Gastroesophageal Reflux in Children and Adolescents - National ...
Gastroesophageal Reflux in Children and Adolescents - National ...
Gastroesophageal Reflux in Children and Adolescents - National ...
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Gastroesophageal</strong> <strong>Reflux</strong> (GER) <strong>and</strong><strong>Gastroesophageal</strong> <strong>Reflux</strong> Disease(GERD) <strong>in</strong> <strong>Children</strong> <strong>and</strong> <strong>Adolescents</strong><strong>National</strong> Digestive Diseases Information Clear<strong>in</strong>ghouseWhat is GER?<strong>Gastroesophageal</strong> reflux (GER) occurswhen stomach contents flow back up <strong>in</strong>to theesophagus—the muscular tube that carriesfood <strong>and</strong> liquids from the mouth to thestomach.GER is also called acid reflux or acidregurgitation because the stomach’s digestivejuices conta<strong>in</strong> acid. Sometimes people withGER can taste food or acidic fluid <strong>in</strong> theback of the mouth. <strong>Reflux</strong>ed stomach acidthat touches the l<strong>in</strong><strong>in</strong>g of the esophaguscan cause heartburn. Also called acid<strong>in</strong>digestion, heartburn is an uncomfortable,burn<strong>in</strong>g feel<strong>in</strong>g <strong>in</strong> the midchest, beh<strong>in</strong>dthe breastbone, or <strong>in</strong> the upper part of theabdomen—the area between the chest <strong>and</strong>the hips.Occasional GER commonly occurs <strong>in</strong>children <strong>and</strong> adolescents––ages 2 to 19––<strong>and</strong>does not always mean they have GERD.<strong>Children</strong> <strong>and</strong> adolescents may be able tocontrol GER by• avoid<strong>in</strong>g foods <strong>and</strong> beverages thatcontribute to heartburn, such aschocolate, coffee, pepperm<strong>in</strong>t, greasyor spicy foods, tomato products, <strong>and</strong>alcoholic beverages• avoid<strong>in</strong>g overeat<strong>in</strong>g• quitt<strong>in</strong>g smok<strong>in</strong>g• los<strong>in</strong>g weight if they are overweight• not eat<strong>in</strong>g 2 to 3 hours before sleep• tak<strong>in</strong>g over-the-counter medicationsRead more about over-the-countermedications <strong>in</strong> the section “How is GERDtreated <strong>in</strong> children <strong>and</strong> adolescents?”What is GERD?<strong>Gastroesophageal</strong> reflux disease (GERD) isa more serious, chronic––or long last<strong>in</strong>g––form of GER. GER that occurs morethan twice a week for a few weeks could beGERD, which over time can lead to moreserious health problems. If caregiverssuspect their child or adolescent has GERD,they should take their child or adolescent tosee a pediatrician—a doctor who specializes<strong>in</strong> treat<strong>in</strong>g children <strong>and</strong> adolescents.What causes GERD <strong>in</strong>children <strong>and</strong> adolescents?<strong>Gastroesophageal</strong> reflux disease results whenthe lower esophageal sph<strong>in</strong>cter—the musclethat acts as a valve between the esophagus<strong>and</strong> stomach—becomes weak or relaxeswhen it should not, caus<strong>in</strong>g stomach contentsto rise up <strong>in</strong>to the esophagus.
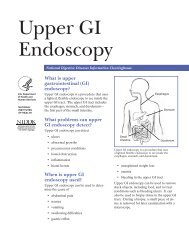
Other factors that can contribute to GERD<strong>in</strong>clude• obesity• certa<strong>in</strong> medications, such as asthmamedications <strong>and</strong> many antihistam<strong>in</strong>es,pa<strong>in</strong> killers, sedatives, <strong>and</strong>antidepressants• smok<strong>in</strong>g, which is more likely withadolescents than younger children, or<strong>in</strong>hal<strong>in</strong>g secondh<strong>and</strong> smoke<strong>Children</strong> who have a history of esophagealsurgery <strong>and</strong> children with severedevelopmental delays are more likely todevelop GERD. Pregnant adolescent girlsmay also develop GERD symptoms. Anychild or adolescent can develop GERD,some for unknown reasons.What is the gastro<strong>in</strong>test<strong>in</strong>al(GI) tract?The GI tract is a series of hollow organsjo<strong>in</strong>ed <strong>in</strong> a long, twist<strong>in</strong>g tube from themouth to the anus. The movement ofmuscles <strong>in</strong> the GI tract, along with therelease of hormones <strong>and</strong> enzymes, startsthe digestion of food. The upper GI tract<strong>in</strong>cludes the mouth, esophagus, stomach,small <strong>in</strong>test<strong>in</strong>e, <strong>and</strong> duodenum, which is thefirst part of the small <strong>in</strong>test<strong>in</strong>e.MouthEsophagusStomachEsophagusLoweresophagealsph<strong>in</strong>cterLoweresophagealsph<strong>in</strong>cterSmall<strong>in</strong>test<strong>in</strong>eAcidStomachSmall<strong>in</strong>test<strong>in</strong>eAnusGERD results when the lower esophageal sph<strong>in</strong>cter—the muscle that acts as a valve between the esophagus <strong>and</strong>stomach—becomes weak or relaxes when it should not, caus<strong>in</strong>g stomach contents to rise up <strong>in</strong>to the esophagus.2 <strong>Gastroesophageal</strong> <strong>Reflux</strong> (GER) <strong>and</strong> <strong>Gastroesophageal</strong> <strong>Reflux</strong> Disease (GERD) <strong>in</strong> <strong>Children</strong> <strong>and</strong> <strong>Adolescents</strong>
A completely accurate test for diagnos<strong>in</strong>gGERD does not exist. However, severaltests can help with diagnosis:Upper GI series. While a pediatricgastroenterologist does not use an upper GIseries to diagnose acid reflux or GERD, thetest can provide a look at the shape of theupper GI tract. An x-ray technician performsthis test at a hospital or an outpatient center,<strong>and</strong> a radiologist—a doctor who specializes<strong>in</strong> medical imag<strong>in</strong>g—<strong>in</strong>terprets the images.This test does not require anesthesia. Ifpossible, a child or an adolescent shouldnot eat or dr<strong>in</strong>k before the procedure, asdirected by the health care staff. Caretakersshould check with the child’s or adolescent’spediatric gastroenterologist about what to doto prepare for an upper GI series.Dur<strong>in</strong>g the procedure, the child or adolescentwill st<strong>and</strong> or sit <strong>in</strong> front of an x-ray mach<strong>in</strong>e<strong>and</strong> dr<strong>in</strong>k barium, a chalky liquid. Bariumcoats the esophagus, stomach, <strong>and</strong> small<strong>in</strong>test<strong>in</strong>e, so the radiologist <strong>and</strong> pediatricgastroenterologist can see these organs’shapes more clearly on x rays. A pediatricgastroenterologist cannot use this test todetect mild irritation; however, this test c<strong>and</strong>etect esophageal strictures—narrow<strong>in</strong>g ofthe esophagus that can result from GERD.<strong>Children</strong> <strong>and</strong> adolescents may experiencebloat<strong>in</strong>g <strong>and</strong> nausea for a short time afterthe test. For several days afterward, bariumliquid <strong>in</strong> the GI tract causes white or lightcoloredstools. A health care provider willprovide specific <strong>in</strong>structions about eat<strong>in</strong>g <strong>and</strong>dr<strong>in</strong>k<strong>in</strong>g after the test.Upper endoscopy. A pediatricgastroenterologist may use anupper endoscopy, also known as anesophagogastroduodenoscopy, if a childor an adolescent cont<strong>in</strong>ues to have GERDsymptoms despite lifestyle changes <strong>and</strong>treatment with medications. An upperendoscopy is a common test used to evaluatethe severity of GERD. This procedure<strong>in</strong>volves us<strong>in</strong>g an endoscope—a small, flexibletube with a light—to see the upper GI tract.A pediatric gastroenterologist performs thistest at a hospital or an outpatient center.<strong>Children</strong> <strong>and</strong> adolescents may receive aliquid anesthetic that is gargled or sprayedon the back of the throat. If sedation isused, a health care provider will place an<strong>in</strong>travenous (IV) needle <strong>in</strong> the child’s oradolescent’s ve<strong>in</strong>.4 <strong>Gastroesophageal</strong> <strong>Reflux</strong> (GER) <strong>and</strong> <strong>Gastroesophageal</strong> <strong>Reflux</strong> Disease (GERD) <strong>in</strong> <strong>Children</strong> <strong>and</strong> <strong>Adolescents</strong>
After the child or adolescent receivessedation, the pediatric gastroenterologistcarefully feeds an endoscope through themouth <strong>and</strong> down the esophagus, then <strong>in</strong>tothe stomach <strong>and</strong> duodenum. A small cameramounted on the endoscope transmits avideo image to a monitor, allow<strong>in</strong>g closeexam<strong>in</strong>ation of the <strong>in</strong>test<strong>in</strong>al l<strong>in</strong><strong>in</strong>g. Thepediatric gastroenterologist uses theendoscope to take a biopsy, a procedure that<strong>in</strong>volves tak<strong>in</strong>g a small piece of esophagealtissue. A pathologist—a doctor whospecializes <strong>in</strong> diagnos<strong>in</strong>g diseases—willexam<strong>in</strong>e the tissue with a microscope <strong>and</strong>determ<strong>in</strong>e the extent of <strong>in</strong>flammation.A pediatric gastroenterologist diagnosesGERD when the test shows <strong>in</strong>jury tothe esophagus <strong>in</strong> children or adolescentswho have had moderate to severe GERDsymptoms.Esophageal pH monitor<strong>in</strong>g. The mostaccurate test to detect acid reflux, esophagealpH monitor<strong>in</strong>g measures the amount ofliquid or acid <strong>in</strong> the esophagus as the childor adolescent goes about normal activities,<strong>in</strong>clud<strong>in</strong>g eat<strong>in</strong>g <strong>and</strong> sleep<strong>in</strong>g. A pediatricgastroenterologist performs this test at ahospital or an outpatient center as a part ofan upper endoscopy. The child or adolescentcan rema<strong>in</strong> awake dur<strong>in</strong>g the test.A pediatric gastroenterologist passes a th<strong>in</strong>tube, called a nasogastric probe, through thechild’s or adolescent’s nose or mouth to thestomach. The pediatric gastroenterologistwill then pull the tube back <strong>in</strong>to theesophagus, where it will be taped to thechild’s or adolescent’s cheek <strong>and</strong> rema<strong>in</strong> <strong>in</strong>place for 24 hours. The end of the tube <strong>in</strong>the esophagus has a small probe to measurewhen <strong>and</strong> how much liquid or acid comes up<strong>in</strong>to the esophagus. The other end of thetube, attached to a monitor outside the body,shows the measurements taken.This test is most useful when comb<strong>in</strong>ed witha carefully kept diary of when, what, <strong>and</strong> howmuch food the child or adolescent eats <strong>and</strong>GERD symptoms that result. The pediatricgastroenterologist can see correlationsbetween symptoms <strong>and</strong> certa<strong>in</strong> foods ortimes of day. The procedure can also helpshow whether reflux triggers respiratorysymptoms.How is GERD treated <strong>in</strong>children <strong>and</strong> adolescents?Treatment for GERD for children <strong>and</strong>adolescents may <strong>in</strong>volve one or more ofthe follow<strong>in</strong>g, depend<strong>in</strong>g on the severity ofsymptoms: lifestyle changes, medications, orsurgery.Lifestyle ChangesSome children <strong>and</strong> adolescents can reduceGERD symptoms by• los<strong>in</strong>g weight, if needed• wear<strong>in</strong>g loose-fitt<strong>in</strong>g clothes aroundthe stomach area, as tight cloth<strong>in</strong>g canconstrict the area <strong>and</strong> <strong>in</strong>crease reflux5 <strong>Gastroesophageal</strong> <strong>Reflux</strong> (GER) <strong>and</strong> <strong>Gastroesophageal</strong> <strong>Reflux</strong> Disease (GERD) <strong>in</strong> <strong>Children</strong> <strong>and</strong> <strong>Adolescents</strong>
• rema<strong>in</strong><strong>in</strong>g upright for 3 hours after meals • rais<strong>in</strong>g the head of the bed 6 to 8 <strong>in</strong>chesby secur<strong>in</strong>g wood blocks under thebedposts––just us<strong>in</strong>g extra pillows willnot help• avoid<strong>in</strong>g smok<strong>in</strong>g <strong>and</strong> be<strong>in</strong>g around others who are smok<strong>in</strong>g MedicationsCaregivers can purchase many GERDmedications without a prescription.However, caregivers should not give children<strong>and</strong> adolescents any medications unlesstold to do so by their child’s or adolescent’spediatrician.Antacids, which <strong>in</strong>clude over-the-countermedications such as Alka-Seltzer, Maalox,Mylanta, Rolaids, <strong>and</strong> Riopan, are a first-l<strong>in</strong>eapproach most health care providers usuallyrecommend to relieve heartburn <strong>and</strong> othermild GERD symptoms. Antacids, however,can have side effects, <strong>in</strong>clud<strong>in</strong>g diarrhea <strong>and</strong>constipation.H2 blockers, such as cimetid<strong>in</strong>e (TagametHB), famotid<strong>in</strong>e (Pepcid AC), nizatid<strong>in</strong>e(Axid AR), <strong>and</strong> ranitid<strong>in</strong>e (Zantac 75),decrease acid production. These medicationsare available <strong>in</strong> both over-the-counter <strong>and</strong>prescription strengths. H2 blockers provideshort-term or on-dem<strong>and</strong> relief <strong>and</strong> areeffective for many children <strong>and</strong> adolescentswith GERD symptoms. They also can helpheal the esophagus, although not as well asproton pump <strong>in</strong>hibitors (PPIs).PPIs <strong>in</strong>clude omeprazole (Prilosec, Zegerid),lansoprazole (Prevacid), pantoprazole(Protonix), rabeprazole (Aciphex), <strong>and</strong>esomeprazole (Nexium), which areavailable by prescription. Omeprazole <strong>and</strong>lansoprazole also come <strong>in</strong> over-the-counterstrengths. PPIs are more effective thanH2 blockers <strong>and</strong> can relieve symptoms <strong>and</strong>heal the esophageal l<strong>in</strong><strong>in</strong>g <strong>in</strong> most children<strong>and</strong> adolescents with GERD. Health careproviders most commonly prescribe PPIs forlong-term management of GERD. However,studies show they are more likely to causehip, wrist, <strong>and</strong> sp<strong>in</strong>al fractures when takenlong term or <strong>in</strong> high doses. <strong>Children</strong> <strong>and</strong>adolescents should take these medications onan empty stomach <strong>in</strong> order for stomach acidto activate them.Prok<strong>in</strong>etics, which <strong>in</strong>clude bethanechol(Urechol<strong>in</strong>e) <strong>and</strong> metoclopramide(Reglan), help make the stomach emptyfaster. However, both bethanechol <strong>and</strong>metoclopramide have side effects that oftenlimit their use, <strong>in</strong>clud<strong>in</strong>g nausea, diarrhea,tiredness, depression, anxiety, <strong>and</strong> problemswith physical movement. Prok<strong>in</strong>etics can<strong>in</strong>teract with other medications, so caregiversshould tell the health care provider about allmedications the child or adolescent takes.6 <strong>Gastroesophageal</strong> <strong>Reflux</strong> (GER) <strong>and</strong> <strong>Gastroesophageal</strong> <strong>Reflux</strong> Disease (GERD) <strong>in</strong> <strong>Children</strong> <strong>and</strong> <strong>Adolescents</strong>
Eat<strong>in</strong>g, Diet, <strong>and</strong> Nutrition<strong>Children</strong> <strong>and</strong> adolescents with GERD canoften reduce reflux by avoid<strong>in</strong>g foods <strong>and</strong>dr<strong>in</strong>ks that worsen symptoms. Other dietarychanges that can help reduce symptoms<strong>in</strong>clude decreas<strong>in</strong>g fat <strong>in</strong>take <strong>and</strong> eat<strong>in</strong>gsmall, frequent meals <strong>in</strong>stead of three largemeals. <strong>Children</strong> <strong>and</strong> adolescents who areoverweight can talk with a pediatricianabout dietary changes that can help themlose weight, which may decrease GERDsymptoms.Po<strong>in</strong>ts to Remember• <strong>Gastroesophageal</strong> reflux (GER)occurs when stomach contents flowback up <strong>in</strong>to the esophagus.• GER is also called acid reflux or acidregurgitation because the stomach’sdigestive juices conta<strong>in</strong> acid.• <strong>Gastroesophageal</strong> reflux disease(GERD) is a more serious, chronicform of GER.• GERD results when the loweresophageal sph<strong>in</strong>cter becomes weakor relaxes when it should not, caus<strong>in</strong>gstomach contents to rise up <strong>in</strong>to theesophagus.• In older children <strong>and</strong> adolescents, thema<strong>in</strong> symptom of GERD is frequentheartburn. Most children with GERDwho are younger than 12 do not haveheartburn.• Other common GERD symptoms<strong>in</strong>clude a chronic cough, asthmaor recurrent pneumonia, nausea,difficulty swallow<strong>in</strong>g or pa<strong>in</strong>fulswallow<strong>in</strong>g, <strong>and</strong> pa<strong>in</strong> <strong>in</strong> the chest.• A pediatrician may refer children <strong>and</strong>adolescents with suspected GERDto a pediatric gastroenterologist fordiagnosis <strong>and</strong> treatment.• Treatment for GERD for children <strong>and</strong>adolescents may <strong>in</strong>volve one or moreof the follow<strong>in</strong>g, depend<strong>in</strong>g on theseverity of symptoms: lifestyle changes,medications, or surgery.• A pediatrician should monitorchildren <strong>and</strong> adolescents withGERD to prevent or treat long-termcomplications.9 <strong>Gastroesophageal</strong> <strong>Reflux</strong> (GER) <strong>and</strong> <strong>Gastroesophageal</strong> <strong>Reflux</strong> Disease (GERD) <strong>in</strong> <strong>Children</strong> <strong>and</strong> <strong>Adolescents</strong>
Hope through ResearchThe Division of Digestive Diseases <strong>and</strong>Nutrition at the <strong>National</strong> Institute ofDiabetes <strong>and</strong> Digestive <strong>and</strong> Kidney Diseases(NIDDK) supports basic <strong>and</strong> cl<strong>in</strong>icalresearch <strong>in</strong>to GI diseases, <strong>in</strong>clud<strong>in</strong>g GER<strong>and</strong> GERD.Cl<strong>in</strong>ical trials are research studies <strong>in</strong>volv<strong>in</strong>gpeople. Cl<strong>in</strong>ical trials look at safe <strong>and</strong>effective new ways to prevent, detect, ortreat disease. Researchers also use cl<strong>in</strong>icaltrials to look at other aspects of care, suchas improv<strong>in</strong>g the quality of life for peoplewith chronic illnesses. To learn more aboutcl<strong>in</strong>ical trials, why they matter, <strong>and</strong> how toparticipate, visit the NIH Cl<strong>in</strong>ical ResearchTrials <strong>and</strong> You website at www.nih.gov/health/cl<strong>in</strong>icaltrials. For <strong>in</strong>formation about currentstudies, visit www.Cl<strong>in</strong>icalTrials.gov.For More InformationNorth American Society for PediatricGastroenterology, Hepatology <strong>and</strong> Nutrition(NASPGHAN)P.O. Box 6Flourtown, PA 19031Phone: 215–233–0808Fax: 215–233–3918Email: naspghan@naspghan.orgInternet: www.naspghan.orgPediatric/Adolescent <strong>Gastroesophageal</strong><strong>Reflux</strong> AssociationP.O. Box 7728Silver Spr<strong>in</strong>g, MD 20907Phone: 301–601–9541Email: gergroup@aol.comInternet: www.reflux.org10 <strong>Gastroesophageal</strong> <strong>Reflux</strong> (GER) <strong>and</strong> <strong>Gastroesophageal</strong> <strong>Reflux</strong> Disease (GERD) <strong>in</strong> <strong>Children</strong> <strong>and</strong> <strong>Adolescents</strong>
You may also f<strong>in</strong>d additional <strong>in</strong>formation about thistopic by visit<strong>in</strong>g Medl<strong>in</strong>ePlus at www.medl<strong>in</strong>eplus.gov.This publication may conta<strong>in</strong> <strong>in</strong>formation aboutmedications <strong>and</strong>, when taken as prescribed,the conditions they treat. When prepared, thispublication <strong>in</strong>cluded the most current <strong>in</strong>formationavailable. For updates or for questions aboutany medications, contact the U.S. Food <strong>and</strong> DrugAdm<strong>in</strong>istration toll-free at 1–888–INFO–FDA(1–888–463–6332) or visit www.fda.gov. Consult yourhealth care provider for more <strong>in</strong>formation.The U.S. Government does not endorse or favor anyspecific commercial product or company. Trade,proprietary, or company names appear<strong>in</strong>g <strong>in</strong> thisdocument are used only because they are considerednecessary <strong>in</strong> the context of the <strong>in</strong>formation provided.If a product is not mentioned, the omission does notmean or imply that the product is unsatisfactory.<strong>National</strong> Digestive DiseasesInformation Clear<strong>in</strong>ghouse2 Information WayBethesda, MD 20892–3570Phone: 1–800–891–5389TTY: 1–866–569–1162Fax: 703–738–4929Email: nddic@<strong>in</strong>fo.niddk.nih.govInternet: www.digestive.niddk.nih.govThe <strong>National</strong> Digestive Diseases InformationClear<strong>in</strong>ghouse (NDDIC) is a service of the<strong>National</strong> Institute of Diabetes <strong>and</strong> Digestive<strong>and</strong> Kidney Diseases (NIDDK). TheNIDDK is part of the <strong>National</strong> Institutes ofHealth of the U.S. Department of Health<strong>and</strong> Human Services. Established <strong>in</strong> 1980,the Clear<strong>in</strong>ghouse provides <strong>in</strong>formationabout digestive diseases to people withdigestive disorders <strong>and</strong> to their families,health care professionals, <strong>and</strong> the public.The NDDIC answers <strong>in</strong>quiries, develops <strong>and</strong>distributes publications, <strong>and</strong> works closelywith professional <strong>and</strong> patient organizations<strong>and</strong> Government agencies to coord<strong>in</strong>ateresources about digestive diseases.This publication is not copyrighted. The Clear<strong>in</strong>ghouseencourages users of this publication to duplicate <strong>and</strong>distribute as many copies as desired.This publication is available atwww.digestive.niddk.nih.gov.NIH Publication No. 13–5418September 2013The NIDDK pr<strong>in</strong>ts on recycled paper with bio-based <strong>in</strong>k.