Filling out Claim Form UB-04 - TRICARE Overseas
Filling out Claim Form UB-04 - TRICARE Overseas
Filling out Claim Form UB-04 - TRICARE Overseas
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
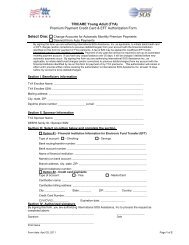
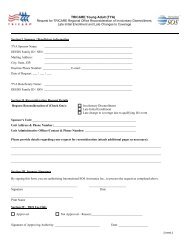
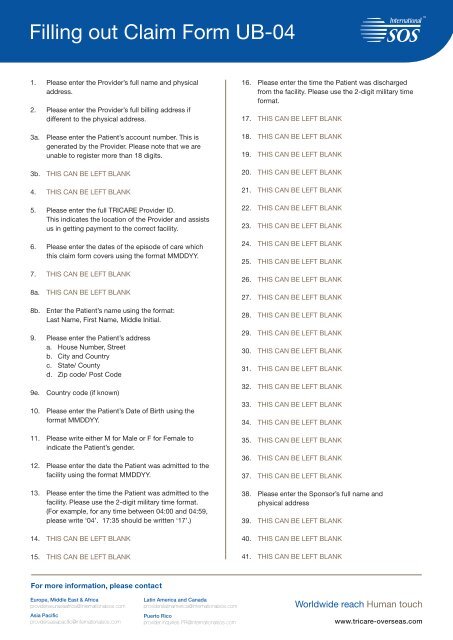
<strong>Filling</strong> <strong>out</strong> <strong>Claim</strong> <strong>Form</strong> <strong>UB</strong>-<strong>04</strong>1. Please enter the Provider’s full name and physicaladdress.2. Please enter the Provider’s full billing address ifdifferent to the physical address.3a. Please enter the Patient’s account number. This isgenerated by the Provider. Please note that we areunable to register more than 18 digits.3b. THIS CAN BE LEFT BLANK4. THIS CAN BE LEFT BLANK5. Please enter the full <strong>TRICARE</strong> Provider ID.This indicates the location of the Provider and assistsus in getting payment to the correct facility.6. Please enter the dates of the episode of care whichthis claim form covers using the format MMDDYY.7. THIS CAN BE LEFT BLANK8a. THIS CAN BE LEFT BLANK8b. Enter the Patient’s name using the format:Last Name, First Name, Middle Initial.9. Please enter the Patient’s addressa. House Number, Streetb. City and Countryc. State/ Countyd. Zip code/ Post Code9e. Country code (if known)10. Please enter the Patient’s Date of Birth using theformat MMDDYY.11. Please write either M for Male or F for Female toindicate the Patient’s gender.12. Please enter the date the Patient was admitted to thefacility using the format MMDDYY.13. Please enter the time the Patient was admitted to thefacility. Please use the 2-digit military time format.(For example, for any time between <strong>04</strong>:00 and <strong>04</strong>:59,please write ‘<strong>04</strong>’. 17:35 should be written ‘17’.)14. THIS CAN BE LEFT BLANK15. THIS CAN BE LEFT BLANK16. Please enter the time the Patient was dischargedfrom the facility. Please use the 2-digit military timeformat.17. THIS CAN BE LEFT BLANK18. THIS CAN BE LEFT BLANK19. THIS CAN BE LEFT BLANK20. THIS CAN BE LEFT BLANK21. THIS CAN BE LEFT BLANK22. THIS CAN BE LEFT BLANK23. THIS CAN BE LEFT BLANK24. THIS CAN BE LEFT BLANK25. THIS CAN BE LEFT BLANK26. THIS CAN BE LEFT BLANK27. THIS CAN BE LEFT BLANK28. THIS CAN BE LEFT BLANK29. THIS CAN BE LEFT BLANK30. THIS CAN BE LEFT BLANK31. THIS CAN BE LEFT BLANK32. THIS CAN BE LEFT BLANK33. THIS CAN BE LEFT BLANK34. THIS CAN BE LEFT BLANK35. THIS CAN BE LEFT BLANK36. THIS CAN BE LEFT BLANK37. THIS CAN BE LEFT BLANK38. Please enter the Sponsor’s full name andphysical address39. THIS CAN BE LEFT BLANK40. THIS CAN BE LEFT BLANK41. THIS CAN BE LEFT BLANKFor more information, please contactEurope, Middle East & Africaproviderseurasiaafrica@internationalsos.comAsia Pacificprovidersasiapacific@internationalsos.comLatin America and Canadaproviderslatinamerica@internationalsos.comPuerto Ricoprovider.inquiries.PR@internationalsos.comWorldwide reach Human touchwww.tricare-overseas.com
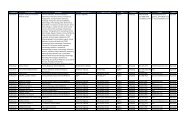
<strong>Filling</strong> <strong>out</strong> <strong>Claim</strong> <strong>Form</strong> <strong>UB</strong>-<strong>04</strong>3a1 2PAT.CNTL b.# MEDREC. 5. FED. TAX NO.36. STATEMENT COVERS PERIODFROMTHROUGH74. TYPEOF BILL8 PATIENT NAME a 9 PATIENT ADDRESS a42. THIS CAN ALL BE LEFT BLANK PROVIDING ANITEMIZED 10. INVOICE IS S<strong>UB</strong>MITTEDADMISSIONb b c d eBIRTHDATE11 SEX12 DATE13 HR 14TYPE43. THIS 31 CAN ALL 32 BE OCCURRENCE LEFT BLANK 33 PROVIDING OCCURRENCE ANOCCURRENCE CODE DATECODE DATEITEMIZEDCODE DATEINVOICE IS S<strong>UB</strong>MITTED44. THIS CAN ALL BE LEFT BLANK PROVIDING ANITEMIZED INVOICE IS S<strong>UB</strong>MITTED45. THIS CAN ALL BE LEFT BLANK PROVIDING ANITEMIZED 42 REV. INVOICE IS S<strong>UB</strong>MITTED46. THIS CAN ALL BE LEFT BLANK PROVIDING ANITEMIZED INVOICE IS S<strong>UB</strong>MITTED47. THIS CAN ALL BE LEFT BLANK PROVIDING ANITEMIZED INVOICE IS S<strong>UB</strong>MITTED48. THIS CAN ALL BE LEFT BLANK PROVIDING ANITEMIZED INVOICE IS S<strong>UB</strong>MITTED49. THIS CAN ALL BE LEFT BLANK PROVIDING ANITEMIZED INVOICE IS S<strong>UB</strong>MITTED50. Please enter the Patient’s primary health insurance ifit is not <strong>TRICARE</strong>.51. Please enter the corresponding health insurancepolicy number.15SRC16DHR17STAT 18 19 20 2134 OCCURRENCECODE DATECONDITION CODES22 23 24 25 26 27 2835 OCCURRENCE SPANCODE FROM THROUGH38 39 VALUE CODESCODE AMOUNTab29 ACDTSTATE36 OCCURRENCE SPANCODE FROM THROUGH40 VALUE CODESCODE AMOUNT303741 VALUE CODESCODE AMOUNTc63. Please enter the Authorization Number supplied byd43. DESCRIPTION 44. HCPCS/RATE/HIPPS CODE45 SERV.48 NON-COVERED46. SER UNITS 47 TOTAL CHARGES49CD.DATECHARGESright corner).1 12 23 34 45 56 67 78 89 910 1011 1Itemized Invoice.12 1213 1314 1415 165. THIS CAN BE LEFT BLANK516 1617 1718 66. THIS CAN BE LEFT BLANK1819 1920 267. THIS CAN BE LEFT BLANK021 2122 268. THIS CAN BE LEFT BLANK2232PAGE OF CREATION DATE TOTA3525350 PAYER NAME 51 HEALTH PLAN ID54 PRIOR LSRELASG.55 EST. AMOUNT DUE56PAYMENTS NPINFOBEN.A I 57 AOTBHER PRCVID58 INSURED’S NAME5960 INSURED’S UNIQUE ID 61 GROUP NAME 62 INSURANCE GROUP NO.P.REL 71. THIS CAN BE LEFT BLANKAB53.CAlways mark ‘Y’ for Yes in this section. This ensuresABName of Primary Health Insurance52. THIS CAN BE LEFT BLANKthe Provider is reimbursed for their services.63 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 65 EMPLOYER NAME54. Please record any payments which have already beenCmade towards this claim, either by the beneficiary oranother health insurance. You may leave this blankif you are submitting the other health insurance’s70Explanation 69 ADMIT of Benefits PATIENT (EOB) with your claim.DXREASON a b cIf the other health DX insurance has not made any66DX 67 A B C D E F G HI J K L M N O P Q74 PRINCIPAL PROCEDURE a OTHER PROCEDUREpayments CODE you DATE must send their CODE EOB. DATEc OTHER PROCEDURE d OTHER PROCEDURE55. THIS CODE CAN BE DATE LEFT BLANK CODEDATE56. THIS CAN BE LEFT BLANK80 REMARKS 81CCa57. THIS CAN BE LEFT BLANKPolicy Numberbe71 PPSCODEOTHER PROCEDURECODEDATEOTHER PROCEDURECODEDATE59. THIS CAN BE LEFT BLANK60. Please enter the Sponsor’s 9 digit SSN number.This can be found on the Patient’s Military ID Card.61. THIS CAN BE LEFT BLANK62. THIS CAN BE LEFT BLANKInternational SOS on the Authorization <strong>Form</strong> (see topNote: No prior authorization is needed for EmergencyRoom Services. Providers must clearly indicate“Emergency Room” or “ER” in Field 63 or on the64. THIS CAN BE LEFT BLANK69. THIS CAN BE LEFT BLANK70. THIS CAN BE LEFT BLANK72. THIS CAN BE LEFT BLANK73. THIS CAN BE LEFT BLANK74. THIS CAN BE LEFT BLANK75. THIS CAN BE LEFT BLANK76. THIS CAN BE LEFT BLANK72ECI77. THIS CAN BE LEFT BLANK7576 ATTENDING NPI78. THIS CAN BE LEFT BLANKLAST77 OPERATING NPI79. THIS CAN BE LEFT BLANKb LAST FIRSTLASTQUALFIRSTQUALFIRST80. Here the Provider’s signature is required.QU78 OTHER NPIThis can be signed by the physician, theALsupplier orsome other authorized person.7368BCABCABC58. Please enter the Sponsor’s name.81. THIS CAN BE LEFT BLANKc 79 OTHER NPIQUALFor more information, please contactd LAST FIRSTCopyright 2007 <strong>Form</strong>s in Word (www.formsinword.com). For individual or single-branch use only.Europe, Middle East & Africaproviderseurasiaafrica@internationalsos.comAsia Pacificprovidersasiapacific@internationalsos.comLatin America and Canadaproviderslatinamerica@internationalsos.comPuerto Ricoprovider.inquiries.PR@internationalsos.comWorldwide reach Human touchwww.tricare-overseas.com