SOMATOM Sessions - Siemens Healthcare
SOMATOM Sessions - Siemens Healthcare
SOMATOM Sessions - Siemens Healthcare

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Clinical Results Cardio-Vascular<br />
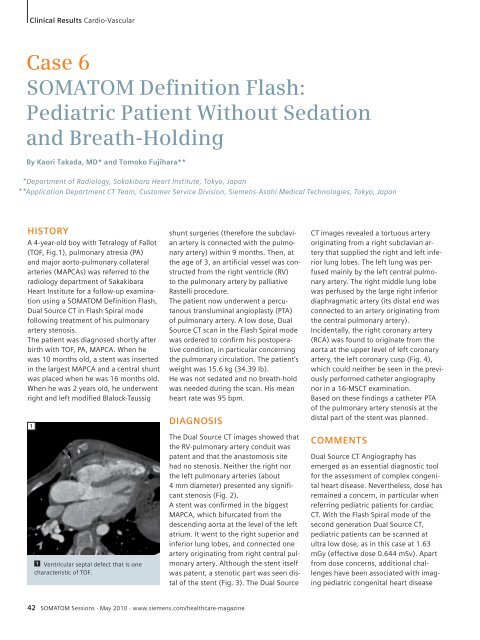
Case 6<br />
<strong>SOMATOM</strong> Defi nition Flash:<br />
Pediatric Patient Without Sedation<br />
and Breath-Holding<br />
By Kaori Takada, MD* and Tomoko Fujihara**<br />
* Department of Radiology, Sakakibara Heart Institute, Tokyo, Japan<br />
**<br />
Application Department CT Team, Customer Service Division, <strong>Siemens</strong>-Asahi Medical Technologies, Tokyo, Japan<br />
HISTORY<br />
A 4-year-old boy with Tetralogy of Fallot<br />
(TOF, Fig.1), pulmonary atresia (PA)<br />
and major aorto-pulmonary collateral<br />
arteries (MAPCAs) was referred to the<br />
radiology department of Sakakibara<br />
Heart Institute for a follow-up examination<br />
using a <strong>SOMATOM</strong> Definition Flash,<br />
Dual Source CT in Flash Spiral mode<br />
following treatment of his pulmonary<br />
artery stenosis.<br />
The patient was diagnosed shortly after<br />
birth with TOF, PA, MAPCA. When he<br />
was 10 months old, a stent was inserted<br />
in the largest MAPCA and a central shunt<br />
was placed when he was 16 months old.<br />
When he was 2 years old, he underwent<br />
right and left modified Blalock-Taussig<br />
1<br />
1 Ventricular septal defect that is one<br />
characteristic of TOF.<br />
shunt surgeries (therefore the subclavian<br />
artery is connected with the pulmonary<br />
artery) within 9 months. Then, at<br />
the age of 3, an artificial vessel was constructed<br />
from the right ventricle (RV)<br />
to the pulmonary artery by palliative<br />
Rastelli procedure.<br />
The patient now underwent a percutanous<br />
transluminal angioplasty (PTA)<br />
of pulmonary artery. A low dose, Dual<br />
Source CT scan in the Flash Spiral mode<br />
was ordered to confirm his postoperative<br />
condition, in particular concerning<br />
the pulmonary circulation. The patient’s<br />
weight was 15.6 kg (34.39 lb).<br />
He was not sedated and no breath-hold<br />
was needed during the scan. His mean<br />
heart rate was 95 bpm.<br />
DIAGNOSIS<br />
The Dual Source CT images showed that<br />
the RV-pulmonary artery conduit was<br />
patent and that the anastomosis site<br />
had no stenosis. Neither the right nor<br />
the left pulmonary arteries (about<br />
4 mm diameter) presented any significant<br />
stenosis (Fig. 2).<br />
A stent was confirmed in the biggest<br />
MAPCA, which bifurcated from the<br />
descending aorta at the level of the left<br />
atrium. It went to the right superior and<br />
inferior lung lobes, and connected one<br />
artery originating from right central pulmonary<br />
artery. Although the stent itself<br />
was patent, a stenotic part was seen distal<br />
of the stent (Fig. 3). The Dual Source<br />
42 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
CT images revealed a tortuous artery<br />
originating from a right subclavian artery<br />
that supplied the right and left inferior<br />
lung lobes. The left lung was perfused<br />
mainly by the left central pulmonary<br />
artery. The right middle lung lobe<br />
was perfused by the large right inferior<br />
diaphragmatic artery (its distal end was<br />
connected to an artery originating from<br />
the central pulmonary artery).<br />
Incidentally, the right coronary artery<br />
(RCA) was found to originate from the<br />
aorta at the upper level of left coronary<br />
artery, the left coronary cusp (Fig. 4),<br />
which could neither be seen in the previously<br />
performed catheter angiography<br />
nor in a 16-MSCT examination.<br />
Based on these findings a catheter PTA<br />
of the pulmonary artery stenosis at the<br />
distal part of the stent was planned.<br />
COMMENTS<br />
Dual Source CT Angiography has<br />
emerged as an essential diagnostic tool<br />
for the assessment of complex congenital<br />
heart disease. Nevertheless, dose has<br />
remained a concern, in particular when<br />
referring pediatric patients for cardiac<br />
CT. With the Flash Spiral mode of the<br />
second generation Dual Source CT,<br />
pediatric patients can be scanned at<br />
ultra low dose, as in this case at 1.63<br />
mGy (effective dose 0.644 mSv). Apart<br />
from dose concerns, additional challenges<br />
have been associated with imaging<br />
pediatric congenital heart disease


![WalkAway plus Technical Specifications [41 KB] - Siemens Healthcare](https://img.yumpu.com/51018135/1/190x253/walkaway-plus-technical-specifications-41-kb-siemens-healthcare.jpg?quality=85)