(TYA) Premium Payment Credit Card - TRICARE Overseas
(TYA) Premium Payment Credit Card - TRICARE Overseas
(TYA) Premium Payment Credit Card - TRICARE Overseas
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
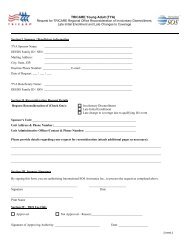
Select One:<strong>TRICARE</strong> Young Adult (<strong>TYA</strong>)<strong>Premium</strong> <strong>Payment</strong> <strong>Credit</strong> <strong>Card</strong> & EFT Authorization FormChange Accounts for Automatic Monthly <strong>Premium</strong> <strong>Payment</strong>sDisenroll from Auto <strong>Payment</strong>sBy signing this form you are authorizing International SOS Assistance, Inc. as applicable, to initiate debit/credit cardor EFT charges (and/or corrections to previous debits/charges) from your account with the financial institutionidentified on this form for payment of <strong>TYA</strong> premiums. A fee of $20 may be applied for insufficient EFT funds.Important note for auto monthly payments: <strong>Payment</strong> of any past due amount is required to set up an automatedmonthly payment account. If you have any unpaid balance over 30 days, it will be charged / debited before newautomatic payments occur. By signing this form you are authorizing International SOS Assistance Inc., asapplicable, to initiate debit/credit charges (and/or corrections to previous debits/charges) from my account with thefinancial institution identified by me on this form for payment of my <strong>TYA</strong> premiums. This authorization will remain ineffect until I provide written notice revoking the authorization to International SOS Assistance Inc. at least 10 daysbefore my account is to be debited/charged.Section I. Beneficiary information<strong>TYA</strong> Enrollee Name: __________________________________________________________<strong>TYA</strong> Enrollee SSN: ___________________________________________________________Mailing address: _____________________________________________________________City, state, ZIP: ______________________________________________________________Daytime phone number: __________________e-mail: _______________________________Section II. Sponsor Information<strong>TYA</strong> Sponsor Name: __________________________________________________________DEERS family ID / Sponsor SSN: ________________________________________________Section III. Select an option below and complete the section.Option #1 - Financial Institution Information for Electronic Fund Transfer (EFT)Type of account: - Checking - SavingsBank routing/transfer number: _____________________________________________Bank account number ___________________________________________________Name of financial institution: _______________________________________________Name(s) on bank account: ________________________________________________Branch address, city, state, ZIP: ____________________________________________Branch telephone number: ________________________________________________Option #2 - <strong>Credit</strong> card paymentsType of account: - Visa - Master<strong>Card</strong><strong>Card</strong>holder name: _______________________________________________________<strong>Card</strong>holder billing address: ________________________________________________City: _____________ State: _______ ZIP: ________ Country: _________<strong>Credit</strong> <strong>Card</strong> Number: _____________________________________________________CVV/CVV2:__________ Expiration date: ________________Section IV. Authorized signatureBy signing this form, you are authorizing International SOS Assistance, Inc to process the request ascompleted above._____________________________________________________________SignatureDate________________________________________________Print NameForm date: April 25, 2011 Page 1 of 2
Form Instructions<strong>TRICARE</strong> Young Adult (<strong>TYA</strong>)<strong>Premium</strong> <strong>Payment</strong> <strong>Credit</strong> <strong>Card</strong> & EFT Authorization FormUse this form if you would like to initiate or discontinue a <strong>TYA</strong> premium payment using your credit/debit cardor and electronic fund transfer from your bank account. Forms will be process within 10 days of receipt.Upon receipt of this form International SOS will process all outstanding charges (if any) due for your <strong>TYA</strong>premium program balance.Section I. – Beneficiary InformationComplete <strong>TYA</strong> Beneficiary account information. Please do not leave anything blank. Please provider aphone number where we can reach you if we need your assistance in processing the information youprovided on this form.Section II. – Sponsor InformationComplete <strong>TYA</strong> Sponsor account information for verification of eligibility to enroll to <strong>TYA</strong> program. Please donot leave anything blank.Section III. - Choose payment optionComplete section for EFT (Electronic Funds Transfer) for checking or savings account debits, or the <strong>Credit</strong><strong>Card</strong> section for Visa or Master<strong>Card</strong> payments.Option #1 – Electronic Fund Transfer (EFT) from your Checking or Savings AccountFor EFT, enclose a blank check mark “VOID.” If you prefer not to attach a voided check, you must provideyour bank account number and routing/transit number (see below). The example provided below is for USbank accounts. If you are using non-US financial institution, please contact your financial institution forassistance in obtaining your required information for this form.Option #2 - <strong>Credit</strong> card payment by Visa and Master<strong>Card</strong><strong>Credit</strong> card payments are only offered for Visa or Master<strong>Card</strong>. For your added security, we ask that youprovide your credit card CVV code. The CVV is a three- or four-digit value printed on the back of your cardlocated near your signature strip.Section IV. Authorized signature (If you are disenrolling from auto monthly payments,select “Disenroll from auto payments” and sign in Section IV)How to Submit Form:Submit a completed copy of page 1 of this form via one of the options belowMail to: International SOS Assistance, IncAttention: <strong>TYA</strong> Accounts ReceivablePO Box 11689Philadelphia, PA 19116Fax to: +1 215-354-2340Form date: April 25, 2011 Page 2 of 2