V2 MRI Pt screening form KT 9-9-09 - McLean Hospital
V2 MRI Pt screening form KT 9-9-09 - McLean Hospital
V2 MRI Pt screening form KT 9-9-09 - McLean Hospital

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
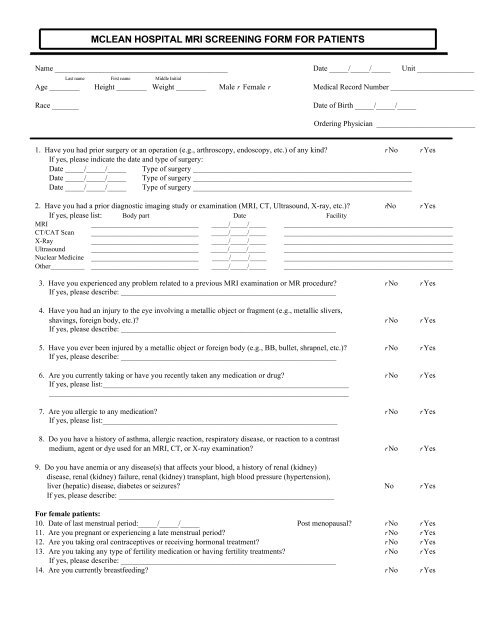
MCLEAN HOSPITAL <strong>MRI</strong> SCREENING FORM FOR PATIENTSName ______________________________________________ Date _____/_____/_____ Unit _______________Last name First name Middle InitialAge ________ Height ________ Weight ________ Male r Female r Medical Record Number ______________________Race _______Date of Birth _____/_____/_____Ordering Physician __________________________1. Have you had prior surgery or an operation (e.g., arthroscopy, endoscopy, etc.) of any kind? r No r YesIf yes, please indicate the date and type of surgery:Date _____/_____/_____ Type of surgery _________________________________________________________Date _____/_____/_____ Type of surgery _________________________________________________________Date _____/_____/_____ Type of surgery _________________________________________________________2. Have you had a prior diagnostic imaging study or examination (<strong>MRI</strong>, CT, Ultrasound, X-ray, etc.)? rNo r YesIf yes, please list: Body part Date Facility<strong>MRI</strong> ____________________________ _____/_____/_____ ____________________________________________CT/CAT Scan ____________________________ _____/_____/_____ ____________________________________________X-Ray ____________________________ _____/_____/_____ ____________________________________________Ultrasound ____________________________ _____/_____/_____ ____________________________________________Nuclear Medicine ____________________________ _____/_____/_____ ____________________________________________Other__________ ____________________________ _____/_____/_____ ____________________________________________3. Have you experienced any problem related to a previous <strong>MRI</strong> examination or MR procedure? r No r YesIf yes, please describe: ________________________________________________________4. Have you had an injury to the eye involving a metallic object or fragment (e.g., metallic slivers,shavings, foreign body, etc.)? r No r YesIf yes, please describe: ________________________________________________________5. Have you ever been injured by a metallic object or foreign body (e.g., BB, bullet, shrapnel, etc.)? r No r YesIf yes, please describe: ________________________________________________________6. Are you currently taking or have you recently taken any medication or drug? r No r YesIf yes, please list:______________________________________________________________________________________________________________________________________________7. Are you allergic to any medication? r No r YesIf yes, please list:_____________________________________________________________8. Do you have a history of asthma, allergic reaction, respiratory disease, or reaction to a contrastmedium, agent or dye used for an <strong>MRI</strong>, CT, or X-ray examination? r No r Yes9. Do you have anemia or any disease(s) that affects your blood, a history of renal (kidney)disease, renal (kidney) failure, renal (kidney) transplant, high blood pressure (hypertension),liver (hepatic) disease, diabetes or seizures? No r YesIf yes, please describe: ________________________________________________________For female patients:10. Date of last menstrual period:_____/_____/_____ Post menopausal? r No r Yes11. Are you pregnant or experiencing a late menstrual period? r No r Yes12. Are you taking oral contraceptives or receiving hormonal treatment? r No r Yes13. Are you taking any type of fertility medication or having fertility treatments? r No r YesIf yes, please describe: ________________________________________________________14. Are you currently breastfeeding? r No r Yes
WARNING: Certain implants, devices, or objects may be hazardous to you and/or may interfere with theMR procedure (i.e., <strong>MRI</strong>, MR angiography, functional <strong>MRI</strong>, MR spectroscopy). Do not enter the MR system roomor MR environment if you have any question or concern regarding an implant, device, or object. Consult the <strong>MRI</strong>Technologist or Radiologist BEFORE entering the MR system room. The MR system magnet is ALWAYS on.Please indicate if you have any of the following:r Yes r No Aneurysm clip(s)r Yes r No Cardiac pacemakerr Yes r No Implanted cardioverter defibrillator (ICD)r Yes r No Electronic implant or devicer Yes r No Magnetically-activated implant or devicer Yes r No Neurostimulation systemr Yes r No Spinal cord stimulatorr Yes r No Internal electrodes or wiresr Yes r No Bone growth/bone fusion stimulatorr Yes r No Cochlear, otologic, or other ear implantr Yes r No Insulin or other infusion pumpr Yes r No Implanted drug infusion devicer Yes r No Any type of prosthesis (eye, penile, etc.)r Yes r No Heart valve prosthesisr Yes r No Eyelid spring or wirer Yes r No Artificial or prosthetic limbr Yes r No Metallic stent, filter, or coilr Yes r No Shunt (spinal or intraventricular)r Yes r No Vascular access port and/or catheterr Yes r No Radiation seeds or implantsr Yes r No Swan-Ganz or thermodilution catheterr Yes r No Medication patch (Nicotine, Nitroglycerine,etc.)r Yes r No Any metallic fragment or foreign bodyr Yes r No Wire mesh implantr Yes r No Tissue expander (e.g., breast)r Yes r No Surgical staples, clips, or metallic suturesr Yes r No Joint replacement (hip, knee, etc.)r Yes r No Bone/joint pin, screw, nail, wire, plate, etc.r Yes r No IUD, diaphragm, or pessaryr Yes r No Dentures or partial platesr Yes r No Tattoo or permanent makeupr Yes r No Body piercing jewelryr Yes r No Hearing aid(Remove before entering MR system room)r Yes r No Other implant _______________________r Yes r No Breathing problem or motion disorderr Yes r No ClaustrophobiaPlease mark on the figure(s) belowthe location of any implant or metalinside of or on your body.IMPORTANT INSTRUCTIONSBefore entering the MR environment or MR systemroom, you must remove all metallic objects includinghearing aids, dentures, partial plates, keys, beeper, cellphone, eyeglasses, hair pins, barrettes, jewelry, bodypiercing jewelry, watch, safety pins, paperclips, moneyclip, credit cards, bank cards, magnetic strip cards,coins, pens, pocket knife, nail clipper, tools, clothingwith metal fasteners, & clothing with metallic threads.Please consult the <strong>MRI</strong> Technologist or your physician ifyou have any question or concern BEFORE you enter theMR system room.NOTE: You may be advised or required to wear earplugs or other hearing protection duringthe MR procedure to prevent possible problems or hazards related to acoustic noise.I attest that the above in<strong>form</strong>ation is correct to the best of my knowledge. I read and understand the contents of this <strong>form</strong> and had theopportunity to ask questions regarding the in<strong>form</strong>ation on this <strong>form</strong> and regarding the MR procedure that I am about to undergo.Signature of Person Completing Form: _______________________________________SignatureDate _____/_____/_____Form Completed By: r Patient r Relative r Physician r Nurse ____________________________________ ____________________________Print nameRelationship to patientPhysician reviewing / confirming <strong>screening</strong> in<strong>form</strong>ation: ______________________________ _______________________________________Printed NameSignaturer Attending Physicianr Other ________________________________________________