Glens Falls Hospital Patient Financial Assistance Program
Glens Falls Hospital Patient Financial Assistance Program
Glens Falls Hospital Patient Financial Assistance Program

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
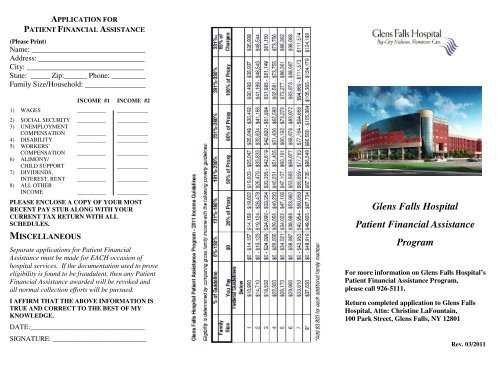
APPLICATION FORPATIENT FINANCIAL ASSISTANCE(Please Print)Name: ______________________________Address: ____________________________City: _______________________________State: _____ Zip:______ Phone: _________Family Size/Household: ________________INCOME #1 INCOME #21) WAGES __________ ___________2) SOCIAL SECURITY __________ ___________3) UNEMPLOYMENTCOMPENSATION __________ ___________4) DISABILITY __________ ___________5) WORKERS’COMPENSATION __________ ___________6) ALIMONY/CHILD SUPPORT __________ ___________7) DIVIDENDS,INTEREST, RENT __________ ___________8) ALL OTHERINCOME __________ ___________PLEASE ENCLOSE A COPY OF YOUR MOSTRECENT PAY STUB ALONG WITH YOURCURRENT TAX RETURN WITH ALLSCHEDULES.MISCELLANEOUSSeparate applications for <strong>Patient</strong> <strong>Financial</strong><strong>Assistance</strong> must be made for EACH occasion ofhospital services. If the documentation used to proveeligibility is found to be fraudulent, then any <strong>Patient</strong><strong>Financial</strong> <strong>Assistance</strong> awarded will be revoked andall normal collection efforts will be pursued.I AFFIRM THAT THE ABOVE INFORMATION ISTRUE AND CORRECT TO THE BEST OF MYKNOWLEDGE.DATE:_________________________________SIGNATURE: ___________________________<strong>Glens</strong> <strong>Falls</strong> <strong>Hospital</strong><strong>Patient</strong> <strong>Financial</strong> <strong>Assistance</strong><strong>Program</strong>For more information on <strong>Glens</strong> <strong>Falls</strong> <strong>Hospital</strong>’s<strong>Patient</strong> <strong>Financial</strong> <strong>Assistance</strong> <strong>Program</strong>,please call 926-5111.Return completed application to <strong>Glens</strong> <strong>Falls</strong><strong>Hospital</strong>, Attn: Christine LaFountain,100 Park Street, <strong>Glens</strong> <strong>Falls</strong>, NY 12801Rev. 03/2011
GENERAL INFORMATION<strong>Glens</strong> <strong>Falls</strong> <strong>Hospital</strong> will make <strong>Patient</strong> <strong>Financial</strong><strong>Assistance</strong> available to qualified patients. <strong>Glens</strong><strong>Falls</strong> <strong>Hospital</strong> recognizes that there are times whenpatients in need of care will be unable to pay forthe needed health care services provided. It is thepolicy of <strong>Glens</strong> <strong>Falls</strong> <strong>Hospital</strong> to provide andpromote a consistent methodology for extendingfinancial assistance to qualified patients in order tofacilitate payment for hospital services.ELIGIBILITYA patient’s eligibility for <strong>Patient</strong> <strong>Financial</strong><strong>Assistance</strong> will be based upon the size of theapplicant’s family and is limited to those familieswhose income is less than or equal to 3.3 times(330%) of the current poverty level incomeguidelines as determined by the CommunityServices Administration. In addition, applicantsmust demonstrate that they are unable to pay forthe services rendered. <strong>Glens</strong> <strong>Falls</strong> <strong>Hospital</strong> willthen use the attached guidelines to determine theappropriate level of financial assistance.DESCRIPTION OF SERVICE AREA<strong>Glens</strong> <strong>Falls</strong> <strong>Hospital</strong> will extend financialassistance to all eligible patients including patientswhose residency falls outside our primary servicearea within New York State as well as patientswhose residency is outside New York State.INABILITY TO PAYEligible patients are requested to provide incomeverification every six months. Once qualified, the<strong>Hospital</strong> will use income information to determinelevels of financial assistance for each six-monthperiod. <strong>Patient</strong>s must demonstrate that they arenot eligible for Medicaid. The <strong>Hospital</strong> willprovide assistance in obtaining Medicaid coverage,if required documents are provided to the<strong>Hospital</strong> in a timely manner.COVERED SERVICES<strong>Patient</strong> <strong>Financial</strong> <strong>Assistance</strong> funds will be utilizedfor all services rendered by <strong>Glens</strong> <strong>Falls</strong> <strong>Hospital</strong>,including Adirondack Medical Services, with theexception of cosmetic procedures and hearingaids. Charges from private Physicians who provideservices at the hospital are not covered. (example:Radiologist/Pathologists/Anesthesiologists)APPLICATION PROCESS<strong>Patient</strong>s seeking access to the <strong>Patient</strong> <strong>Financial</strong><strong>Assistance</strong> <strong>Program</strong> will complete an applicationunder the guidance of a <strong>Patient</strong> <strong>Financial</strong> Servicesrepresentative. During this process, thedetermination of eligibility will be made contingentupon the patient producing income verification(tax returns) and a Medicaid denial, if applicable.The <strong>Patient</strong> <strong>Financial</strong> Services Department willrender a decision within ten (10) business daysof receipt of all necessary patient documentation.Any application will be considered withdrawnif all requested documentation is notpresented within twenty (20) days of therequest. If the documentation used to proveeligibility is found to be fraudulent, any <strong>Patient</strong><strong>Assistance</strong> awarded will be revoked and allnormal collection efforts will be pursued.ACCEPTABLE INCOMEVERIFICATION1. Most recent income tax return (FederalTax Return will be used to determinefamily size/adjusted gross income.)2. Self-Employed individual’s incomecalculation will be based on adjusted grossincome reported on IRS tax form – 1040.3. Other income documentation (example:SSI, SSD or pension statement)<strong>Patient</strong> <strong>Financial</strong> <strong>Assistance</strong> will only be appliedafter all insurance coverage has been exhaustedor for uninsured self-pay patients. A <strong>Patient</strong><strong>Financial</strong> <strong>Assistance</strong> application must be madewithin 90 days after receipt of the initial billfrom <strong>Glens</strong> <strong>Falls</strong> <strong>Hospital</strong>.