONA’s evidence showed the unit had highlycomplex, unpredictable patients with ahigh level of acuity. Care needs are notwell defined and subject to change; close,frequent monitoring is required.The arbitrator concluded that, “On theRN/RPN, continuum, this scenario does notpermit that RPNs be added to the skill mix.This fits within the model of an RN providingcare alone...the employer violated Article10.12(a) at the time of the grievance as Iam not satisfied, based on the evidence, thatquality patient care would have been maintainedwith the skill mix proposed.”The grievance was allowed. The hospitalmay not proceed with its proposed skillmix change and the layoff notices are to berescinded. This is the first significant decisionon the meaning of Article 10.12(a).Charter, and if so, whether such a violationis a “reasonable limit prescribed by law ascan be demonstrably justified in a free anddemocratic society.”“Purpose” of replacing full-timewith part-timeONA & Hotel-Dieu Grace Hospital(Crljenica, September 11, 2005)This grievance involves the interpretationof Article 10.12(a), which states, “…workperformed by full-time nurses will not beassigned to part-time nurses for the purposeof eliminating full-time positions.” In particular,it involves the meaning of “for the purposeof.” Several full-time nurses voluntarilyleft their positions, which the employer filledby posting part-time positions as part ofcost-cutting measures. The arbitrator ruledthis violated Article 10.12(a), which prohibitsthe hospital from eliminating full-timenurses and assigning their work to part-time,even if their purpose is cost-cutting, re-balancingor patient care.Enforcement of collectiveagreement notice pay andseverance payONA & Access Health Care Services Inc(Chapman, October 11 & November 2, 2005,Superior Court of Justice, December 15, 2005)The local Community Care Access Centre(CCAC) terminated the employer’s contractto provide home health care services onshort notice; the employer then gave inadequatenotice of permanent layoff to thenurses and ONA. <strong>Nurses</strong> availed themselvesof the collective agreement right to resignduring the notice period yet maintain eligibilityfor two weeks of severance per year ofemployment, but the employer paid neitherseverance nor notice pay. The arbitratorrejected the employer’s arguments that thecollective agreement gave employees theright to accelerate severance pay only incases of “long-term layoff,” not the “permanentlayoff” that had actually happened, andallowed the grievance. ONA, aware of theemployer’s financial situation, took steps toquantify the amount owing – over $130,000,plus all required contributions to HOOPP.When ONA proceeded to collect the moneythrough garnishment, the employer filedfor judicial review of the arbitrator’s awardand sought a stay of the order to pay untilthat was finished. Before the court, ONAwas willing to accept payment of the totalamount into court instead of garnishment.This was enough for the court to deny theemployer’s stay application.ONTARIO NURSES’ ASSOCIATION 27
AWARDS AND DECISIONS SUMMARYAgreement prohibits elimination offull-time positionONA & Daimler Chrysler Canada(Crljenica, October 23, 2005)The planned closure of part of the employer’soperations was a major theme in the last roundof negotiations. ONA sought and gained aguarantee that it would not lose a full-timenurse position as a result of that closure. Threemonths after negotiations were concluded, theplant in question closed. Later that year, theemployer gave notice it would be reducingthe full-time staff complement by one fulltimenurse, effective January 1. The arbitratoragreed with ONA’s position that the employer’sdecision to eliminate the full-time job was aviolation of that specific provision, as well asother ones setting rules for reducing full-timestaff. As a result, the arbitrator ordered theemployer to reclassify the grievor, whose statushad been changed to part-time, back to fulltime,and compensate her for losses.Interest Arbitration AwardsONA allied members secure ratesof pay amongst highest in provinceCommunity Lifecare (Port Perry)(Arbitrator Jolliffe, October 21, 2005)The employer proposed setting rates for RPNsand Health Care Aides (HCAs) based on theaverage rates across the province for nursinghomes among all unions. This bargaining unithad rates that were near the top end of therange, and sought to keep their relative standing.The employer argued that a total compensationmodel should be applied, and that ratesof pay should be discounted on the basis thatsome employer savings achieved in SEIU bargainingwere not available in this bargainingunit. ONA resisted such discounting except inrelation to percent in lieu, which was reducedfrom 7 per cent to 6 per cent. This reductionenabled the members to retain their shift28 VISION, SPRING 2006premium payment, even though there is norotation requirement. In most other serviceunits, shift premium is only paid if rotation isrequired. Even with the reduction, part-timeemployees still get a superior benefit packageas in addition to the 6 per cent in lieu, theyreceive holiday pay as well as employer contributionsto their RRSP.Transfer of authority does notinterfere in finalizing collectiveagreementRainycrest District Home for the Aged(Arbitrator Devlin, November 23, 2005)One month after the interest arbitrationboard issued its award at this home, andbefore a collective agreement document wassigned incorporating the award, the districttransferred authority to operate the home tothe Ministry of Health and Long-Term Care.Once ONA put together the collective agreementdocument, neither the district, nor theMinistry or its agent, agreed to sign. ONAapplied to the arbitration board to exerciseits legal authority to issue a document thatwould constitute the collective agreement,even without an employer signature. The districtchallenged the jurisdiction of the arbitrationboard to exercise its authority in thiscase, because of the transfer of the operationof the home to the Ministry. The position wasbased on the argument that the governmentisn’t bound by the <strong>Ontario</strong> Labour RelationsAct (OLRA) or the Hospital Labour DisputesArbitration Act (HLDAA). ONA argued thatany events subsequent to the issuance ofthe initial HLDAA award were irrelevant,and pointed out that if the district was correct,the barrier to getting a signed collectiveagreement wouldn’t just exist where transfersof the operation of the home were made togovernment. Because of the Harris governmentamendments, the sale of a home to anynon-government entity would also preventthe finalization of a collective agreement. Thearbitration board adopted ONA’s view thatthe key date was the date of the initial award.Since on that date the district still operatedthe home, the Board did have the power to“order up” the collective agreement.Parity with hospitals includes extraincrementGlen Stor Dun Home for the Aged(Arbitrator Knopf, December 27, 2005)The parties had a prior history of hospitalparity and had renewed their agreement inadvance of the September 8, 2005 hospitalHLDAA award with a “Hospital me too.”Following the Keller award, this employerrefused to implement the extra increment of 2per cent for employees with 25 years’ experience,on the grounds there was no need for aretention bonus. The board rejected this characterizationof the Keller award, and ruled theextra increment was an integral componentof the hospital grid, which the parties at GlenStor Dun had agreed to adopt in advance.WSIB DecisionsPost-traumatic mental stressrelated to SARS allowedHospital Sector in South District(June 29, 2005)A nurse became emotionally ill as a resultof witnessing many co-workers become sickwith SARS. She feared for her own health andher family’s health. WSIB denied entitlementand benefits because, in their opinion, WSIBpolicy did not allow entitlement to mentalstress where it arises from a normal partof the working environment. WSIB claimedsince nurses deal with infectious disease on aregular basis and since SARS was an infectiousdisease, the policy did not allow for them togrant entitlement. In written submissions andat the hearing, ONA demonstrated the workeris entitled to benefits for mental stress that isan acute reaction to a sudden and unexpected
AWARDS AND DECISIONS SUMMARYtraumatic event, arising from her employment.The appeals resolution officer (ARO)determined medical evidence supported theclaim the worker did suffer a post-traumaticstress event from April 3, 2003 that continuedfor the duration of the disability, and thatthis worker’s experience with SARS was notnormal for the purposes of exclusion. Theworker was awarded WSIB entitlement for alllost time and health care benefits.Labour Market Re-Entry notsuitable for severely disabledworkerHospital (South District)(August 4, 2005)A highly active nurse was severely injuredwhen assisting in transfer of a patient to achair. She sustained two herniated discs, followedby emergency surgery. She had postoperativecomplications, and further surgerydiscovered a guide wire used to insert acentral line in the first surgery had not beenremoved. As a result of the injury, surgeries,complications and re-injury when attendingLabour Market Re-Entry (LMR), the nursemust now wear a leg brace and has assortedother impairments. Her WSIB claim wasallowed, and she was awarded a 50 per centNon-Economic Loss (NEL) award for her permanentimpairments. Despite this high award,WSIB determined the nurse could return towork, and ordered she engage in a programof learning to become an occupational healthand safety inspector. Despite her inability tosit and complete course assignments and meetdeadlines, WSIB pressured the nurse to persistin her studies at home. ONA argued theLMR program was not suitable, and that theworker was unemployable. After consideringthe evidence, which included a Ministry ofLabour physical-demands analysis proving thework of an inspector is unsuitable, the WSIBfinally relented, terminated her LMR program,declared her “unemployable” and granted fullLoss of Earnings (LOE) benefits to age 65.LTD Internal Carrier AppealsWhat is appropriate treatment foraddiction?Hospital in West District(October 5, 2005)A member suffering from major mental healthdisorders experienced a severe reaction to afamily matter. She was ultimately requiredto stop working. Shortly after, she sustainedinjuries in a fall. She followed recommendedtreatments for all her conditions. When shewanted to return to work, the employer askedher to see an addiction specialist. The specialistfound no reason for her not to return, but shewas subsequently sent home for suspected substanceabuse. She acknowledged a problem andrequested counseling. She saw the same specialist,who found that increased substance abusewas resulting in signs of illness. After treatment,she returned to work with reduced and thenfull-time hours. Her claim for LTD benefits wasdenied for lack of supporting medical evidenceand for failure to follow the specialist’s initialsuggestion that she seek in-patient treatment.ONA argued the community-based treatmentprogram finally agreed to between the specialistREGION 3Local 24Naomi AmoahJanet BookerLilliana ClarkeLynne HeeneyKaren HickeyGail KingPatricia McKennaGwendolynO’Brien-ReidMariammaVargheseand the member was appropriate for her needsand functioning, and that it was successful. Theargument succeeded.OLRB DecisionsONA RETIREESLocal 43Mary BantMary E. BellLorna BissLucia ChanBina DooPam FerrisLiz FisherJanis HuntCarmen JacksonAllison KellettLynda KingBrenda KirkpatrickDarlene KlineVictory concerning handling ofpatients from prisonOPSEU & ONA v Centre for Addiction and MentalHealth (CAMH)(OLRB, September 1, 2005)On August 3, 2005, a Ministry of Labouroccupational health and safety inspector madeorders against CAMH relating to the CollegeStreet site, prohibiting CAMH from accepting“forensic patients” (from jail) in a site notdesigned to handle them safely, and by employeesnot given specific training in dealing withthem. The employer appealed the orders andasked the board for an expedited procedure tosuspend the orders until the appeal is heard.The OLRB rejected the employer’s request onthe basis that it would likely create a dangerto worker health and safety. ONA and OPSEU,acting together in this matter, are now dealingwith the employer’s appeal.Dorothy MaherLynda MochrieMarilyn NellesAgnes PatersonSusan PeelCarolyn RappEileen RideoutJanice RobbinsPatricia SilcoxDorothy SterlingGrace SylvesterLynette Thomas-DevonishJean ThompsonREGION 4Local 7Dawn GeorgeLorri PattersonTerri-Lynn SmithJudith Spohn-GairRose-MarieThompsonLocal 75Pauline ClarkJudith MatthewsONTARIO NURSES’ ASSOCIATION 29
Membres de l’AIIO –Comment participer aux équipes deprojets et aux groupes de discussionFormulaire d’expression d’intérêt (membres)Équipes de projets spéciaux/groupes de discussionSelon la rétroaction des membres, nous avons mis au point unprocessus vous permettant d’exprimer votre intérêt à participer auxéquipes de projets spéciaux et groupes de discussion de l’AIIO.Ceci donne la chance de vous impliquer dans les décisions etprocessus de l’AIIO. Veuillez remplir le formulaire et le renvoyer à :Organizational Learning, 85, rue Grenville, bureau 400Toronto (<strong>Ontario</strong>) M5S 3A2 - Télécopieur : 416 964-8864<strong>Not</strong>e : Le Formulaire d’expression d’intérêt n’est valable quejusqu’au 31 décembre de l’année où il est présenté.Veuillez soumettre les nouveaux formularies pour 2006.Domaine d’intérêt n Provincial n Localn Droits de la personne/équité n Relations de travailn Santé et sécuritén Éducationn Financen Action politiquen Exercice professionnelBesoin d’une personne par régionn Vision / Semaine des soins infirmiers n Électionsn Équipe de consultation LEAPExpliquez brièvement les raisons pour lesquelles vous êtesintéressée à participer à une équipe de projet spécial ou à ungroupe de discussionONA Members –How to get involved with projectteams and focus groupsExpression of Interest Form (Members)Ad Hoc Project Teams/Focus GroupsBased on membership feedback, we have developed a process thatwill enable you to express your interest in serving on ONA ad hocproject teams or focus groups. This provides an opportunity foryou to be involved in ONA decisions and processes. Pleasecomplete the form and return it to:Organizational Learning, 85 Grenville Street, Suite 400Toronto, ON M5S 3A2 - Fax: (416) 964-8864<strong>Not</strong>e: The Expression of Interest form is only valid untilDecember 31 st of the year submitted.Please submit new forms for 2006.Area of Interest n Provincial n Localn Human Rights/Equityn Labour Relationsn Health and Safetyn Educationn Financen Political Actionn Professional PracticeNeed one person per regionn Vision/Nursing Weekn Electionsn LEAP AdvisoryPlease provide a brief statement telling us why you areinterested in serving on an ad hoc project team or gettinginvolved in a focus groupDate de présentation :Région : Local : Unité de négociation :Nom :Adresse :Ville : Province : ON Code postal :Tél. : (Bureau)Tél. : (Domicile)Secteur : n Hôpital n Foyers n Communautaire n CASCn Santé publique n VON/SEN n (Autre)n Professionnels paramédicauxStatut : n Plein temps n Temps partielDomaine d’exercice actuel :Date Submitted:Region: Local: Bargaining Unit:Name:Address:City:Province: ON Postal Code:Phone: (Bus.)Phone: (H.)Sector: n Hospital n Homes n Community n CCACn Public Health n VON/SEN n (Other) n AlliedStatus: n Full-Time n Part-TimeCurrent Area(s) of Practice:Expérience/antécédents à l’AIIO :ONA Experience/Background:30 VISION, SPRING 2006:
ONTARIO NURSES’ ASSOCIATION 31
ONTARIO NURSES’ ASSOCIATIONwww.ona.orgONTARIO NURSES’ ASSOCIATIONSuite 400, 85 Grenville StreetToronto ON M5S 3A2Canadian Publicaton Mail Sales Agreement No. 4006910832 VISION, SPRING 2006