ABT-DSI08 Congrats Packet - Dance - Wayne State University
ABT-DSI08 Congrats Packet - Dance - Wayne State University
ABT-DSI08 Congrats Packet - Dance - Wayne State University

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
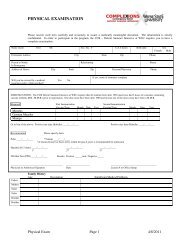
Have you had allergies to any drugs? (please specify)__________________________________________________Are you taking any medication (ex. hormones, inhalers, etc.) on a regular basis? (please list)________________________________________________________________________________________________________________Have you ever had any significant/chronic medical condition(s)? (please specify)____________________________Have you ever had a serious injury or surgery? (please list)___________________________________________________________________________________________________________________________________________Do you have any illness or medical condition that requires regular treatment or alteration of your manner of living?_____________________________________________________________________________________________Is there any other information which could be of assistance?_____________________________________________Have you had any of the following? Select “yes” or “no” to all questions about your personal medical history and brieflycomment on “yes” answers in the space provided (dates, complications, etc.).Yes No Yes NoAsthma____________________________________ Repeated Urinary Tract Infections________________________________Rheumatic Fever_____________________________ High Blood Pressure___________________________________________Congenital Heart Problems/Disease______________ Abnormal Bleeding Tendency____________________________________Hepatitis___________________________________ Epilepsy, Convulsions, Seizures__________________________________Diminished Hearing__________________________ Cancer______________________________________________________Infectious Mononucleosis______________________ Gastric or Duodenal Ulcer_______________________________________Gall Bladder or Liver Disease___________________ Tuberculosis_________________________________________________Diabetes____________________________________ Thyroid Disease______________________________________________Severe Headaches____________________________Comments:__________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________I certify that this information given on this form is true and correct, and I have no abnormality, limitation, or restriction not mentioned on thisdocument. I understand that any false information, willful or negligent misrepresentation or failure to disclose any requested information couldbe sufficient grounds for dismissal from the Summer Intensive. I acknowledge by my signature that I have read and understand these statementsand I hereby authorize the medical professionals of the <strong>ABT</strong> Summer Intensive to treat my child’s medical conditions that appear indicated tothem.__________________________________________Signature_________________________Date SignedThe following physical exam is highly recommended but is not a requirementName_____________________________________ Social Security Number_________________________Height__________in. Weight____________lbs. Temp.____F Pulse________ BP_________Laboratory: Hemoglobin or Hemacrit_____________ Urine SP Gr. ___________ Alb. ________ Sugar _______TB Skin Test: Date_________ Results___________ Name of Test________________Eyes: Are glasses worn? ___Yes ___ No Is color vision defective? ___Yes ___NoEars: Is hearing normal? ___ Yes ___ No Are drums intact? ___Yes ___NoDistant Vision: Right 20/___ Corrected to 20/___ Left 20/___ Corrected to 20/___Near Vision: Right 20/___ Corrected to 20/___ Left 20/___ Corrected to 20/___(Wearers of contact lenses are advised to have a pair of glasses for alternative use.)Normal Abnormal Normal AbnormalSkin__________________________________________ Abdomen__________________________________________Head, Face, Neck________________________________ Endocrine system____________________________________Nose and Sinuses________________________________ Spine______________________________________________Mouth and Throat________________________________ Neurologic_________________________________________Teeth__________________________________________ Hernia_____________________________________________Lungs and Chest_________________________________ Genitalia___________________________________________Heart__________________________________________ Breasts_____________________________________________Vascular_______________________________________ Pelvic, if indicated____________________________________Are muscle strength and function of extremities normal and all digits present? ____Yes ____NoComments:______________________________________________________________________________________________________________________________________________________________________________________________________________28_______________________________________________________________________________________________Signature of M.D./O.D.DatePhysical Exam Page 2 4/22/2008