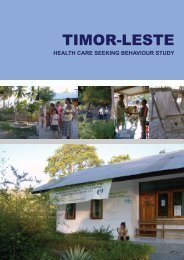
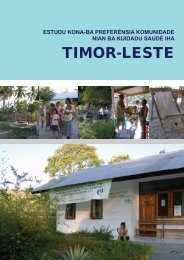
IDP camp at SAMES, February 2007 Photo: T<strong>in</strong>uko’o J. VasCommunity members <strong>in</strong> some IDP camps had enhanced access through mobile services <strong>and</strong> <strong>in</strong>-camp cl<strong>in</strong>ics, aswell as be<strong>in</strong>g able to use non-government cl<strong>in</strong>ics such as Bairo Pite, private cl<strong>in</strong>ics <strong>and</strong> pharmacies when thesecurity situation allowed. High levels <strong>of</strong> utilisation were observed <strong>in</strong> these services at early stages <strong>of</strong> the emergency.The graph below <strong>in</strong>dicates diagnoses for three common conditions: malaria <strong>and</strong> diarrhea (graphed together) <strong>and</strong>upper respiratory tract <strong>in</strong>fections. No major outbreaks <strong>of</strong> communicable diseases were identified, although a number<strong>of</strong> possible outbreaks were identified <strong>and</strong> <strong>in</strong>vestigated. As described later there was some confusion regard<strong>in</strong>gsurveillance data. Where cases <strong>of</strong> diarrhoea <strong>and</strong> poor water supplies were identified this was corrected by chlor<strong>in</strong>ation.Cases detected450040003500300025002000150010005000URTI Disease Trend 29 May to 24 Dec 200622 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52Report<strong>in</strong>g weekFigure 9: URTI Disease Trend 29 May - 24 December 2006.Source <strong>Timor</strong>-<strong>Leste</strong> M<strong>in</strong>istry <strong>of</strong> <strong>Health</strong>Cases reported500450400350300250200150100500Disease trends 29 May to 24 Dec 06DiarrhoeaMalaria22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51Report<strong>in</strong>g weekFigure 10: Disease Trends 29 May - 24 December 2006.Source <strong>Timor</strong>-<strong>Leste</strong> M<strong>in</strong>istry <strong>of</strong> <strong>Health</strong>However, the effort that went <strong>in</strong>to provid<strong>in</strong>g IDPs <strong>and</strong> the general community <strong>in</strong> Dili with access to services was notreplicated <strong>in</strong> the Districts where services were placed under considerable additional stra<strong>in</strong> as they sought to copewith larger numbers <strong>of</strong> population flee<strong>in</strong>g from Dili <strong>in</strong> search <strong>of</strong> safety <strong>and</strong> family support.Until now, we never get money or ‘rent’ for this… to solve some problems … you know the IDPs come here<strong>and</strong> maybe someth<strong>in</strong>g happens <strong>and</strong> we can’t help… we don’t have the money for that – District Adm<strong>in</strong>istrator22 TIMOR-LESTE HEALTH SECTOR RESILIENCE AND PERFORMANCE IN A TIME OF INSTABILITY
Some districts, such as Lautem, went to the trouble <strong>of</strong> arrang<strong>in</strong>g for the District Adm<strong>in</strong>istrator <strong>and</strong> others to visit theIDP camps <strong>in</strong> Dili <strong>and</strong> <strong>in</strong>vit<strong>in</strong>g people with family ties <strong>in</strong> the district to come home. Transport <strong>and</strong> support wereprovided. The District established two “Commissions” to provide emergency support, to coord<strong>in</strong>ate all the availablecommunity resources, <strong>and</strong> to reassure people <strong>of</strong> their commitment to impartiality <strong>and</strong> non-discrim<strong>in</strong>ation.Most district services coped with the additional load, at times us<strong>in</strong>g <strong>in</strong>novative strategies to keep services function<strong>in</strong>g,such as shar<strong>in</strong>g drugs between cl<strong>in</strong>ics. There were stra<strong>in</strong>s, however, <strong>of</strong>ten relat<strong>in</strong>g to lack <strong>of</strong> fuel supplies forcommunity-based activities:Dur<strong>in</strong>g the crisis our health services ran as normal, we gave treatment as usual to <strong>in</strong>patient <strong>and</strong> outpatientservices; everyday we still attended the patients. The drugs was still sufficient, … Also we ma<strong>in</strong>ta<strong>in</strong>ed ourimmunization program for several sucos but some sucos we didn’t do because the situation did not allow. Butthe services at <strong>Health</strong> Posts <strong>and</strong> <strong>Health</strong> centers still functioned as <strong>in</strong> normal time.- Senior health manager, Ermera districtPregnant women were identified as a group requir<strong>in</strong>g particular attention. UN agencies, work<strong>in</strong>g with government<strong>and</strong> NGOs promoted the establishment <strong>of</strong> a Maternity Wait<strong>in</strong>g Camp (MWC) with<strong>in</strong> the national hospital. Althoughthis was an <strong>in</strong>novative idea, seek<strong>in</strong>g to improve access <strong>and</strong> safety, it also had some unanticipated negative effects(Box 3).Although rout<strong>in</strong>e services cont<strong>in</strong>ued to be provided, immunisation activity through the Dili district CHCs decl<strong>in</strong>eddramatically <strong>in</strong> May <strong>and</strong> for the rest <strong>of</strong> the year, <strong>in</strong> respect <strong>of</strong> DPT-3 immunisation (Figure 11). For measles, activity<strong>in</strong>creased <strong>in</strong> the third quarter <strong>and</strong> then spiked, reflect<strong>in</strong>g major measles immunisation campaign activities <strong>in</strong> November(Figure 12).Figure 11: DPT-3 immunisation <strong>in</strong> Dili CHCs Centro, Becora <strong>and</strong>Comoro. Source <strong>Timor</strong>-<strong>Leste</strong> M<strong>in</strong>istry <strong>of</strong> <strong>Health</strong>Figure 12: Measels immunisation <strong>in</strong> Dili CHCs Centro, Becora <strong>and</strong>Comoro. Source <strong>Timor</strong>-<strong>Leste</strong> M<strong>in</strong>istry <strong>of</strong> <strong>Health</strong>Demonstrat<strong>in</strong>g that the government is <strong>in</strong> charge: leadership, coord<strong>in</strong>ation <strong>and</strong>flexibilityIn times <strong>of</strong> crisis, effective government leadership can help ensure that emergency <strong>and</strong> humanitarian issues areaddressed with<strong>in</strong> the context <strong>of</strong> exist<strong>in</strong>g policies <strong>and</strong> strategies. It may also help ensure that national capacity isdeveloped dur<strong>in</strong>g the emergency <strong>and</strong> that lessons can be learned <strong>and</strong> fed back <strong>in</strong>to the system. Failure to demonstrateleadership may result <strong>in</strong> the <strong>in</strong>ternational community (United Nations <strong>and</strong> <strong>in</strong>ternational NGOs <strong>and</strong> others) assum<strong>in</strong>gresponsibility for address<strong>in</strong>g basic needs <strong>and</strong> provid<strong>in</strong>g services. The Government <strong>and</strong> public sector may be sidel<strong>in</strong>ed<strong>and</strong> unable to control how the <strong>in</strong>ternational community engages locally. One effect <strong>of</strong> this may be that additionalresources bypass <strong>and</strong> even underm<strong>in</strong>e national <strong>and</strong> local systems. Where fragile <strong>and</strong> weak states lack the resources<strong>and</strong> the capacity to respond to essential needs, the <strong>in</strong>tervention <strong>of</strong> the <strong>in</strong>ternational community is justifiable. Butwhere national government is able to demonstrate its sovereignty <strong>and</strong> ability to respond, the <strong>in</strong>ternational communityTIMOR-LESTE HEALTH SECTOR RESILIENCE AND PERFORMANCE IN A TIME OF INSTABILITY 23