SOMATOM Sessions - Siemens Healthcare
SOMATOM Sessions - Siemens Healthcare
SOMATOM Sessions - Siemens Healthcare

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>SOMATOM</strong> <strong>Sessions</strong><br />
The Difference in Computed Tomography<br />
Issue Number 26/May 2010<br />
International Edition<br />
Cover Story<br />
The Best of Both Worlds<br />
in Neuro Imaging<br />
Page 6<br />
News<br />
Best Balance Between<br />
Image Quality<br />
and Reduced Dose<br />
Page 18<br />
Business<br />
More for Less in Monaco<br />
Page 28<br />
Clinical<br />
Results<br />
<strong>SOMATOM</strong> Defi nition AS+:<br />
CT Perfusion With<br />
Extended Coverage for<br />
Acute Ischemic Stroke<br />
Page 50<br />
Science<br />
CT in Pediatrics: Easier<br />
and Safer With the Flash<br />
Page 62
Editorial<br />
“Our new neurological<br />
software combined with<br />
the <strong>SOMATOM</strong> Defi nition<br />
line of scanners repre-<br />
sents a quantum leap<br />
in speed, low dose and<br />
diagnostic accuracy.”<br />
Sami Atiya, PhD, Chief Executive Officer,<br />
Business Unit Computed Tomography, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
Cover Page: With Volume Perfusion CT Neuro fused with carotid CT Angiography the perfusion status of the brain tissue<br />
can be observed. Courtesy of University Hospital Göttingen, Germany.<br />
2 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine
Dear Reader,<br />
Imagine an emergency room only a<br />
few short years ago: in the middle of<br />
the night, a 55-year-old, unconscious<br />
patient is wheeled in. All neurologic<br />
observations indicate stroke. But<br />
how severe? Is it an occlusion or a<br />
hemorrhage and where is it located?<br />
All crucial questions that demand fast<br />
answers! The physician on duty could<br />
request a head CT examination that<br />
could possibly involve two scans at 15<br />
to 30 mSv radiation dose. The physician<br />
would then begin with extensive postprocessing<br />
– possibly using a PACS<br />
Workstation before the CT results could<br />
provide life the necessary clinical information<br />
required. Not a very pleasant<br />
alternative for the physicians or the<br />
patient.<br />
Now imagine the same situation in a<br />
modern emergency room equipped with<br />
<strong>Siemens</strong> cutting-edge technology such<br />
as <strong>SOMATOM</strong> Definition Flash scanner –<br />
that scans faster than all other CT<br />
scanners on the market – with latest<br />
neuro imaging software and syngo.via<br />
software that “post-process on-the-fly”<br />
Within minutes, the physician would<br />
have access to the head scan results with<br />
all post-processing completed at lowest<br />
possible dose, including non-enhanced<br />
CT for exclusion of hemorrhage, complete<br />
vascular status plus functional<br />
information.<br />
André Hartung,<br />
Vice President<br />
Marketing and Sales<br />
Business Unit CT,<br />
<strong>Siemens</strong> <strong>Healthcare</strong><br />
With syngo.via, <strong>Siemens</strong>’ new workplace<br />
software, all time consuming<br />
pre- and post-processing steps are<br />
eliminated and all diagnostic information<br />
– including information from<br />
other modalities such as MR, MI and<br />
PET – are available in almost real time.<br />
Best possible image quality is provided<br />
with sophisticated “signal boost”<br />
technologies or image-optimizing<br />
techniques resulting in definitive<br />
grey and white tissue differentiation<br />
in neuro imaging. Excellent image<br />
quality and fast processes are beneficial<br />
for both physicians and patients<br />
as they are preconditions for highest<br />
diagnostic accuracy and, at the same<br />
time, low dose safety for the patient.<br />
In all patient groups, including difficult<br />
obese and pediatric patients, as well as<br />
emergency room situations, safety is<br />
strongly linked to ALARA (As Low As<br />
Reasonably Achievable) radiation exposure.<br />
In the past, especially in acute<br />
clinical cases, lowering the radiation<br />
exposure when utilizing CT for diagnosis<br />
was not the primary focus. In stroke<br />
cases, “minutes equaled mind” and for<br />
accident victims, minutes could mean<br />
life or death. Today, thanks to <strong>Siemens</strong>’<br />
significant leadership in bringing low<br />
dose CT into clinical routine, image<br />
quality is not necessarily tied to a slower<br />
diagnosis path and higher dose expo-<br />
* syngo.via can be used as a standalone device or together with a variety of syngo.via based software options,<br />
which are medical devices in their own rights..<br />
André Hartung<br />
Editorial<br />
sure. CT is steadily moving into the first<br />
line of emergency and stroke imaging<br />
mainly because of the wide diagnostic<br />
spectrum, speed and diagnostic precision.<br />
Providing all the advantages in<br />
CT imaging aligned with measures to<br />
minimize the radiation exposure has<br />
always been one of <strong>Siemens</strong> key goals.<br />
Therefore we have recently introduced<br />
new technical developments like IRIS to<br />
reduce radiation exposure to the lowest<br />
level in the CT industry. In functional<br />
imaging, e.g. for CT brain perfusion, the<br />
dose can be reduced by up to 50 % with<br />
4D Noise Reduction, without compromising<br />
image quality. And our Adaptive<br />
Dose Shield completely eliminates pre-<br />
and post-spiral radiation that cannot be<br />
utilized for image reconstruction. These<br />
are only a few examples from dozens of<br />
additional large and small improvements<br />
developed by our dedicated employees<br />
to make the radiologist’s life easier and<br />
the patient’s healthcare better. You will<br />
find many of these reported in this, and<br />
in future editions of <strong>SOMATOM</strong> <strong>Sessions</strong>.<br />
Good reading,<br />
Sincerely<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 3
Content<br />
Content<br />
Cover Story<br />
6<br />
The Best of Both Worlds<br />
6 Exciting advances in computed<br />
tomography (CT) examination<br />
methods, including low dose<br />
protocols, technical innovations<br />
such as whole brain CT Perfusion,<br />
Dual Energy or Neuro Best Contrast<br />
applications and groundbreaking<br />
radiological research have dramatically<br />
changed the diagnostic<br />
approach for reading physicians<br />
by enabling new indications and<br />
improved timing in the examination<br />
of patients with acute neurological<br />
deseases. <strong>SOMATOM</strong> <strong>Sessions</strong><br />
discussed with five experienced<br />
physicians how CT can routinely be<br />
used as the key diagnostic modality<br />
in neuro imaging before the start<br />
of appropriate treatment.<br />
4 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
Cover Story<br />
6 The Best of Both Worlds in Neuro<br />
Imaging<br />
News<br />
24<br />
International CT Image Contest<br />
at Lowest Dose<br />
16 Affordable Performance in 16- and<br />
64-slice CT<br />
18 Best Balance Between Image Quality<br />
and Reduced Dose<br />
19 IRIS Now Extended to <strong>SOMATOM</strong><br />
Definition AS 20 and <strong>SOMATOM</strong><br />
Definition AS 40<br />
20 syngo CT 2010B Now Available:<br />
New Software Version for the<br />
<strong>SOMATOM</strong> Definition AS Launched<br />
20 Worldwide Dose Counter<br />
21 syngo.via Workstation Face-off<br />
<strong>Sessions</strong><br />
22 syngo.via CT Speedometer<br />
24 International CT Image Contest –<br />
Highest Image Quality at<br />
Lowest Dose
– Highest Image Quality<br />
Business<br />
28 More for Less in Monaco<br />
30 New Feature: Neuro Image Quality<br />
Surpasses all Expectations<br />
Clinical Results<br />
Cardio-Vascular<br />
32 Adenosine Myocardial Stress<br />
Imaging Using <strong>SOMATOM</strong><br />
Definition Flash<br />
34 <strong>SOMATOM</strong> Definition Flash:<br />
Visualization of the Adamkiewicz<br />
Artery by IV-CTA in Dual Power Mode<br />
36 Dynamic Myocardial Stress Perfusion<br />
38 Pre-operative Exclusion of Coronary<br />
Artery Stenosis With Less Than<br />
1 mSv Dose<br />
40 Utilizing Ultra Low Dose of 0.05 mSv<br />
for Premature Baby With Congenital<br />
Heart Disease<br />
42 <strong>SOMATOM</strong> Definition Flash: Pediatric<br />
Patient Without Sedation and<br />
Breath-Holding<br />
44 <strong>SOMATOM</strong> Definition Flash: Dual<br />
Energy Coronary CT Angiography for<br />
Evaluation of Chest Pain After RCA<br />
Revascularization<br />
52<br />
Vasospasm After Subarachnoid Hemorrhage:<br />
Volume Perfusion CT Neuro<br />
Oncology<br />
46 3D Guided RF Ablation and CT<br />
Perfusion – a New Combination for<br />
Monitoring of Treatment Response<br />
48 <strong>SOMATOM</strong> Definition Flash:<br />
Routine Re-staging of Oesophageal<br />
Carcinoma Utilizing IRIS Technology<br />
Neurology<br />
50 <strong>SOMATOM</strong> Definition AS+: CT Perfusion<br />
With Extended Coverage for<br />
Acute Ischemic Stroke<br />
52 Vasospasm After Subarachnoid<br />
Hemorrhage: Volume Perfusion CT<br />
Neuro<br />
Acute Care<br />
56 Dual Energy Scanning: Diagnosis<br />
of Ruptured Cocaine Capsule<br />
58 Progressive Kidney Hematoma<br />
Post-interventional Biopsy<br />
60 <strong>SOMATOM</strong> Definition Dual Source<br />
High Pitch vs. Routine Pitch Scanning<br />
in a Pediatric Lung Low Dose<br />
Examination<br />
Science<br />
Content<br />
64<br />
Study Finds Atherosclerosis in 3,500<br />
Year old Egyptian Mummies<br />
62 CT in Pediatrics: Easier and Safer<br />
With the Flash<br />
64 Study Finds Atherosclerosis in<br />
3,500 Year old Egyptian Mummies<br />
65 Independent Validation of Perfusion<br />
Evaluation Software<br />
66 Reduced Procedure Time and Radiation<br />
Dose in Interventional CT Workflow<br />
68 Scientific Validation of the <strong>SOMATOM</strong><br />
Definition Flash<br />
Life<br />
70 Behind the Scenes: CT Scan Protocols<br />
72 First syngo.via Hands-on Workshops<br />
at ECR 2010<br />
72 Upcoming Events & Congresses<br />
73 Training Website for Knowledge<br />
Improvement<br />
73 Free Trial Licenses for Neuro Imaging<br />
74 Frequently Asked Questions<br />
74 Dual Energy CT: Learning From the<br />
Experts<br />
75 Clinical Workshops 2010<br />
76 <strong>Siemens</strong> <strong>Healthcare</strong> – Customer<br />
Magazines<br />
77 Imprint<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 5
Coverstory<br />
6 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine
The Best of Both Worlds in<br />
Neuro Imaging<br />
Exceptional Image Quality Meets Lowest Dose<br />
in Neuroradiology<br />
Exciting advances in computed tomography<br />
(CT) examination methods, including<br />
low dose protocols, technical<br />
innovations such as whole brain CT<br />
Perfusion, Neuro BestContrast or Dual<br />
Energy applications and groundbreaking<br />
radiological research have dramatically<br />
changed the diagnostic approach for<br />
reading physicians by enabling new indications<br />
and improved timing in the examination<br />
of patients with acute neurological<br />
deseases. CT is routinely used as<br />
the key diagnostic modality in neuro<br />
imaging before the start of appropriate<br />
treatment to detect or exclude intracranial<br />
hemorrhage, either traumatic or<br />
non-traumatic, or to detect other causes<br />
of acute onset of neurological disease,<br />
such as stroke, intracerebral tumors, or<br />
hematoma. Rapid evaluation is critical<br />
after trauma and with symptoms such<br />
as weakness, headache, and dizziness,<br />
which is why CT is the modality of<br />
choice in these scenarios.<br />
Exceptional image quality is key to optimize<br />
diagnosis, and lower dose imaging<br />
helps to minimize the risk to the patient.<br />
It is often said that the price of improved<br />
image quality with CT is increased radiation<br />
dose, but <strong>Siemens</strong> has shown that<br />
high quality, low dose imaging is possible<br />
in even the most challenging neuroradiology<br />
applications. Whole brain CT<br />
Coverstory<br />
At Duke University Medical Center in Durham, North Carolina, USA and<br />
elsewhere, <strong>Siemens</strong> equipment is helping radiologists combine exceptional<br />
image quality in neuro imaging with innovative dose-reducing features<br />
to maximize diagnostic confi dence.<br />
By Sameh Fahmy<br />
Perfusion imaging with <strong>Siemens</strong>’ unique<br />
Adaptive 4D Spiral and the use of CT<br />
Angiography from the aortic arch to the<br />
cranium are further expanding possibilities,<br />
increasing the diagnostic confidence<br />
of neurologists and potentially enabling<br />
more appropriate treatment decisions.<br />
“By providing really good image quality,<br />
we are able to improve the efficiency of<br />
care,” says David S. Enterline, MD, Associate<br />
Professor of Radiology and Division<br />
Chief of Neuroradiology at Duke University<br />
Medical Center in Durham, North<br />
Carolina, USA. “And through dose savings,<br />
we can minimize the risk to patients.”<br />
Neuro BestContrast<br />
Although newer techniques are revolutionizing<br />
stroke assessment, the gold<br />
standard for the initial diagnosis of<br />
stroke and intracranial hemorrhage is<br />
still non-contrast imaging of the brain.<br />
<strong>Siemens</strong> has always placed emphasis on<br />
providing the highest image quality on<br />
all of their scanners for this challenging<br />
application. Now, <strong>Siemens</strong> has taken<br />
image quality to the next level. Last<br />
year, Duke became the first hospital in<br />
the United States to install <strong>Siemens</strong>’<br />
Neuro BestContrast, an application that<br />
dramatically increases gray/white matter<br />
differentiation in non-contrast head CT<br />
“Neuro BestContrast<br />
allows radiologists<br />
to better visualize<br />
the gray/white matter<br />
interface to see<br />
subtle edema and<br />
signs of stroke, and<br />
to better delineate<br />
the cortical margin.”<br />
David S. Enterline, MD, Division Chief<br />
Neuroradiology, Duke University Medical<br />
Center in Durham, North Carolina, USA<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 7
Coverstory<br />
1A 1B 1C<br />
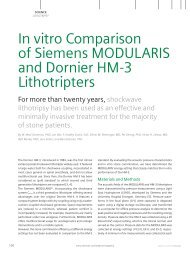
1 Comparing conventional head CT imaging (Fig. 1A) with the new IRIS technology (Fig. 1B) shows decreased image noise. Combining IRIS<br />
with Neuro BestContrast technology provides very high image quality with decreased noise by utilizing reduced radiation dose (Fig. 1C).<br />
exams using the <strong>SOMATOM</strong> Definition<br />
line of scanners. Enterline says that Neuro<br />
BestContrast allows radiologists to<br />
better visualize subtle edemas as well<br />
as subtle signs of stroke, and to better<br />
delineate the cortical margin, adding,<br />
“My colleagues and I uniformly feel that<br />
with better image quality, our comfort<br />
level and our ability to make diagnoses<br />
are significantly increased.”<br />
The improved image quality experienced<br />
by Enterline and his colleagues at Duke<br />
is also evidenced by clinical data and the<br />
experience of radiologists in Europe. In<br />
a blinded study whose results were presented<br />
at the 2009 scientific assembly<br />
and annual meeting of the Radiological<br />
Society of North America, neuroradiologists<br />
preferred Neuro BestContrast data<br />
sets in 97 % of cases. 1 Other readers,<br />
who viewed the Neuro BestContrast<br />
data set side-by-side with the traditional<br />
images, also rated image quality better<br />
in more than 90 % of the cases and<br />
lesion conspicuity higher in more than<br />
50 % of the cases.<br />
8 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
At the University Hospital in Göttingen,<br />
Germany, Peter Schramm, MD, Deputy<br />
Head of the Department of Neuroradiology,<br />
was able to compare images<br />
acquired before and after the implementation<br />
of Neuro BestContrast in a patient<br />
with head trauma whose hospitalization<br />
coincided with the hospital’s transition<br />
to the new software. “We were able to<br />
perform an exact comparison intraindividually,<br />
and in that case it was really<br />
impressive to see the improvement that<br />
came along with Neuro BestContrast,”<br />
“I think Neuro BestContrast and<br />
IRIS work perfectly with each<br />
other and have additive value<br />
in reducing dose.”<br />
Christoph Becker, MD, Professor of Radiology and Section Chief of CT and PET/CT<br />
at Munich University Hospital, Munich, Germany
Schramm says. “The delineation of the<br />
edema and the margins of the edema<br />
were definitely better visualized using<br />
Neuro BestContrast, and the same applies<br />
to the changes that occur in acute<br />
stroke.”<br />
Neuro BestContrast improves non-contrast<br />
head images by taking advantage<br />
of the fact that clinically important information<br />
from CT scans is contained in medium<br />
and low frequencies, while high frequencies<br />
are dominated by image noise.<br />
The software processes high-frequency<br />
data differently than the low-to-medium<br />
frequency data, resulting in improved<br />
tissue contrast without the amplification<br />
of image noise.<br />
Enterline says the use of Neuro BestContrast<br />
has the potential to reduce radiation<br />
dose as well. His preliminary data has<br />
documented a 15 to 20 % improvement<br />
in gray/white matter differentiation that<br />
can allow for image acquisition at a lower<br />
dose than is currently used. “Our institution<br />
has traditionally fought for lower<br />
dose,” he says, “and I think this will now<br />
allow us to further reduce our dose.”<br />
IRIS<br />
Neuro BestContrast can be combined<br />
with another new <strong>Siemens</strong> technology<br />
known as Iterative Reconstruction in<br />
Image Space (IRIS) to reduce dose and<br />
improve image quality even further.<br />
“I think they work perfectly with each<br />
other and have additive value,” says<br />
Christoph Becker, MD, Professor of Radiology<br />
and Section Chief of Computed<br />
Tomography and PET/CT at Ludwig-Maximilians-University<br />
in Munich, Germany.<br />
Iterative reconstruction uses a correction<br />
loop to improve image quality in several<br />
steps, or iterations. The idea was first<br />
introduced in the 1970s, but the computing<br />
power and time required for the<br />
reconstruction made it impractical for<br />
use in clinical settings. An alternative<br />
known as statistical image reconstruction<br />
reduced the time associated with iterative<br />
reconstruction but produced a texture<br />
that radiologists found unacceptable.<br />
With IRIS, <strong>Siemens</strong> took a different<br />
approach. The algorithm takes all of the<br />
data, which contains fine details as well<br />
as significant amounts of noise, com-<br />
2<br />
Iterative Reconstruction in Image Space (IRIS)<br />
Fast Image Data Space<br />
Slow Raw Data Space<br />
Compare<br />
Strong artifact and dose reduction<br />
Well-established image impression<br />
Fast reconstruction in image space<br />
bines it in a master image and cleans it<br />
up in the fast-processing image space<br />
rather than in the slow-processing raw<br />
data area. The result is that high spatial<br />
resolution is preserved and noise is reduced<br />
– without disrupting workflow.<br />
Becker says the combination of Neuro<br />
BestContrast and IRIS, which is available<br />
on the <strong>SOMATOM</strong> Definition line of<br />
scanners, allows him and his colleagues<br />
to better differentiate the basal ganglia<br />
and to see subtle signs of stroke. He<br />
adds that IRIS also reduces the blooming<br />
Image data<br />
recon<br />
Master<br />
recon<br />
Image<br />
correction<br />
Coverstory<br />
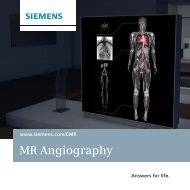
2 IRIS takes all of the data, which contains fine details as well as significant amounts<br />
of noise, combines it in a master image and cleans it up in the fast-processing image space<br />
rather than in the slow-processing raw data area. The result is that that high spatial resolution<br />
is preserved and noise is reduced – without disrupting workflow.<br />
of dense structures such as bone and<br />
calcium, making it easier to visualize<br />
or rule out subarachnoid hemorrhage.<br />
Preliminary data from Becker show that<br />
IRIS reduces dose by 25 % in head CT<br />
exams yet achieves the same level of<br />
noise as filtered back projection, the traditional<br />
method for image reconstruction.<br />
Becker notes that clinicians can<br />
also choose to use the same dose as filtered<br />
back projection yet deliver significantly<br />
better image quality using IRIS.<br />
In the United States, Ridgeview Medical<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 9
Coverstory<br />
Center in Waconia, Minnesota, USA installed<br />
IRIS on its <strong>SOMATOM</strong> Definition<br />
AS 40-slice CT and its Definition AS+<br />
128-slice scanner early in 2010. Chief<br />
of Radiology, David Gross, MD, directly<br />
compared images produced using IRIS<br />
with traditional filtered back projection<br />
images and then enthusiastically adopted<br />
IRIS. “After two or three days, we<br />
decided that there’s no sense in even<br />
comparing anymore,” Gross says. “With<br />
the improvement in radiation dose, the<br />
image quality is not changed, so we<br />
just switched right over to it.”<br />
Neuro BestContrast and IRIS build upon<br />
other <strong>Siemens</strong> innovations in neuro<br />
imaging that maximize diagnostic confidence.<br />
The “Posterior Fossa Optimization”<br />
algorithm, which was introduced in 2001<br />
and is implemented in all <strong>SOMATOM</strong><br />
Sensation and Definition scanners,<br />
significantly reduces streaks and dark<br />
bands, known as Hounsfield Bars, to<br />
allow for better resolution with less<br />
artifact. <strong>Siemens</strong>’ z-Sharp Technology<br />
provides routine isotropic resolution of<br />
0.33 mm, one of the industry’s highest,<br />
enabling the visualization of small<br />
anatomical details such as fine vascular<br />
structures. For ultra-high-resolution bone<br />
imaging for inner ear structures, <strong>Siemens</strong>’<br />
z-UHR Technology provides 0.24 isotropic<br />
resolution.<br />
Perfusion CT and CTA<br />
While non-contrast head CT exams are<br />
still important for excluding intracranial<br />
“With the improvement<br />
in radiation<br />
dose using IRIS,<br />
the image quality<br />
is not changed, so<br />
we just switched<br />
right over to it.”<br />
David Gross, MD, Chief of Radiology<br />
Ridgeview Medical Center, Waconia,<br />
Minnesota, USA<br />
hemorrhage and ischemic stroke mimics,<br />
the use of perfusion CT imaging is increasingly<br />
being adopted. “Dynamic CT<br />
Perfusion imaging, which can be acquired<br />
immediately after the non-contrast head<br />
10 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
CT while the patient is still in the scanner,<br />
allows improved detection of acute<br />
stroke, which has been substantiated in<br />
several studies,” says Ke Lin, MD, Assistant<br />
Professor of Radiology at New York<br />
University Langone Medical Center in<br />
New York City, USA. In a study of 100<br />
patients presenting to the emergency<br />
department within three hours of stroke<br />
onset, Lin and his colleagues found that<br />
CT Perfusion provided significantly improved<br />
sensitivity and accuracy in acute<br />
stroke detection over non-contrast CT.<br />
Specifically, the researchers found that<br />
CT Perfusion revealed 64.6% of acute<br />
infarctions compared to 26.2 % for noncontrast<br />
CT. CT Perfusion also had an accuracy<br />
of 76 % compared to an accuracy<br />
of 52 % for non-contrast CT. 2<br />
Lin and his colleagues obtained CT Perfusion<br />
data from a z-direction coverage<br />
of 24 mm centered at the mid-basal<br />
ganglia which maximizes the visualization<br />
of the middle cerebral artery territory.<br />
Still, the researchers noted that<br />
they missed ten infarcts that were outside<br />
of this volume of coverage. The advent<br />
of whole brain CT Perfusion using<br />
<strong>Siemens</strong>’ unique Adaptive 4D Spiral, however,<br />
further increases the value of CT<br />
Perfusion by expanding the scan range.<br />
The revolutionary scan mode, which is<br />
available on the <strong>SOMATOM</strong> Definition<br />
line of scanners, overcomes the limitations<br />
of a static detector design by applying<br />
a continuously repeated bi-directional<br />
table movement that smoothly<br />
“Dynamic CT Perfusion imaging, which can<br />
be acquired immediately after the noncontrast<br />
head CT while the patient is still in<br />
the scanner, allows improved detection of<br />
acute stroke, which has been substantiated<br />
2, 4<br />
in several studies.”<br />
Ke Lin, MD, Assistant Professor of Radiology, Department of Radiology, New York University<br />
Langone Medical Center, New York, USA
3<br />
moves the patient in and out of the<br />
gantry over the desired scan range. Lin<br />
has recently switched to a <strong>SOMATOM</strong><br />
Definition AS+ Scanner with all the<br />
advantages of full brain coverage. “With<br />
the increased coverage, we now expect<br />
further improvement in acute stroke<br />
detection accuracy, as well as the full<br />
delineation of the ischemic penumbra<br />
and the infarct core,” Lin says.<br />
The stroke imaging workflow at NYU<br />
Langone Medical Center also includes<br />
a CT Angiography immediately following<br />
the CT Perfusion exam to evaluate clot<br />
location, clot burden, and collateral recruitment.<br />
Lin adds that the information<br />
is also used for planning interventional<br />
procedures such as mechanical thrombectomy.<br />
Lin says the fast image acquisition of<br />
the <strong>SOMATOM</strong> Definition AS+ 128-slice<br />
scanner, combined with the rapid postprocessing<br />
of the <strong>Siemens</strong> syngo Volume<br />
Perfusion CT Neuro software, allows<br />
reading physicians to arrive quickly at an<br />
appropriate treatment decision through<br />
a smooth, fast, and user-friendly workflow.<br />
A number of steps are automated,<br />
including motion correction, bone segmentation,<br />
arterial input function determination,<br />
and vascular pixel elimination.<br />
The software allows for simultaneous<br />
visualization of functional parametric<br />
maps of cerebral blood flow, cerebral<br />
blood volume, time to peak, mean transit<br />
time and other clinically important<br />
information. With the click of a button,<br />
clinicians can toggle between axial,<br />
sagittal and coronal reformations.<br />
Lin and his colleagues acquire the CT<br />
Perfusion data for the whole brain in<br />
just 45 seconds. Next, CT Angiography<br />
data from the aortic arch through the<br />
whole brain, a scan range of typically<br />
more than 30 cm, is acquired in a couple<br />
of seconds to deliver valuable information<br />
about the feeding vessels that<br />
are not covered by the initial perfusion<br />
scan. Post-processing takes an additional<br />
three to five minutes. In total, when<br />
time for interpretation is accounted for,<br />
the use of CT Perfusion and CT Angio-<br />
Coverstory<br />
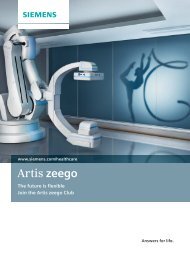
3 Perfusion CT<br />
imaging is increasinglybeing<br />
adopted in<br />
daily routine.<br />
This function<br />
overcomes the<br />
limitations of a<br />
static detector<br />
design, which<br />
provides full<br />
brain coverage,<br />
and the potential<br />
for improvement<br />
in diagnostic<br />
accuracy<br />
for acute stroke.<br />
graphy adds approximately 10 minutes<br />
to the acute stroke workflow. “That’s not<br />
a lot of time considering that the additional<br />
information provided by the CT<br />
Perfusion and the CT Angiography may<br />
have very important implications for the<br />
patient’s treatment and management,”<br />
Lin says.<br />
Reducing Dose in CT Perfusion<br />
Lin recognizes that, while the use of CT<br />
Perfusion is moving from academic<br />
medical centers to community hospitals,<br />
some barriers to its widespread adoption<br />
remain. Chief among them is a concern<br />
about the radiation dose associated with<br />
the acquisition of CT Perfusion and CT<br />
Angiography data. The use of <strong>Siemens</strong><br />
4D Noise Reduction, however, can reduce<br />
the radiation noise of dynamic CT<br />
Perfusion. The reconstruction technique<br />
treats the static anatomical information<br />
differently from the dynamically changing<br />
perfusion information that results<br />
from the in and outflow of the contrast<br />
agent. By sampling multiple passes over<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 11
4<br />
5<br />
Coverstory<br />
12 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
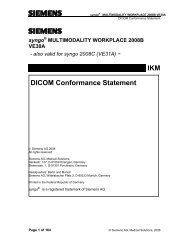
4 With Volume<br />
Perfusion CT (VPCT)<br />
fused with carotid<br />
CTA the perfusion<br />
status of the brain<br />
tissue can be revealed.<br />
This patient<br />
presented after<br />
onset of stroke and<br />
underwent lysis<br />
therapy. The followup<br />
examination<br />
showed a complete<br />
revascularization<br />
of the previously<br />
hypoperfused area.<br />
Courtesy of University<br />
Hospital Göttingen,<br />
Germany.<br />
5 With Dual Energy<br />
(DE) Bone Removal<br />
vascular structures<br />
can quickly be separated<br />
from the bones<br />
even in difficult areas<br />
such as the base of<br />
the skull. This clearly<br />
proves the clinical<br />
benefit of DE for<br />
clinical routine.<br />
Courtesy of University<br />
Hospital Munich,<br />
Campus Großhadern,<br />
Germany.<br />
the same volume it allows for the reduction<br />
of image noise. So the initial scan<br />
can be performed with a lower tube<br />
current, thus saving dose. The result<br />
is that radiation dose is reduced by<br />
up to 50 % while retaining equivalent<br />
diagnostic information.<br />
Although such dose-saving features can<br />
benefit patients, Lin cautions that the<br />
issue of dose must be kept in context<br />
during an acute stroke. “The acute critical<br />
ischemic event that could kill the<br />
patient takes priority over the slight increase<br />
in radiation dose that is imparted<br />
to the patient in order to arrive at a<br />
more accurate diagnosis, a clearer<br />
understanding of the patient’s pathophysiology,<br />
and a broader understanding<br />
of the acute event,” he emphasizes.<br />
Lin points out that only 2 % of acute<br />
stroke patients receive intravenous<br />
tissue plasminogen activator (tPA), the<br />
only U.S. Food and Drug Administration<br />
approved drug for acute stroke. He says<br />
this low rate is largely because of the<br />
restrictive three-hour time window in<br />
which the drug is approved for use.<br />
An additional factor is that an unknown<br />
time of onset, which occurs in up to<br />
25 % of acute stroke patients, disqualifies<br />
patients from receiving the drug.<br />
In Europe, the University of Göttingen,<br />
Germany has established stroke units<br />
where patients are examined in an elongated<br />
time window of 4.5 hours after the<br />
onset of stroke, based on results from the<br />
Third European Cooperative Acute Stroke<br />
Study 3 (ECASS III), so that more patients<br />
can benefit from tPA treatment.<br />
Rather than making treatment decisions<br />
based on the clock, the use of perfusion<br />
CT and CT Angiography can help deliver<br />
truly personalized medicine for acute<br />
stroke patients. The adage “time is brain”<br />
still applies, Lin says, but technology can<br />
enable a new paradigm that says that<br />
“physiology is brain.”<br />
“The rallying cry of ‘physiology is brain’<br />
is really a summation of the proposal<br />
to use a patient’s own pathophysiology,<br />
his own cerebral hemodynamics, to determine<br />
whether he still has significant<br />
amounts of salvageable tissue at risk<br />
and therefore should be a candidate for<br />
acute stroke therapy within the confines
of the safety profile of the various treatments,”<br />
Lin says.<br />
A Range of Neuro Imaging<br />
Options<br />
Of course, the use of CT in neuroradiology<br />
is not limited to patients with acute<br />
stroke. syngo Volume Perfusion CT<br />
Neuro software provides a rapid and<br />
automated evaluation of brain tumors<br />
that enhances the ability to grade<br />
tumors, plan biopsies, and monitor<br />
therapy. The use of MRI to image brain<br />
tumors is well established, but Schramm<br />
notes that the use of CT Perfusion can<br />
be advantageous in some cases. Intracerebral<br />
lymphomas, for instance, can<br />
be difficult to differentiate using MRI but<br />
can be easily identified using perfusion<br />
CT. “My prognosis is that CT will gain<br />
even more ground in the coming years,<br />
and this is due to the fact that it is<br />
broadly available, less expensive than<br />
MRI, and, in many cases, offers better<br />
spatial resolution,” he says.<br />
Another tool that significantly improves<br />
workflow and diagnostic confidence in<br />
the assessment of vascular structures of<br />
the head and neck is syngo.via* CT<br />
Neuro DSA (Digital Subtraction Angiography),<br />
which automates the removal<br />
of bone from images, even in difficult<br />
areas such as the base of the skull. The<br />
very robust technique uses a non-contrast,<br />
low-dose scan that is acquired before<br />
the actual CT Angiography and is<br />
then used to automatically remove all<br />
the bone structures in the scanned region.<br />
On Dual Source CT scanners such<br />
Coverstory<br />
“We were able to perform an exact comparison<br />
intra-individually, and in that<br />
case it was really impressive to see the<br />
improvement that came along with<br />
Neuro BestContrast.”<br />
Peter Schramm, MD, Deputy Head of the Department of Neuroradiology,<br />
University of Göttingen, Germany<br />
as the <strong>SOMATOM</strong> Definition and<br />
Definition Flash “syngo Dual Energy<br />
Direct Angio” offers a similar technique<br />
which permits direct removal of bone<br />
using only one scan. It uses the fact<br />
that two X-ray sources running simulta-<br />
“<strong>Siemens</strong> is committed<br />
to reducing<br />
radiation dose to<br />
the lowest possible<br />
level. Innovations<br />
such as IRIS are<br />
evidence of this<br />
commitment as is<br />
X-CARE”<br />
Sami Atiya, PhD, Chief Executive<br />
Officer, Business Unit Computed<br />
Tomography, <strong>Siemens</strong> <strong>Healthcare</strong>,<br />
Forchheim, Germany.<br />
neously at different energies can acquire<br />
two data sets with different attenuation<br />
levels.<br />
“DSA is susceptible to any motion that<br />
occurs between the exams,” Becker<br />
points out, “whereas with Dual Energy<br />
there are never any motion artifacts<br />
when we extract the bone from the<br />
dataset.” The scan speed of up to<br />
45,8 cm per second and the temporal<br />
resolution of 75 milliseconds that is<br />
possible with the <strong>SOMATOM</strong> Definition<br />
Flash can be particularly helpful in<br />
scanning the carotid arteries, Becker<br />
says, since they quickly fill with contrast<br />
media. He says the high-pitch Flash<br />
mode makes it easy to accurately time<br />
the scan so that pure arterial phase can<br />
be achieved without venous overlay that<br />
can impair visualization. Additionally,<br />
the information from dynamic CTAs<br />
using the Adaptive 4D Spiral technology<br />
offers new insights in cerebral hemodynamics<br />
to evaluate endoleaks, Takayasu<br />
disease, or complex hemodynamics of<br />
dural arteriovenous fistula. Becker adds<br />
that <strong>Siemens</strong>’ latest imaging software,<br />
syngo.via*, speeds workflow by allowing<br />
him and his colleagues to access and<br />
share data from anywhere** within the<br />
network.<br />
As Low as Reasonably<br />
Achievable<br />
“In developing advances that aim to improve<br />
the diagnostic confidence of physicians<br />
and patient outcomes, <strong>Siemens</strong><br />
is committed to reducing radiation dose<br />
to the lowest possible level following the<br />
* syngo.via can be used as a standalone device or together with a variety of syngo.via based software options, which are medical devices in their own rights.<br />
**<br />
Prerequisites include: internet connection to clinical network, DICOM compliance, meeting of minimum hardware requirements, and adherence to local data security regulations.
7<br />
Coverstory<br />
6A 6B<br />
6 X-CARE is especially important in CT for protecting dose sensitive tissue, e.g. the lenses of the eyes (Fig. 6A). To further reduce the<br />
radiation dose for the lenses, additional safety devices like an eye protector (Fig. 6B) can be used.<br />
Dose Shield<br />
2007<br />
Dose Shield<br />
Adaptive Dose Shield<br />
Up to 25 % dose reduction<br />
Selective<br />
Photon<br />
Shield<br />
2008<br />
80 kV<br />
Attenuation B<br />
Selective<br />
Photon<br />
Shield<br />
No dose penalty<br />
140 kV<br />
Attenuation A<br />
2008<br />
4D Noise<br />
Reduction<br />
Up to 50 % dose reduction<br />
7 <strong>Siemens</strong> has been a pioneer in creating a host of innovative technical features that significantly reduce radiation exposure in CT scans.<br />
Using these features may result in variant values of dose reduction.<br />
14 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine
‘as low as reasonably achievable’<br />
(ALARA) principle. Innovations such as<br />
IRIS are evidence of this commitment,<br />
as is <strong>Siemens</strong> X-CARE”, says Sami Atiya,<br />
PhD, Chief Executive Officer, Business<br />
Unit Computed Tomography, <strong>Siemens</strong><br />
<strong>Healthcare</strong> in Forchheim, Germany. The<br />
application protects sensitive organs by<br />
lowering the tube current during the<br />
portion of the rotation in which the area<br />
of concern would otherwise be near the<br />
X-ray source. Enterline, at Duke University<br />
Medical Center in Durham, USA, points<br />
out that X-CARE is especially important<br />
for protecting the lenses of the eyes,<br />
which are particularly radiosensitive. He<br />
says the technology has allowed him and<br />
his colleagues to reduce dose to the lens<br />
up to 30 % in preliminary data without<br />
a reduction in image quality. They<br />
routinely use X-CARE in their practice.<br />
Another technology that minimizes dose<br />
to patients is the <strong>Siemens</strong> Adaptive<br />
Dose Shield, available on the <strong>SOMATOM</strong><br />
2008<br />
Neuro BestContrast<br />
Up t o 30 % dose reduction<br />
Definition AS and Definition Flash scanners.<br />
With traditional spiral CT exams,<br />
patients are exposed to unnecessary<br />
radiation at the beginning and the end<br />
of the exam. The Adaptive Dose Shield<br />
automatically moves collimators into<br />
place to block this unnecessary exposure,<br />
thereby reducing dose by up to 25 %.<br />
Becker notes that the proportion of overbeaming<br />
is especially significant over<br />
small scan ranges, so pediatric patients<br />
and those requiring head CT exams<br />
stand to gain the most.<br />
Becker and his colleagues further reduce<br />
radiation dose with <strong>Siemens</strong> CARE<br />
Dose4D, which provides real-time modulation<br />
of dose, based on patient size<br />
and the anatomy being imaged. “I totally<br />
insist on using it,” Becker says. “We<br />
don’t switch this option on and off –<br />
we use it for every CT scan.”<br />
Concerns about radiation dose have<br />
moved from the medical journals and<br />
conference halls into the mainstream<br />
2008<br />
X-CARE X-ray low<br />
X-ray on<br />
Up t o 40 % dose<br />
reduction<br />
2009<br />
Image data<br />
recon<br />
Coverstory<br />
news media. Enterline and others say<br />
that, as a result, patients increasingly<br />
ask about the potential consequences<br />
of their exposure to medical imaging.<br />
Discussing the risks and benefits associated<br />
with CT imaging with patients<br />
helps reassure them, Enterline says, and<br />
so does having technology that minimizes<br />
dose. “It’s our responsibility to do what<br />
we can to minimize dose and to make<br />
sure that the studies are appropriate,”<br />
he adds. “It’s the right thing to do for<br />
patients.”<br />
Sameh Fahmy is an award-winning freelance<br />
medical and technology journalist based in<br />
Athens, Georgia, USA<br />
1 Diehn F, et al. – RSNA 2009 presentation SSE23-<br />
03: A Preliminary Study of Novel Post-processing<br />
Tool: Multi-Band Filtration of Noncontrast Head<br />
CTs.<br />
2 Lin K, et. al. – Cerebrovascular Diseases 2009;<br />
28:72-79<br />
3 Hacke W, et al. – NEJM 2008;359 (13) 1317-1329<br />
4 Thomandl B, et al. – RadioGraphics, 23:565-592<br />
Image<br />
correction<br />
Iterative<br />
Reconstruction in<br />
Image Space (IRIS)<br />
Up to 60 % dose reduction<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 15
News<br />
Affordable Performance<br />
in 16- and 64-slice CT<br />
At the European Congress of Radiology in March 2010, <strong>Siemens</strong><br />
introduced new 16- and 64-slice systems to the market: The <strong>SOMATOM</strong><br />
Emotion Excel Edition and the <strong>SOMATOM</strong> Defi nition AS Excel Edition.<br />
By Jan Freund, Steven Bell and Rami Kusama, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
The new Excel Editions from <strong>Siemens</strong><br />
are especially cost-effective versions<br />
of the <strong>SOMATOM</strong> Emotion 16-slice and<br />
<strong>SOMATOM</strong> Definition AS 64-slice scanners.<br />
The Excel Edition is the result of<br />
<strong>Siemens</strong>’ commitment to developments<br />
that bring new technology to more<br />
people through reducing the costs of<br />
these innovations. These new additions<br />
to the Emotion and Definition AS families<br />
offer customers access to 16-slice<br />
and 64-slice <strong>Siemens</strong> technology in<br />
scanners that include many of the advantages<br />
that existing Emotion and<br />
Definition AS customers know, at a<br />
significantly more advantageous price.<br />
On the one side, the <strong>SOMATOM</strong> Emotion<br />
Excel Edition is especially designed to<br />
make it easier for small and medium-sized<br />
hospitals and practices to enter the<br />
world of 16-slice computed tomography.<br />
It continues the success story of the<br />
Emotion platform that remains the most<br />
popular CT in the world.<br />
The success of the <strong>SOMATOM</strong> Emotion<br />
platform to date has been due to superb<br />
image quality, a simplified and efficient<br />
workflow, and the ability to save money<br />
over the life of the CT system. To date,<br />
there are around 7000 systems installed<br />
worldwide. The 16-slice <strong>SOMATOM</strong><br />
Emotion Excel Edition builds on the prior<br />
success of this imaging platform to bring<br />
these advantages to more customers<br />
and patients. It offers the smallest focalspot<br />
size and a high number of effective<br />
16 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
The new Excel Editions from <strong>Siemens</strong> are especially affordable versions of the <strong>SOMATOM</strong> Emotion<br />
16-slice and <strong>SOMATOM</strong> Definition AS 64-slice scanners.
detector channels for increased image<br />
clarity and resolution. It continues<br />
<strong>Siemens</strong>’ focus on dose reduction with<br />
the exclusive CARE Dose4D algorithm<br />
offering dose reduction of up to 68 % in<br />
routine scanning. Customers will also<br />
continue to benefit from the easy-to-use<br />
syngo user interface that <strong>Siemens</strong><br />
customers across all imaging modalities<br />
are familiar with.<br />
On the other side, the <strong>SOMATOM</strong><br />
Definition AS Excel Edition introduces<br />
a high-end, yet affordable 64-slice workhorse<br />
for both everyday clinical routine<br />
and advanced imaging. It will broaden<br />
the portfolio of the <strong>SOMATOM</strong> Definition<br />
AS family and continue its legacy as the<br />
world´s first adaptive scanner. Its unique-<br />
ness is the unprecedented adaptability<br />
to any patient and any clinical question,<br />
making it an expert in virtually any<br />
clinical field. With the introduction of<br />
the <strong>SOMATOM</strong> Definition AS Excel<br />
Edition, <strong>Siemens</strong> continues to lead the<br />
world of innovation by making two ends<br />
meet: bring outstanding imaging technology<br />
and advanced clinical applications<br />
to budget-minded customers.<br />
The <strong>SOMATOM</strong> Definition AS Excel<br />
Edition addresses the growing market for<br />
entry-level 64-slice scanners. Especially<br />
this segment is currently facing a very<br />
strong trend towards commoditization,<br />
demanding a reliable, cost-efficient<br />
64-slice system to realize high throughput<br />
in everyday clinical routine. For this,<br />
www.siemens.com/<br />
somatom-emotion<br />
www.siemens.com/<br />
somatom-definition-as<br />
News<br />
the scanner offers the highest degree of<br />
flexibility with its 78 cm gantry and a<br />
table load capacity of up to 300 kg thus<br />
avoiding delays and patient exclusions.<br />
Combined with the industry’s highest<br />
sub-mm resolution and coverage speed<br />
in its segement, a rotation speed of 0.33<br />
seconds and unique applications like 3Dguided<br />
CT interventions, the <strong>SOMATOM</strong><br />
Definition AS Excel Edition delivers<br />
state-of-the-art CT imaging and can<br />
cope with literally every need in clinical<br />
routine. At the same time, it sets standards<br />
in patient safety by providing a<br />
unique composition of dose protection<br />
features like CARE Dose4D, the innovative<br />
Adaptive Dose Shield, which avoids<br />
unnecessary overradition in every spiral<br />
scan, or IRIS – the Iterative Reconstruction<br />
in Image Space which allows a dose<br />
reduction of up to 60 %. With its onsite<br />
upgradeability to the standard AS<br />
64-slice and AS+ 128-slice configurations<br />
and with the smallest footprint in its<br />
segment, the new Edition is the ideal<br />
system for customers that are both<br />
performance and budget-minded.<br />
Finally, together with syngo.via* –<br />
<strong>Siemens</strong>’ new imaging software – the<br />
<strong>SOMATOM</strong> Definition AS Excel Edition<br />
grants access to a whole new world of<br />
workflow improvement.<br />
By moving from post-processing of image<br />
data to having it pre-processed and<br />
ready to review, it sets new standards in<br />
ease-of-use and thus clinical efficiency.<br />
The <strong>SOMATOM</strong> Emotion Excel Edition<br />
was released on the first of April 2010<br />
and the <strong>SOMATOM</strong> Definition AS Excel<br />
Edition on the first of May. For more<br />
information about the new Excel Editions,<br />
the local <strong>Siemens</strong> representative can be<br />
contacted.<br />
* syngo.via can be used as a standalone device or together with a variety of syngo.via based software options, which are medical devices in their own rights.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 17
News<br />
Best Balance Between<br />
Image Quality<br />
and Reduced Dose<br />
Iterative Reconstruction in Image<br />
Space (IRIS) provides individual choices<br />
and benefi ts for all patients.<br />
By Annette Tuffs, MD<br />
It is a difficult choice for physicians<br />
to decide what benefits the patient most,<br />
the highest resolution with best image<br />
quality and diagnostic confidence –<br />
or the lowest radiation level to reduce<br />
the long-term risks for their patients.<br />
Modern CT technology like IRIS cannot<br />
entirely overcome this dilemma, of<br />
course, but it provides flexible solutions<br />
that allow choices for the individual<br />
patient according to age, condition,<br />
suspected pathology and the specific CT<br />
investigation being performed, thereby<br />
permitting the reading physician to<br />
carefully weigh the benefits of highest<br />
possible resolution against the advantages<br />
of minimized radiation exposure.<br />
IRIS – A Success Story<br />
The peak of these impressive developments<br />
is IRIS, which stands for Iterative<br />
Reconstruction in Image Space. It had<br />
its debut at the 2009 RSNA meeting in<br />
Chicago and has proven to be another<br />
<strong>Siemens</strong> success story in substantially<br />
reducing radiation dose. It is based upon<br />
“iterative reconstruction,” a method first<br />
developed in the 1970s to reduce noise<br />
in CT images.<br />
Iterative reconstruction includes a “correction<br />
loop,” in which images are repeatedly<br />
calculated by assumptions. The<br />
image becomes softer in homogenous<br />
tissue regions while, at the same time,<br />
high-contrast tissue boundaries are maintained.<br />
Image resolution and image noise<br />
are no longer closely inter-dependant.<br />
However, this process required a lot of<br />
time and enormous computing capacity<br />
and therefore – before IRIS – was not<br />
feasible for use in clinical routine. Now,<br />
<strong>Siemens</strong> engineers and scientists have<br />
optimized the process and developed<br />
IRIS, where time and computing capacity<br />
are no longer an issue.<br />
“We are enthusiastic about this innovative<br />
method in CT scanning, that´s why<br />
we use it in our greatly improved daily<br />
routine,” says Professor Joseph Schoepf,<br />
MD, whose Department of Radiology at<br />
the Medical University of South Carolina,<br />
Charleston, USA, was one of the first<br />
to gain clinical experience with IRIS.<br />
His department has been using IRIS on<br />
a routine basis since autumn 2009 for<br />
about 15 patients per day.<br />
All Patients Benefi t<br />
Several university hospitals, in Germany<br />
and abroad, have already been able to<br />
gather extensive clinical experience with<br />
IRIS. One of them is the University<br />
Hospital, Erlangen in Germany, where<br />
Michael Lell, MD, Senior Physician at the<br />
Radiology Institute, has been involved in<br />
studies concerning the potential of IRIS<br />
in reducing radiation dosage. In one of his<br />
studies, that he will submit for publication<br />
in the next months, more than 70<br />
patients have been evaluated with and<br />
without IRIS. The radiologists in Erlangen<br />
were looking specifically at the abdomen.<br />
“As a preliminary result, we can say<br />
that we were able to achieve a 50 %<br />
dosage reduction while maintaining<br />
high standards of image quality,” Lell<br />
18 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
1<br />
1 Since autumn 2009 in the University Hospitals<br />
Munich and Erlangen-Nuremberg all CT scan<br />
protocols have been changed to use IRIS in clinical<br />
routine.<br />
recounts. Which patients will benefit<br />
most from the use of IRIS? “All patients<br />
should have the benefit,” says Lell, “and<br />
therefore we changed all our protocols<br />
to include IRIS.” However, there are specific<br />
patient groups that should benefit<br />
even more, for instance children, since<br />
they demand the smallest possible dose<br />
because of long-term, higher potential<br />
radiation risks and, at the same time,<br />
have smaller body structures, which are<br />
more difficult to visualize in CT scanning<br />
procedures.<br />
Lell specifically mentions the group of<br />
children and juvenile patients with mucoviscidosis,<br />
an unstable condition that can<br />
require frequent CT scans. He is optimistic<br />
that, with the ongoing fine-tuning of IRIS,<br />
further dose reductions will be possible<br />
and he is confident that the magic threshold<br />
of up to 70 % reductions can be<br />
reached.<br />
Special Object:<br />
Cardiovascular Stent<br />
Another group of patients that especially<br />
benefit from IRIS is the increasing number<br />
of obese patients of both genders<br />
and all ages. Even when the smaller of<br />
these morbidly obese patients are able to<br />
squeeze through the CT gantries, the<br />
resulting images are often substandard,<br />
sometimes strikingly so.<br />
“The diagnostic results can be greatly<br />
improved with IRIS in obese patients,”<br />
says Schoepf. His hospital mainly cares<br />
for patients with either digestive disease<br />
or cardiovascular disease. His special
interest is testing IRIS in patients with<br />
heart stents that are supposed to keep<br />
the coronary arteries open.<br />
“Coronary stents are the Achilles’ heels<br />
of radiological heart diagnostics,” says<br />
Schoepf. With IRIS, it is easier to detect<br />
whether there is a true obliteration of<br />
the stent or the so-called, “beam hardening,”<br />
that only simulates closure of the<br />
stent. Preliminary results of a study at<br />
the Medical University of South Carolina<br />
have already shown that IRIS will help<br />
to make this important distinction, that<br />
has a major impact on therapeutic decisions<br />
and results.<br />
Searching for Small Liver<br />
Metastases<br />
Another important area with far-reaching<br />
therapeutic consequences is the imaging<br />
IRIS Now Extended to <strong>SOMATOM</strong> Defi nition AS 20<br />
and <strong>SOMATOM</strong> Defi nition AS 40<br />
By Rami Kusama, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
Because at <strong>Siemens</strong> dose reduction has<br />
continued to be given top priority, assuring<br />
both patients and medical personnel<br />
the best in medical care with the least<br />
possible risk, the availiability of IRIS with<br />
the <strong>SOMATOM</strong> Definition, <strong>SOMATOM</strong><br />
Definition Flash, and <strong>SOMATOM</strong><br />
Definition AS+ and AS 64, will be extended<br />
to the <strong>SOMATOM</strong> Definition AS<br />
40, as well as AS 20. Now all scanners<br />
from the <strong>SOMATOM</strong> Definition family*<br />
will benefit from excellent diagnostic<br />
image quality with levels of dose lower<br />
than ever before. With IRIS, <strong>Siemens</strong>’<br />
smart approach to iterative reconstruction,<br />
up to 60% additional dose reduction<br />
can be achieved in a wide range of daily<br />
routine CT applications.<br />
Dose reduction with CT has been limited<br />
by the currently used filtered back projection<br />
reconstruction algorithm. When<br />
using this conventional reconstruction of<br />
acquired raw data, a trade-off between<br />
spatial resolution and image noise has to<br />
be considered. Higher spatial resolution<br />
of the liver, especially when searching<br />
for small metastases of malignant tumors<br />
elsewhere in the body. “With IRIS, we<br />
have a much better chance of finding<br />
these lesions,” says Schoepf.<br />
Konstantin Nikolaou, MD, Prof. of<br />
Radiology, Associate Chair of the Department<br />
of Radiology, Munich University<br />
Hospital, Germany, also agrees that all<br />
patients can profit from the use of IRIS,<br />
some of them more than others. Since<br />
last autumn, he and his colleagues have<br />
changed all the protocols to use IRIS. By<br />
April 2010, more than 3.000 patients of<br />
all ages and conditions profited from<br />
improved IRIS image quality or dose<br />
reduction. Overall dose reductions in all<br />
body regions of about 30 % were<br />
achieved, and current scientific studies<br />
at the University of Munich are designed<br />
increases the ability to see the smallest<br />
detail; however, it is directly correlated<br />
with increased image noise.<br />
In an iterative reconstruction, a correction<br />
loop is introduced into the image<br />
generation process. To avoid long reconstruction<br />
times, IRIS first applies a raw<br />
data reconstruction only once. During this<br />
initial raw data reconstruction, a socalled<br />
and newly developed master<br />
volume is generated that contains the full<br />
amount of raw data information, but at<br />
the expense of significant image noise.<br />
During the following iterative corrections,<br />
the image noise is removed without<br />
degrading image sharpness. The<br />
new technique results in increased image<br />
quality or dose savings of up to 60 %<br />
for a wide range of clinical applications.<br />
90 day, free trial licenses for IRIS are<br />
now also available. The local sales<br />
representative can be contacted for<br />
details.<br />
*requires syngo CT 2010A or syngo CT 2010B<br />
to prove this effect. “IRIS has improved<br />
our daily routine because of higher image<br />
quality or lower dose.” The Munich<br />
radiologists are currently running studies<br />
where the diagnostic results from IRIS<br />
images are compared with conventional<br />
images, and their recent finding have<br />
shown that an experienced radiologist<br />
can easily adjust to the new kind of<br />
image impressions. “A trained eye can<br />
benefit from the IRIS specific images –<br />
the improved spatial image resolution in<br />
high contrast areas, with less noise in<br />
the low contrast areas.”<br />
Annette Tuffs, MD, is a medical journalist<br />
based in Heidelberg, Germany. The former<br />
medical editor of the daily Die Welt has<br />
been contributing to the Lancet and the<br />
British Medical Journal since 1990.<br />
News<br />
Iterative Reconstuction in Image Space (IRIS)<br />
Fast Image Data Space<br />
Slow Raw Data Space<br />
Compare<br />
Image data<br />
recon<br />
Master<br />
recon<br />
Image<br />
correction<br />
� Up to 60 % dose reduction<br />
� Image quality improvement<br />
� Fast recon in image space<br />
� Well-established image impression<br />
� 90 day, free trial license<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 19
News<br />
syngo CT 2010B Now Available:<br />
New Software Version for the<br />
<strong>SOMATOM</strong> Defi nition AS Launched<br />
By Jan Freund, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
The new syngo software version, CT<br />
2010B, for <strong>SOMATOM</strong> Definition AS<br />
scanners, was released in April 2010.<br />
It makes IRIS (Iterative Reconstruction<br />
in Image Space) available to <strong>SOMATOM</strong><br />
Definition AS customers. With IRIS, a<br />
dose reduction of up to 60% is possible<br />
without compromising image quality.<br />
In addition, native head-image quality<br />
can be significantly improved with<br />
Neuro BestContrast without an increase<br />
in dose. By separating low and high fre-<br />
Worldwide Dose Counter<br />
By Peter Seitz, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
With the <strong>SOMATOM</strong> Definition Flash,<br />
coronary CTAs become routinely available<br />
at dose levels below 1 mSv. Now everybody<br />
can check dose values for themselves,<br />
in daily routine, worldwide, and in<br />
almost real-time. Being able to image the<br />
coronary arteries with a radiation dose of<br />
below 1 mSv is impressive in itself, but it<br />
becomes even more impressive when this<br />
happens everyday, all around the globe<br />
and not just in a few specialized cases.<br />
That’s why <strong>Siemens</strong> decided to make average<br />
doses of Flash Spiral Cardio scans –<br />
our all-new high-pitch mode for scan<br />
speeds up to 458 mm/s – publicly available.<br />
With this ultrafast scanning, the<br />
<strong>SOMATOM</strong> Definition Flash acquires the<br />
entire heart in only around 270 ms, reducing<br />
radiation exposure to the minimum,<br />
all the while maintaining the excellent<br />
image quality that previously was<br />
only possible at much higher dose levels.<br />
At www.siemens.com/low-dose anyone<br />
can observe the current average dose on<br />
the installed base. This value is updated<br />
every 30 minutes by statistical data<br />
20 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
quency data, it specificly optimizes the<br />
tissue contrast without amplifying the<br />
image noise, resulting in an improvement<br />
of signal to noise ratio of up to<br />
30 %. In dynamic studies, such as CT<br />
Perfusion images, noise can be significantly<br />
reduced. As a result, radiation<br />
dose can be lowered without compromising<br />
image quality. The Adaptive<br />
Signal Boost optimizes lower signals,<br />
e.g. when low dose or obese protocols<br />
are used. Neuro BestContrast, 4D Noise<br />
Reduction and the Adaptive Signal Boost<br />
will be available free of charge. CARE<br />
Contrast II synchronizes CT scan and<br />
contrast media injection. With its open<br />
interface technology, it is ready for<br />
future applications. The syngo CT 2010B<br />
will be delivered with all new systems<br />
beginning in May 2010 and as a field<br />
roll-out to the complete installed base<br />
of the <strong>SOMATOM</strong> Definition AS.<br />
View on the <strong>Siemens</strong> <strong>Healthcare</strong><br />
dose counter homepage.<br />
analysis that is sent from <strong>SOMATOM</strong><br />
Definition Flash installations worldwide.<br />
In addition latest news and further information<br />
are available on <strong>Siemens</strong> Low<br />
Dose CT.<br />
www.siemens.com/low-dose
syngo.via<br />
Workstation<br />
Face-off <strong>Sessions</strong><br />
By Karin Barthel, Business Unit CT,<br />
<strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
At RSNA 2009, <strong>Siemens</strong> <strong>Healthcare</strong><br />
introduced their new imaging software,<br />
syngo.via,* a client-server based software<br />
solution which allows to display<br />
most used applications across various imaging<br />
modalities – dedicated not only to<br />
general radiology but tailored to specific<br />
clinical fields such as oncology, neurology,<br />
vascular imaging and cardiology as well.<br />
Since then, syngo.via has participated at<br />
2 major face-offs. At a face-off, several<br />
industry vendors enter the arena to demonstrate<br />
cases live on their respective<br />
workplaces, permitting the audience to<br />
make an immediate, direct comparison of<br />
the software versions and results.<br />
First, syngo.via met the challenge at the<br />
6th International MDCT Symposium 2010<br />
in Garmisch-Partenkirchen, Germany,<br />
where about 1.600 CT experts were registered.<br />
Thomas Mang, MD, from the University<br />
Hospital in Vienna demonstrated<br />
the cases for <strong>Siemens</strong>. The first was a<br />
vascular case where an aneurysm needed<br />
to be evaluated. With syngo.via, Mang<br />
could fulfill all tasks ahead of time in outstanding<br />
clinical quality. Only 2 minutes<br />
were required since many steps, like table<br />
removal, bone removal, naming of vessels,<br />
curved MPRs and orthogonal views, were<br />
automatically calculated by syngo.CT<br />
Vascular Analysis.** The second case was<br />
an oncology case in which multiple liver<br />
lesions had to be measured. The automatic<br />
synchronization of datasets, the<br />
propagation of previous results and the<br />
unique Findings Navigator helped to<br />
speed up the workflow tremendously.<br />
The contouring algorithm worked perfectly<br />
and measured reliably, even for the<br />
very complex liver lesions that, in comparison<br />
to the surrounding tissue, showed<br />
very similar density.<br />
The second competition was the workstation<br />
face-off at the ECR in March 2010<br />
in Vienna, Austria. There, 3 cases where<br />
demonstrated by Marco Das, MD, from<br />
the University Hospital in Maastricht, The<br />
Netherlands. The first case was a vascular<br />
case whereby a high-grade stenosis in<br />
the common carotid artery needed to be<br />
quantified and an occlusion in the MCA<br />
segment had to be displayed. The case<br />
was completed with syngo.via with only<br />
a few steps. Due to all the automated<br />
tools, Das only had to click into the areas<br />
of interest and could show the results.<br />
The second case was a brain perfusion in<br />
which the MTT, CBF and CBV parameters<br />
had to be measured. Here it was only<br />
necessary to open the syngo Volume<br />
Perfusion CT Neuro application to accept<br />
the results and to place a ROI into the infarction.<br />
Everything else was automatically<br />
calculated by the system. All in all,<br />
this took only 45 seconds.<br />
The third case was a PET/CT case in which<br />
the assessment of response to treatment<br />
between 3 time-points had to be done<br />
with an volumetric assessment according<br />
to RECIST, WHO and volume, including<br />
percentual change between examinations<br />
as well as an metabolic SUV assessment<br />
based on PET data. With the Findings<br />
Navigator it was very simple to jump<br />
from finding to finding. And the comparison<br />
of findings was easy to use since all<br />
images such as CT, PET, Fused and MIP<br />
images were displayed next to each<br />
other. Due to the dedicated lung, liver<br />
and lymph algorithms, all kinds of lesions,<br />
no matter if large or small were<br />
contoured and measured precisely. These<br />
results showed that syngo.via currently<br />
will be an industry standard for state-ofthe-art<br />
imaging solution.<br />
News<br />
With syngo.via, a vascular case, demonstrated during the face-off in Vienna,<br />
was completed with only a few steps due to automated tools.<br />
Thomas Mang, MD,<br />
AKH, Vienna, Austria<br />
“Due to the automated<br />
features within syngo.via,<br />
manual preparation of<br />
cases is no longer necessary.<br />
Now, a radiologist can<br />
start working where he<br />
wants to start, with reading<br />
the case.”<br />
Marco Das, MD,<br />
Maastricht University<br />
Medical Center,<br />
The Netherlands<br />
“I saw the syngo.via face-off<br />
in Garmisch and was very<br />
impressed. So, when I was<br />
asked to demonstrate it in<br />
Vienna, I agreed immediately.<br />
Although the software was<br />
new for me, it was easy to<br />
learn and I was proud to<br />
demonstrate it at the ECR.”<br />
* syngo.via can be used as a standalone device or together with a variety of syngo.via based software options, which are medical devices in their own rights.<br />
**<br />
The information about this product is being provided for planning purposes. The product is pending 510 (k) review, and is not yet commercially available in the U.S.
1A<br />
News<br />
syngo.via CT Speedometer<br />
In November 2009, <strong>Siemens</strong> <strong>Healthcare</strong> introduced syngo.via, a new<br />
client-server based imaging solution concept to improve quality<br />
of patient care, to cut costs for healthcare and to help hospitals and<br />
practices optimize their workfl ows.<br />
By Karin Barthel, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
syngo.via* is a new imaging software<br />
that supports the physician’s diagnostic<br />
work with indication-specific workflows,<br />
layouts, and tools. Unlike typical radiological<br />
workplace setups – often equipped<br />
with multiple, isolated workstations –<br />
syngo.via is a server-based imaging software<br />
that can be seamlessly integrated<br />
in PACS or RIS-based working scenarios,<br />
accessible from any** PC within a clinical<br />
network.<br />
To give an overview of the many opportunities<br />
for saving time in CT, an easy<br />
to use tool has now been created: the<br />
syngo.via CT Speedometer. The CT Speedometer<br />
shows exactly how utilizing<br />
syngo.via can save time during the whole<br />
workflow, from patient registration over<br />
reading the cases up to distributing the<br />
report. Many time-consuming steps<br />
which previously had to be done manually<br />
can now be avoided.<br />
The following illustrates just a few of the<br />
time-saving features that are quickly located<br />
and explained with the CT Speedometer:<br />
Image Prefetching –<br />
Up-to-date imaging History<br />
As soon as the patient is registered or<br />
data arrives, syngo.via automatically<br />
initiates a query in all connected archives<br />
(e.g. PACS) for previous exams or reports.<br />
Any reasonable previous examinations<br />
of a patient from CT, MR, AX or other<br />
moda-lities are prefetched. Thus, a complete<br />
imaging history is available before<br />
the physician starts reading the case.<br />
Summary: Manual, time-consuming<br />
querying and loading data is history<br />
with syngo.via.<br />
Preprocessing – Reading can be<br />
Started Faster Than Ever Before<br />
For example, as soon as a vascular case<br />
arrives at the server, syngo.via automatically<br />
starts to preprocess the data set. In<br />
this case, the table removal, bone removal<br />
and the labeling of main vessels will be<br />
automatically done by syngo.CT Vascular<br />
Analysis.*** Curved MPR reformations<br />
and orthogonal views of the main vessels<br />
will also be created automatically<br />
(Fig. 1A).<br />
Summary: There is no need to prepare<br />
the data set before being able to read<br />
the case.<br />
One Click Stenosis –<br />
Measurement Straight Away<br />
In cardiac evaluations, three reference<br />
points are automatically placed before,<br />
in and after a stenosis by syngo.CT<br />
Coronary Analysis.*** The entire vessel<br />
lumen can be controlled with a dedicated<br />
profile curve displayed next to the vessel.<br />
By accepting the measurement, the<br />
results – including the images – are<br />
documented in the Findings Navigator<br />
(Fig. 1B).<br />
Summary: There is no need to go<br />
through the entire case manually.<br />
Multimodality Oncology –<br />
Holistic Oncology Imaging<br />
Because syngo.via provides multimodality<br />
imaging, it can provide additional and<br />
* syngo.via can be used as a standalone device or together with a variety of syngo.via based software options, which are medical devices in their own rights.<br />
** Prerequisites includes: internet connection to clinical network, DICOM compliance, meeting of minimum hardware requirements, and adherence to local data security regulations.<br />
*** The syngo.CT Vascular Analysis and syngo.CT Coronary Analysis options are pending 510(k) review and are not yet commercially available in the U.S.<br />
1B
The speedometer shows exactly how much<br />
time can be saved with syngo.via.<br />
www.siemens.com/ct-speedometer<br />
potentially decisive diagnostic information<br />
in oncology cases. Any image data, in<br />
addition to CT, from PET, MRI or ultrasound<br />
available for the patient, can easily<br />
be integrated into the oncology reading<br />
layout with drag and drop (Fig. 1C).<br />
Summary: There is no need to switch<br />
between different data-sets or interfaces.<br />
Lesion Picking – One Click<br />
Synchronization<br />
In Neuro Cases, syngo.via offers a oneclick<br />
aneurysm evaluation. By simply<br />
clicking on the finding, e.g., in the VRT<br />
view, the same finding will be centered<br />
in the axial, coronal and sagittal views,<br />
and the other way round (Fig. 1D).<br />
Summary: No manual update of corresponding<br />
windows is necessary.<br />
Findings Navigator –<br />
Reproducible Results<br />
While reading the patient, findings<br />
and measurements can be created, for<br />
example, the grade of stenoses or<br />
1C 1D<br />
lengths of aneurysms. These are automatically<br />
saved in the Findings Navigator.<br />
Whenever a user opens a case, the last<br />
findings are still there. By clicking on a<br />
finding, the image will again be displayed<br />
as it was before the last save.<br />
Summary: No difficult reproduction of<br />
old measurements is necessary.<br />
News<br />
“With syngo.via, I can cut the time for my cardiovascular<br />
diagnosis from 25 minutes to only 4 minutes.”<br />
Stéphane Rusek, PhD, Centre Cardio-Thoracique de Monaco, Monaco<br />
“In an acute care case, e.g. a whole body scan<br />
with multiple fi ndings – syngo.via can save up to<br />
23 minutes to diagnosis.”<br />
Marco Das, MD, University Hospital, Maastricht, The Netherlands<br />
“Due to the automatic pre-processing of syngo.via a<br />
substracted case of CT Neuro DSA can be seen immediately<br />
instead of waiting up to 5–12 min post-processing<br />
time with a traditional CT Neuro DSA software.”<br />
Jacques Kirsch, MD, Department of Radiology, Hospital Notre-Dame, Tournai, Belgium<br />
“When reading an oncology follow-up examination such<br />
as a PET/CT which demonstrates multiple foci of cancer,<br />
comparison with prior appearance is essential to<br />
report response of therapy, syngo.via can reduce this<br />
total interpretation time by 65 %.”<br />
James Busch, MD, Specialty Networks, USA<br />
Reporting – Complete<br />
Summary Automatically<br />
Finally, when the reading physician is ready<br />
to close a case, a summary including all<br />
image findings and measurements will be<br />
created and saved to the PACS system.<br />
Work can be finished with a few easy clicks.<br />
There is no need to fax or mail results.<br />
1 Time saving opportunities with<br />
syngo.via:<br />
In preprocessing alone, up to 7 min<br />
can be saved (1A). In cardiac evaluation,<br />
one-click stenosis measurement<br />
(1B) saves an additional 4 min. This<br />
also applies to multimodality oncology<br />
reading (1C), and with CT Neuro<br />
DSA aneurysm evaluation (1D), up<br />
to 1 min can be saved (results may<br />
vary; data on file).<br />
More time saving features can be<br />
found in the CT Speedometer.<br />
www.siemens.com/ct-speedometer<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 23
News<br />
International CT Image<br />
Contest – Highest Image<br />
Quality at Lowest Dose<br />
By Rami Kusama, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
Excellent image quality is an essential<br />
requirement in computed tomography<br />
(CT). At the same time, the patient’s<br />
radiation exposure should be kept as low<br />
as possible. <strong>Siemens</strong> wants to motivate<br />
its users to utilize all dose reduction<br />
features available on their CT scanners<br />
to the full extent and share their experi-<br />
1 Winner in Cardiac<br />
Moderate Atherosclerosis<br />
(<strong>SOMATOM</strong> Definition Flash /<br />
0.97 mSv dose), Yuko Utanohara,<br />
MD and co-authors:<br />
Nobuo Iguchi, MD, PhD; Kenji<br />
Horie; Tatsunori Niwa; Sakakibara<br />
Heart Institute, Japan<br />
History:<br />
A 68-year-old female, non-smoker,<br />
with a 3-year history of hyperlipidemia,<br />
shortness of breath and chest<br />
tightness on exertion was referred<br />
for detailed examination to our department<br />
after heart murmur was<br />
detected for the first time.<br />
Diagnosis:<br />
The coronary arteries showed<br />
moderate atherosclerosis on CT.<br />
Jury statement:<br />
“This case study is not only aesthetically<br />
pleasing, but in addition, it<br />
demonstrates that supreme diagnostic<br />
accuracy can be achieved at<br />
very low doses, with unambiguous<br />
visualization of the coronary artery<br />
lumen up to the very distal segments<br />
of the coronary artery tree.”<br />
ences with other users. For this reason,<br />
<strong>Siemens</strong> initiated the International CT<br />
Image Contest from October 1, 2009 to<br />
February 1, 2010 asking physicians from<br />
around the world to send in their work<br />
to compete for the best image quality at<br />
the lowest possible radiation dose.<br />
Around 300 low dose cases from more<br />
24 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
1<br />
than 30 countries were submitted and<br />
were evaluated by a jury of internationally<br />
renowned professors.<br />
The Jury<br />
Professor Stephan Achenbach<br />
University of Erlangen, Germany<br />
Professor Dominik Fleischmann
Stanford University Medical Center, USA<br />
Professor Elliot K. Fishman<br />
Johns Hopkins University Hospital, USA<br />
Professor Yutaka Imai<br />
Tokai University School of Medicine,<br />
Japan<br />
Professor Zengyu Jin<br />
Peking Medical Union College, China<br />
Professor Borut Marincek<br />
University Hospital Zurich, Switzerland<br />
Professor Maximilian Reiser<br />
Ludwig-Maximilians-University Munich,<br />
Germany<br />
Professor Uwe Joseph Schoepf<br />
Medical University of South Carolina,<br />
USA<br />
Participation<br />
Images could be submitted online on<br />
a contest website by users of the<br />
<strong>SOMATOM</strong> Definition, <strong>SOMATOM</strong> Definition<br />
AS, as well as <strong>SOMATOM</strong> Definition<br />
2<br />
Flash, in the categories of: cardiac,<br />
neuro, abdomen and pelvis, vascular,<br />
thorax, as well as Dual Energy. Every<br />
internet viewer could select their<br />
“favorite image” in a public voting.<br />
Winner Announcement<br />
The winner announcement took place<br />
at the ECR 2010 in Vienna during the<br />
Bayer Schering Pharma and <strong>Siemens</strong><br />
<strong>Healthcare</strong> joint Satellite Symposium.<br />
Winning images (Figs. 1–6) were exhibited<br />
at the Grand CT Image Gallery.<br />
For those who could not attend the<br />
ECR, the winners were announced at<br />
the same time on the contest website<br />
and via press release.<br />
www.siemens.com/Image-Contest<br />
The free contest poster can be<br />
ordered at:<br />
www.siemens.com/ct-poster<br />
<br />
Winner in public voting: Interrupted Aortic<br />
Arch (<strong>SOMATOM</strong> Definition/ 0.45 mSv dose),<br />
Pannee Visrutaratna, MD, Maharaj Nokorn<br />
Chiangmai Hospital, Thailand<br />
History: A five-month old girl has suffered from<br />
tachypnea, poor feeding, and poor weight gain<br />
since she was one month old.<br />
Diagnosis: Interrupted Aortic Arch. The arch<br />
interruption occurs distal to the origin of the<br />
left subclavian artery. The descending thoracic<br />
aorta is supplied by a large patent ductus<br />
arteriosus.<br />
2 Winner in Neuro<br />
Perfusion after Occluded Stent<br />
(<strong>SOMATOM</strong> Definition AS / 7.55 mSv<br />
dose), Robert McGregor, MD; Boundary<br />
Trails Health Centre; Canada<br />
History:<br />
Carotid CTA and perfusion imaging<br />
was obtained in a 55-year-old female<br />
post SILK stent for right internal carotid<br />
aneurysm.<br />
Diagnosis:<br />
CTA revealed occlusion of the stented<br />
right internal carotid artery. Perfusion<br />
imaging demonstrated decreased<br />
CBF, increased MTT, but maintained<br />
CBV, indicating a large perfusion<br />
defect without significant infarction.<br />
Jury statement:<br />
“The case nicely presents the potential<br />
of comprehensive stroke assessment<br />
by CT Perfusion. CT Perfusion may<br />
suffer from image noise with unsharp<br />
margins of the infarcted territory.<br />
In this example, the margins of the<br />
infarct are clearly displayed allowing<br />
determination of the extent of the<br />
infarction precisely.”<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 25
News<br />
3 Winner in Abdomen and Pelvis<br />
Cancer of Pancreas (<strong>SOMATOM</strong> Definition<br />
/ 6.34 mSv dose), Prof. Dan Han, MD<br />
and Yu-Hui Chen, MD; Hospital of Kunming<br />
Medical College; P.R. China<br />
History:<br />
A 59-year-old male had experienced upper<br />
abdominal pain for four years. A mass<br />
in the head and neck of pancreas was<br />
identified in both Ultrasound and MRI.<br />
Diagnosis:<br />
The advanced cancer of pancreas resulted<br />
in a significant narrowing in the portal<br />
vein and the collateral circulation was<br />
established.<br />
Jury statement:<br />
“This CTA shows the encasement of the<br />
portal vein / SMV confl uence making the<br />
patient unresectable. The case with the<br />
highest image quality is the one that provides<br />
the most information content for<br />
the radiologist and the referring physician.<br />
This case fulfi lls these criteria completely<br />
at a very low radiation dose.”<br />
4 Winner in Vascular<br />
Child Aortic Transposition (<strong>SOMATOM</strong><br />
Definition Flash / 0.25 mSv dose), Gregory<br />
Nicaise, MD and co-author: Philippe Everarts,<br />
MD, Centre Hospitalier de Jolimont,<br />
Belgium<br />
History:<br />
A 2-year-old child with chronic dyspnea and<br />
pulmonary infection was presented for a CT<br />
examination.<br />
Diagnosis:<br />
Aortic transposition, left bronchial stenosis,<br />
atelectasy, pulmonary clarity and air trapping<br />
were detected.<br />
Jury statement:<br />
“This case demonstrates excellent image<br />
quality achieved at ultra-low dose permitting<br />
a comprehensive and accurate diagnosis<br />
in a complex congenital heart defect.”<br />
26 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
3<br />
4
5<br />
6<br />
News<br />
5 Winner in Thorax<br />
Flash ECG Thorax (<strong>SOMATOM</strong> Definition<br />
Flash / 0.82 mSv dose), Petter Quick; CMIV<br />
Linköping University; Sweden<br />
History:<br />
A 47-year-old woman was presented to the<br />
CT-department with unspecific chest pain.<br />
Diagnosis:<br />
The CT examination showed no pathology and<br />
could successfully rule out coronary disease,<br />
pulmonary embolism as well as lung tumor.<br />
Jury statement:<br />
“This case represented everything that<br />
chest CT can be – a high quality, volume<br />
data set that can provide information<br />
for vascular imaging as well as the lung<br />
parenchyma. High quality imaging requires<br />
the right scanner, the right protocols<br />
and the right execution of these<br />
protocols. This image tells that story<br />
very nicely.”<br />
6 Winner in Dual Energy<br />
Carotid and Circle of Willis<br />
(<strong>SOMATOM</strong> Definition Flash / 1.12 mSv dose),<br />
João Carlos Costa, MD, Diagnóstico por<br />
Imagem, Lda, Portugal<br />
History:<br />
A healthy 75-year-old female was presented<br />
to the CT-department with a family history<br />
of carotid artery stenosis.<br />
Diagnosis:<br />
Small atherosclerotic plaques in the emergence<br />
of braquiocephalic trunk and left carotid artery<br />
were identified.<br />
Jury statement:<br />
“This case illustrates the power of Dual<br />
Energy CT for tissue differentiation. In<br />
a single image and at tremendously low<br />
doses, all tissue layers in the human body<br />
can be simultaneously and intuitively<br />
displayed and provide the anatomic context<br />
of the target structure, the carotid<br />
circulation.”<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 27
Business<br />
Stéphane Rusek, PhD, is convinced that syngo.via radically transforms the use of CT even for his colleagues, turning it into an all’round<br />
tool for all doctors: (from left to right) Filippo Civaia, MD, Philippe Rossi, MD, Stéphane Rusek, PhD, Laura Iacuzio, MD.<br />
More for Less in Monaco<br />
At Monaco’s Centre Cardio-Thoracique, <strong>Siemens</strong>’ latest groundbreaking<br />
image-processing software, syngo.via, is boosting the productivity of the<br />
cardio-vascular team.<br />
By Oliver Klaffke<br />
Only a few meters up from the harbor,<br />
yet still within sight of the multi-milliondollar<br />
fleet resting in the sun, is located<br />
Monaco’s Centre Cardio-Thoracique<br />
where Stéphane Rusek, PhD, head of the<br />
hospital’s IT department, is trying to<br />
extract as much diagnostic information<br />
as he can for as little cost and time as<br />
possible.<br />
Rusek’s goal is to boost the productivity<br />
of radiologists and cardiologists by using<br />
computed tomography (CT) images to<br />
diagnose cardiac cases. And syngo.via,*<br />
<strong>Siemens</strong>’ groundbreaking imaging<br />
software, he’s convinced, is the answer.<br />
syngo.via has the capacity to help<br />
medical professionals use CT images<br />
more easily and efficiently, thus freeing<br />
up more time for actual diagnosis.<br />
Stéphane Rusek is personally responsible<br />
for implementing <strong>Siemens</strong>’ latest breakthrough<br />
in image processing at the<br />
Monaco clinic. “A new era in image processing<br />
and CT diagnosis has dawned,”<br />
he says. “What the iPhone did for mobile<br />
computing, syngo.via is doing for CT. It<br />
offers a user-friendly interface that gets<br />
the most out of the technology without<br />
users even being aware of the sophisticated<br />
software responsible, let alone<br />
having to learn to manipulate it.”<br />
syngo.via has been specifically designed<br />
to free medical professionals from the<br />
burden of having to process the vast<br />
amount of images made available by<br />
today’s CT examinations. Ten years ago,<br />
28 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
such examinations delivered around<br />
50 images; nowadays they generate<br />
thousands – far too many for anyone<br />
to handle promptly and effectively.<br />
Rusek is convinced that syngo.via radically<br />
transforms the use of CT, turning<br />
it into an useful tool for all doctors.<br />
“We are on the brink of a boom in cardiovascular<br />
CT that will see it become<br />
standard and routinely used in every<br />
hospital,” he says. And the time seems<br />
ripe. Health authorities around the<br />
world appear increasingly willing to<br />
fund cardiac CT. They have been funded<br />
in the USA since early 2010, and, in<br />
Europe, German health authorities are<br />
now looking into authorizing payment<br />
for cardiac related examinations. The
certain result will be to make such<br />
exams more widely available.<br />
“The enormous benefit of the cardiovascular<br />
applications in syngo.via<br />
is that they save time,” says Rusek.<br />
“Cardiologists no longer need to carry<br />
out tasks that can be done faster and<br />
better by software.” Preparing scans<br />
for diagnosis can be extremely timeconsuming,<br />
especially in cardiac cases.<br />
For example, manually deleting the<br />
bony rib cage from images and highlighting<br />
the arteries takes a lot of effort.<br />
In Monaco, before syngo.via, cardiologists<br />
often needed up to half an hour<br />
just to prepare the images for diagnosis.<br />
Fortunately, time consuming and<br />
numerous mouse clicks to diagnosis may<br />
soon be no more than a distant memory.<br />
Today, cases can be automatically prepared<br />
and presented using syngo.via.<br />
“My guess is that five out of the six<br />
clicks that you once had to make with<br />
the mouse are no longer necessary,”<br />
smiles Rusek. As soon as his medical<br />
colleagues click to open a case in their<br />
inbox, syngo.via lets them get straight<br />
down to diagnosis. It will already have<br />
prepared the cases automatically and<br />
identified a process to meet the specific<br />
diagnostic needs. Images are immediately<br />
displayed in disease-related<br />
layouts along with the appropriate tools<br />
1<br />
for deeper investigation. The medical<br />
professionals are then carefully guided<br />
through a series of steps that they<br />
predefined in the software for their<br />
institution.<br />
“The syngo.via Cardio-Vascular application<br />
package** now cuts the time<br />
for cardio-vascular diagnosis from<br />
25 to only 4 minutes – a factor of six.”<br />
Information Available – Quality<br />
and Effi ciency<br />
“Here in Monaco, we have benefited<br />
greatly from these disease-related workflows,”<br />
says Rusek. For each diagnosis,<br />
syngo.via presents a to-do list to help<br />
professionals get all the necessary information<br />
reliably and in shortest time.<br />
Simply following these procedures is a<br />
great way to maintain the high standards<br />
that are increasingly the norm<br />
in medicine. In Monaco, the cardiology<br />
team has completely redefined its<br />
standards and processes, thanks to<br />
syngo.via. “Now everybody working here<br />
uses the same processes,” says Rusek.<br />
“This greatly reduces the risk of errors<br />
and omissions during diagnosis.<br />
And since all relevant related data are<br />
stored along with the case and are retrievable<br />
at the click of a mouse, writing<br />
reports has become much easier. “It’s<br />
Business<br />
the perfect way to organize patient<br />
documentation, so that the physician in<br />
charge can work efficiently on the case,”<br />
says Rusek.<br />
In the past, cardiologists at Centre<br />
Cardio-Thoracique often had to switch<br />
between workstations to retrieve older<br />
data stored on different computers.<br />
No longer. “In our radiology department,<br />
that’s a thing of the past,” says Rusek.<br />
Using syngo.via, cases can be easily<br />
accessed from any computer linked to<br />
the hospital’s network. Gone is the need<br />
to wait until a workstation becomes<br />
available. At the PCs on their office<br />
desks, medical professionals can immediately<br />
and conveniently view any case<br />
they want. Even specialists working at a<br />
distance can log in utilizing a broadband<br />
internet connection and get the information<br />
they need quickly and efficiently.<br />
<strong>Siemens</strong> <strong>Healthcare</strong> is dedicated to<br />
making these benefits available everywhere,<br />
not just for Stéphane Rusek and<br />
his colleagues on the beautiful shores<br />
of the Mediterranean Sea.<br />
Oliver Klaffke is a science and business<br />
writer based in Switzerland. He has been<br />
on assignment for New Scientist and<br />
Nature in the past.<br />
1 syngo.via CT Cardio-Vascular applications** for full cardiac assessment in less than 4 min: the automated case preparation, that saves up to<br />
12 typical steps together with advanced visualization tools, like the Image Sharpening Filter for calcified lesions or stents, saves up to 21 min for<br />
a full cardiac assessment (results may vary; data on file).<br />
* syngo.via can be used as a standalone device or together with a variety of syngo.via based software options, which are medical devices in their own rights.<br />
**<br />
The syngo.CT Vascular Analysis and syngo.CT Coronary Analysis options are pending 510(k) review and are not yet commercially available in the U.S.
Business<br />
New Feature: Neuro<br />
Image Quality Surpasses<br />
all Expectations<br />
A better and quicker workfl ow that leads to more time for patient care and<br />
diagnosis – this is the bottom line for Peter Schramm, MD, of the University<br />
of Göttingen, Germany, after testing the new features of syngo CT 2010B.<br />
But specifi cally for him, as neuroradiologist, the new dimension in neuro<br />
image quality is also a main improvement and a very impressive one.<br />
By Wiebke Kathmann, PhD<br />
The new software version, syngo CT<br />
2010B, offers several new features including<br />
Neuro BestContrast, 4D Noise<br />
Reduction, Iterative Reconstruction in<br />
Image Space (IRIS), CARE Contrast II and<br />
Adaptive Signal Boost. Together they<br />
truly improve the diagnostic precision<br />
and workflow as could be clearly demonstrated<br />
during the Market Entrance<br />
Phase (MEP) by Peter Schramm, MD,<br />
Deputy Head of the Neuroradiology<br />
Department at the University of<br />
Göttingen. He was among the first<br />
physicians worldwide to test the new<br />
features in the clinical environment on a<br />
<strong>SOMATOM</strong> Definition AS+ scanner. As a<br />
neuroradiologist, he was especially impressed<br />
by Neuro BestContrast because<br />
it achieves a very substantial improvement<br />
in image contrast, thereby significantly<br />
improving the distinction between<br />
gray and white matter in the<br />
brain – a very important feature in the<br />
diagnosis of acute stroke patients where<br />
tissue changes on the scale of 5 to 10<br />
HU can decide between life and death.<br />
Neuro BestContrast absolutely fulfilled<br />
Schramm’s expectations. „Simply by<br />
looking at the images in our digital<br />
Picture Archiving and Communication<br />
System (PACS), we could recognize the<br />
point in time at which the new software<br />
had been installed. A lot of our patients<br />
get a follow-up CT scan, so we could<br />
also compare scans from before and<br />
after the software was implemented.<br />
When <strong>Siemens</strong> told us that they were<br />
aiming at improving the differentiation<br />
of brain tissue, we were wondering how<br />
A better and quicker<br />
workflow that<br />
leads to more time<br />
for patient care and<br />
diagnosis – this is<br />
the bottom line for<br />
Peter Schramm,<br />
MD, of the University<br />
of Göttingen.
“At some point in the<br />
future, neuroradiologists<br />
may no longer<br />
need to perform<br />
the complete stroke<br />
CT protocol.”<br />
Peter Schramm, MD,<br />
University of Göttingen, Germany<br />
they would be able to achieve an improvement<br />
in contrast without losing<br />
spatial resolution. But they did – by<br />
processing low and high frequencies<br />
separately.“<br />
One-Stop-Shopping<br />
For clinicians performing perfusion imaging,<br />
4D Noise Reduction is the most<br />
interesting feature. Static and dynamic<br />
components are treated separately as<br />
a means to reduce noise, thus improving<br />
the image quality and clinical outcome.<br />
Schramm could confirm this in acute<br />
stroke patients, who are frequently quite<br />
agitated.<br />
The main advantage, however, that<br />
Schramm sees with 4D Noise Reduction<br />
is a reduction in radiation dose while<br />
still being able to get all the diagnostic<br />
information from one 4D volume perfusion<br />
scan. “At some point in the future,<br />
neuroradiologists may no longer need<br />
to perform the complete stroke CT<br />
protocol consisting of a non-contrast CT,<br />
a whole brain perfusion CT including 4D<br />
spiral scans and a CT Angiography of the<br />
brain vessels. Due to the precision with<br />
4D Noise Reduction, there could be ‘onestop-shopping’,<br />
the non-contrast CT<br />
could be skipped by using the first of the<br />
multi-spiral CT images before the contrast<br />
medium arrives and the angio-information<br />
could be taken from one arte-<br />
rial sequence. For the patient that would<br />
mean one instead of three CT scans,<br />
consequently a shorter examination<br />
time and, in the end, less radiation.“<br />
Less Radiation<br />
With the Iterative Reconstruction in<br />
Image Space (IRIS), <strong>Siemens</strong> recently<br />
introduced a new approach to additionally<br />
reduce dose by up to 60 % and, at<br />
the same time, improve image quality for<br />
a wide range of clinical applications. After<br />
an initial raw-data reconstruction, a<br />
newly developed master image is generated<br />
followed by several iterative corrections<br />
that remove image noise without<br />
degrading image sharpness. With this<br />
approach, IRIS achieves a similar image<br />
quality as with true iterative reconstructions<br />
but avoids the long reconstruction<br />
times, as multiple translations from and<br />
to the raw data are not needed. For<br />
Schramm, the main promise IRIS holds<br />
with this new method is a reduction of<br />
radiation dose. So far, he and his team<br />
have worked with the regular dose. After<br />
testing IRIS, they will now commence<br />
with a controlled, stepwise dose reduction<br />
during the next few weeks. In 10 %<br />
steps with about 500 neuroradiological<br />
cases each, they hope to prove that IRIS<br />
allows a reduction of radiation dose while<br />
keeping the image quality at the same<br />
level. “Most likely, IRIS will allow for a<br />
reduction by 20 % in neuroradiology. In<br />
spinal CT, I expect a reduction by 25 to<br />
30 % without any loss of image quality,”<br />
says Schramm. “In very obese patients<br />
and abdominal CT applications, I can<br />
realize a dose reduction of up to 60 %.“<br />
Saving Time<br />
Regarding the use of CARE Contrast II –<br />
the new coupling interface for scanner<br />
and bolus injector – Schramm experienced<br />
two advantages: first, the improved<br />
workflow for the technician due<br />
to the synchronization of injector and<br />
scanner and therefore improved patient<br />
care; second, and more important, the<br />
time saved due to the automatic and<br />
digital transfer of the whole dataset on<br />
contrast media, flow rate etc. to the<br />
patient protocol. ”This archiving of the<br />
complete data set – be it for legal, re-<br />
Business<br />
search, or clinical purposes – saves time,“<br />
explains Schramm.”This makes it a very<br />
interesting feature for both research<br />
and in clinical routine.“<br />
Benefi t for the Obese Patient<br />
As for the Adaptive Signal Boost,<br />
Schramm is convinced that it will improve<br />
diagnostic precision and reliability,<br />
for example in CT imaging of the spine.<br />
“This application is on the rise due to<br />
improvements in CT technology and the<br />
growing number of bariatric patients<br />
who simply do not fit into the MRT and<br />
where it is crucial to provide the required<br />
image quality for clinical evaluation.”<br />
Here the Adaptive Signal Boost<br />
improves the diagnostic accuracy in soft<br />
tissue imaging, especially of paravertebral<br />
and intra-spinal structures. “In routine<br />
examinations, these features do not<br />
“Most likely, IRIS will<br />
allow for a reduction<br />
of radiation dose<br />
by 20-30 % in neuroradiology.”<br />
Peter Schramm, MD,<br />
University of Göttingen, Germany<br />
necessitate changes in the workflow for<br />
the technician,” says Schramm, “They<br />
hardly notice the changes, whereas the<br />
clinical results are very impressive for<br />
the radiologist at the end of the line.”<br />
Wiebke Kathmann, PhD, is a frequent contributor<br />
to medical magazines in the German-speaking<br />
world. She holds a Master in biology and a PhD in<br />
theoretical medicine and was employed as an editor<br />
for many years before becoming a freelancer in<br />
1999. She is based in Munich, Germany.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 31
Clinical Results Cardio-Vascular<br />
Case 1<br />
Adenosine Myocardial Stress Imaging<br />
Using <strong>SOMATOM</strong> Defi nition Flash<br />
By Gudrun Feuchtner, 1, 4 Robert Goetti, 1 André Plass, 2 Monika Wieser, 2 Christophe Wyss, 3<br />
Fernando Vega-Higuera, 5 Hans Scheffel, 1 Michael Fischer, 1 Hatem Alkadhi, 1 Sebastian Leschka 1<br />
1 Institute of Diagnostic Radiology, University Hospital Zurich, Switzerland<br />
2 Clinic of Cardiovascular Surgery, University Hospital Zurich, Switzerland<br />
3 Cardiology Division, University Hospital, Zurich, Switzerland<br />
4 Department of Radiology II, Innsbruck Medical University, Austria<br />
5 Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany.<br />
HISTORY<br />
A 51-year-old male with atypical chest<br />
pain and intermediate coronary risk profile<br />
(cigarette smoking and hypercholesterolemia)<br />
underwent two coronary<br />
128-slice Dual Source CT Angiographies:<br />
the first under adenosine myocardial<br />
stress-imaging, the second at rest.<br />
DIAGNOSIS<br />
High-pitch CT Angiography showed<br />
severely calcified left coronary artery<br />
(Fig. 1C) with significant stenosis, and<br />
bare-metal stent in the RCA.<br />
Adenosine CT stress imaging showed<br />
a reversible myocardial perfusion<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong> Definition Flash<br />
defect indicating ischemia anteroseptal<br />
at midventricular level (Figs. 1A–1B)<br />
corresponding to left artery descending<br />
(LAD) stenosis. No defect was found inferior<br />
of right coronary artery (RCA) vascular<br />
territory. Invasive angiography<br />
confirmed a significant 90 % stenosis at<br />
mid LAD and a patent RCA bare-metal<br />
stent. Total radiation dose was 2.2 mSv<br />
for adenosine stress and rest CT scans<br />
using high-pitch Flash Spiral mode at<br />
3.4 pitch factor. The delay between both<br />
scans was 5 minutes. Scan time was<br />
0.44 seconds for each study, tube settings<br />
were 100 kV and 320 mAs, gantry<br />
rotation time was 0.28 s.<br />
32 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
COMMENTS<br />
Adenosine stress-imaging of reversible<br />
myocardial ischemia is feasable with<br />
128-slice Dual Source CT with comprehensive<br />
evaluation of coronary arteries.<br />
Assessment of PBV reversible ischemia<br />
with CT is helpful to improve accuracy of<br />
coronary CT Angiography, especially in<br />
cases of severe coronary calcification or<br />
limited in-stent lumen visibility.<br />
Scan mode Flash Spiral Pitch 3.4<br />
Scan area Heart Slice collimation 128 x 0.6 mm<br />
Scan length 135 mm Slice width 0.75 mm<br />
Scan direction Cranio-caudal Reconstruction increment 0.4 mm<br />
Scan time 0.44 s Reconstruction kernel B 26f<br />
Tube voltage 100 kV / 100 kV Volume 80 ml<br />
Tube current 320 mAs/rot. Flow rate 5 ml/s<br />
Dose modulation CARE Dose4D Start delay 10 s<br />
CTDIvol 3.09 mGy Postprocessing syngo CT Cardiac –<br />
Effective Dose 2.2 mSv (in total) Function prototype*<br />
Rotation time 0.28 s<br />
*The product is not commercially available in the US.
1A<br />
2A<br />
3A<br />
4A<br />
First CTA under adenosine stress Second CTA at rest<br />
4B<br />
1B<br />
2B<br />
3B<br />
4C<br />
1C<br />
Cardio-Vascular Clinical Results<br />
1 By injecting adenosine<br />
under stress, a perfusion defect<br />
anteroseptal was shown (arrow,<br />
Fig. 1A), which was reversible<br />
after 5 minutes Rest Scan<br />
(arrow, Fig. 1B).<br />
A significant mid LAD stenosis<br />
was detected by CT, and<br />
quantified as 90 % by invasive<br />
angiography. Distal after stenosis<br />
a severely calcified artery<br />
was found (arrow, Fig. 1C).<br />
2 Short axis at midventricular<br />
level showed anteroseptal<br />
myocardial perfusion<br />
defect during adenosine<br />
stress (Fig. 2A, arrow),<br />
which was reversible at<br />
rest (Fig. 2B, arrow).<br />
3 Color maps of the myocardium<br />
showed black/dark<br />
areas (Fig. 3A, arrow) indicating<br />
ischemic myocardium during<br />
stress. There was no defect<br />
at the inferior myocardial<br />
region supplied by RCA<br />
corresponding to patent<br />
RCA stent (Fig. 3B, arrow).<br />
4 Automated quantification<br />
of hypo-attenuating<br />
perfusion defect anteroseptal<br />
midventricular during<br />
stress (Fig. 4A, arrow) represented<br />
with the prototype<br />
of the syngo CT Cardiac<br />
Function software,* including<br />
3D segmentation (Fig. 4B).<br />
No perfusion defect inferior<br />
of RCA vascular territory could<br />
be detected (Fig. 4C, arrow).<br />
* The product is not commercially<br />
available in the US.
Clinical Results Cardio-Vascular<br />
Case 2<br />
<strong>SOMATOM</strong> Defi nition Flash:<br />
Visualization of the Adamkiewicz Artery<br />
by IV-CTA in Dual Power Mode<br />
By Yoshiyuki Mizutani, MD* and Tomoko Fujihara**<br />
*Department of Radiology, Sakakibara Heart Institute, Tokyo, Japan<br />
**Application Department CT Team, Customer Service Division, <strong>Siemens</strong>-Asahi Medical Technologies, Tokyo, Japan<br />
HISTORY<br />
A 75-year-old female was referred to<br />
the radiology department of Sakakibara<br />
Heart Institute to examine where her<br />
Adamkiewicz artery originated before<br />
treatment of her thoracic descending<br />
aortic aneurysm (TAA). The patient was<br />
scanned with Dual Source CT in dual<br />
power mode.<br />
At the referring hospital, the patient<br />
1<br />
1 TAA was clearly seen on the Dual Source CT images (VRT).<br />
had been diagnosed with TAA (descending<br />
aorta of 5.6 cm diameter) by computed<br />
tomography and echography as<br />
well as right coronary artery (RCA) stenosis<br />
by conventional angiography. She<br />
was referred to Sakakibara Heart Institute<br />
for surgical vessel replacement and<br />
coronary artery bypass grafting with<br />
saphenous vein graft to RCA.<br />
34 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
2<br />
DIAGNOSIS<br />
TAA was clearly seen on the Dual Source<br />
CT images. An artery originating from a<br />
lumbar artery was detected, bifurcating<br />
from the aorta at the upper level of the<br />
4th lumbar vertebra, entering into the<br />
spinal canal from the intervertebral foramen<br />
between the 4th and 5th lumbar<br />
vertebrae and running along the spinal<br />
cord on the ventral side up to the lower<br />
2 TAA was clearly seen on the Dual Source CT images (thin MIP).
3A<br />
3B<br />
3 Adamkiewicz artery entering into the spinal canal (Fig. 3A)<br />
from the intervertebral foramen between the 4th and 5th lumbar<br />
vertebrae and running along the spinal cord on the ventral side up<br />
to the lower level of the 12th thoracic vertebra where it changed<br />
direction forming a hairpin shaped structure (Fig. 3B).<br />
level of the 12th thoracic vertebra where<br />
it changed direction forming a hairpin<br />
shaped structure. It connected into the<br />
anterior spinal artery. According to these<br />
characteristics this artery was identified<br />
as the Adamkiewicz artery.<br />
The true lumen of the aorta was highly<br />
enhanced, reaching a CT value of 746<br />
HU at the level between the 4th and 5th<br />
lumbar vertebrae whereas the Adamkiewicz<br />
artery reached a maximum CT<br />
value of only 140 HU.<br />
COMMENTS<br />
The course of the Adamkiewicz artery<br />
needs to be determined before surgery<br />
for TAA repair to ensure that it is not<br />
damaged during surgery and to reduce<br />
the risk of postoperative paraplegia.<br />
However, visualizing the Adamkiewicz<br />
artery with intravenous (IV) CTA is a<br />
challenging task as injection and scan<br />
protocols need to be tailored to the location<br />
and size of this artery. Since the<br />
Adamkiewicz artery is a tiny vessel, a<br />
fair amount of contrast media needs to<br />
be injected at reasonably high rates to<br />
ensure that this tiny vessel is enhanced.<br />
In addition, since the Adamkiewicz<br />
artery runs partially inside the spinal<br />
canal, enough dose needs to be applied<br />
to achieve a high signal to noise ratio<br />
(SNR) in an area surrounded by bones.<br />
Dual Source CT in the dual power mode<br />
combines the power of two X-ray tubes<br />
and two generators and can therefore<br />
provide twice as much X-ray output as<br />
a single source CT at the same pitch. As<br />
a result, areas that need additional dose<br />
can be scanned at high scan speed and<br />
appropriate tube current for a high SNR.<br />
The high scan speed was essential for<br />
visualizing the Adamkiewicz artery,<br />
since it required several seconds after<br />
enhancement of the aorta until the<br />
small arteries were enhanced, then<br />
quickly scan over the required long scan<br />
range while the small arteries were still<br />
enhanced.<br />
4<br />
Cardio-Vascular Clinical Results<br />
4 Adamkiewicz artery connected into the anterior spinal artery.<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong><br />
Definition Flash<br />
Scan area Thorax-abdomen<br />
Scan length 280 mm<br />
Scan direction Cranio-caudal<br />
Scan time 8.41 s<br />
Tube voltage 100 kV / 100 kV<br />
Tube current 600 eff. mAs<br />
Dose modulation CARE Dose4D<br />
Rotation time 0.5 s<br />
Slice collimation 128 x 0.6 mm<br />
Reconstruction<br />
increment<br />
0.3 mm<br />
Reconstruction<br />
kernel<br />
B36<br />
Volume 100 ml<br />
Flow rate 5.0 ml/s<br />
Postprocessing syngo InSpace<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 35
Clinical Results Cardio-Vascular<br />
Case 3<br />
Dynamic Myocardial Stress Perfusion<br />
By Florian Schwarz, MD, Fabian Bamberg, MD, MPH, Christoph R. Becker, MD,<br />
Alexander Becker, MD, Konstantin Nikolaou, MD<br />
Department of Clinical Radiology, University of Munich, Campus Großhadern, Munich, Germany<br />
1<br />
1 Maximum intensity display of the right coronary artery, demonstrating<br />
heavy calcified plaque in the proximal segment and calcified<br />
and non-calcified plaque in the intermediate segment, causing<br />
a mild to moderate stenosis (arrow).<br />
HISTORY<br />
A 71-year-old male was referred for evaluation<br />
of stable chest pain syndrome<br />
and enrolled in a prospective cohort study<br />
to evaluate the diagnostic accuracy and<br />
clinical feasibility of dynamic myocardial<br />
stress perfusion imaging by cardiac CT.<br />
Coronary CT Angiography (CTA) and<br />
CT-based assessment of myocardial perfusion<br />
under adenosine stress was performed<br />
prior to cardiac catheterization.<br />
DIAGNOSIS<br />
Coronary CTA revealed heavy calcified<br />
plaque and a mild to moderate lesion of<br />
the right coronary artery (RCA, Figs. 1<br />
and 2). Dynamic adenosine stress perfusion<br />
imaging revealed homogeneous<br />
perfusion of the myocardium without<br />
defined perfusion defect (Figs. 4 and 5).<br />
36 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
2<br />
2 Curved multiplanar reformation of the left anterior descending<br />
coronary artery with minor calcified and non-calcified plaque in the<br />
proximal segment of the vessel (arrow).<br />
COMMENTS<br />
Non-invasive myocardial perfusion imaging<br />
by CT may represent an attractive<br />
option to determine the hemodynamic<br />
relevance of obstructive coronary lesions,<br />
or lesions with limited evaluability due<br />
to heavy calcification. However, further<br />
validation using appropriate gold standards<br />
is warranted.<br />
After undergoing the CT Perfusion scan,<br />
the patient received conventional medical<br />
therapy.
3A<br />
80<br />
60<br />
40<br />
CT [HU]<br />
20<br />
0<br />
time [s]<br />
0 5 10 15 20 25 30<br />
4<br />
Cardio-Vascular Clinical Results<br />
3 Principle: dynamic volumetric myocardial stress perfusion to quantify Myocardial Blood Flow (MBF). Comparison of different time<br />
attenuation curve (TCA) pattern with a slower and lower peak (86 ml / 100 ml / min) in an ischemic segment (Fig. 3A) and normal blood flow<br />
(MBF 159 ml / 100 ml / min) in an healthy segment (Fig. 3B).<br />
4 Systolic reconstruction display of long axis, color-coded myocardial<br />
stress perfusion image of the left ventricle indicating homogeneous<br />
perfusion (green) and the absence of a circumscribed<br />
perfusion defect.<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong> Definition<br />
5 Short axis color-coded perfusion map of the left ventricle<br />
demonstrating homogeneous perfusion (green) under<br />
adenosine stress.<br />
Scan mode Dynamic Stress Perfusion Mode Dose modulation no<br />
Scan area Left ventricular myocardium CTDIvol 94.15 mGy<br />
Scan length 72 mm Rotation time 0.28 s<br />
Scan direction Cranio-caudal Slice collimation 32 x 1.2 mm<br />
Scan time 31 s Slice width 3 mm<br />
Heart rate 72 bpm Reconstruction increment 2 mm<br />
Tube voltage 100 kV Reconstruction kernel B23f<br />
Tube current 350 mAs/rot. Post processing syngo VPCT<br />
3B<br />
100<br />
80<br />
60<br />
40<br />
CT [HU]<br />
20<br />
0<br />
time [s]<br />
0 5 10 15 20 25 30<br />
5<br />
Body Myocardium<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 37
Clinical Results Cardio-Vascular<br />
Case 4<br />
Pre-operative Exclusion of Coronary<br />
Artery Stenosis With Less Than 1 mSv Dose<br />
By Sebastian Leschka, MD* and Andreas Blaha**<br />
* Institute of Diagnostic Radiology, University Hospital Zurich, Zurich, Switzerland<br />
**<br />
Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
HISTORY<br />
A 71-year-old male patient with a history<br />
of cerebral infarction caused by a highgrade<br />
stenosis of the left internal carotid<br />
artery and lysis therapy was now referred<br />
to the radiology department to<br />
rule out coronary artery disease.<br />
In addition to the coronary CT Angiography<br />
(CTA) examination a non-enhanced<br />
calcium-scoring scan (CaSc)<br />
was performed.<br />
The CTA was acquired with a fast pitch<br />
spiral technique (Flash Spiral Cardio)<br />
while a mean heart rate of 56 bpm was<br />
present.<br />
DIAGNOSIS<br />
Threshold = 130 HU (102.7 mg/cm 3 CaHA)<br />
In total, ten calcified lesions could be<br />
detected in the CaSc. Diffuse distribution<br />
of calcified deposits was observed in<br />
the right coronary artery (RCA), the left<br />
artery descending (LAD) and the left circumflex<br />
coronary artery (CX). The total<br />
Agatston score was 130.<br />
CTA unveiled a normal coronary artery<br />
anatomy, right dominant coronary supply<br />
type with regular sized lumen of the<br />
coronary arteries. RCA and LAD showed<br />
no hemodynamic relevant lesions. CX<br />
coronary artery unveiled a stenosis<br />
smaller than 50% in its proximal segment.<br />
A deep myocardial bridging of the<br />
LAD could also be depicted.<br />
38 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
COMMENTS<br />
In combination with the CaSc (0.35 mSv)<br />
and the CTA (0.8 mSv), an effective<br />
dose* of 1.1 mSv was applied to the<br />
patient to detect coronary artery disease.<br />
The entire acquisition time of the CTA<br />
was 280 ms; calcium scoring was<br />
acquired in 120 ms.<br />
The Flash Spiral cardio method quickly<br />
and reliably combines low radiation<br />
dose values with the accurate display of<br />
the coronary arteries in all segments.<br />
Artery Numbers of Calcium Score (2) Volume [mm 3 ] (3) Equiv. Mass<br />
Lesions (1) [mg CaHA] (4)<br />
LM 0 0.0 0.00 0.0<br />
LAD 2 27.5 29.3 4.89<br />
CX 3 48.3 50.5 8.57<br />
RCA 5 53.6 66.2 10.81<br />
Total 10 129.5 146.0 24.27<br />
(1) Lesion is volume based, (2) Equivalent Agatston score, (3) Isotropic interpolated volume, (4) Calibration Factor: 0.790<br />
*Effective Dose was calculated using the published conversion factor for an adult chest of 0.014 mSv (mGy cm) -1 [1].<br />
[1] McCollough CH et al. Strategies for Reducing Radiation Dose in CT, Radiol. Clin. N. Am. 47: (2009) 27-40.
EXAMINATION PROTOCOL<br />
1<br />
Scanner <strong>SOMATOM</strong> Definition<br />
Cardio-Vascular Clinical Results<br />
Scan mode Flash Spiral CorCTA Rotation time 0.28 s<br />
Scan area Thorax Pitch 3.4<br />
Scan length 130 mm Spatial Resolution 0.33 mm<br />
Scan direction Cranio-caudal Slice collimation 128 x 0.6 mm<br />
Scan time 0.28 s Slice width 0.75 mm<br />
Heart rate 56 bpm Reconstruction increment 0.7<br />
Tube voltage 100 kV / 100 kV Reconstruction kernel B26f<br />
Tube current 320 mAs/rot. Volume 60 ml<br />
Dose modulation CARE Dose4D Flow rate 6 ml/s<br />
CTDIvol 3.10 mGy Start delay Test Bolus<br />
DLP 57 mGy cm Postprocessing syngo Circulation<br />
Effective Dose 0.8 mSv syngo InSpace<br />
1 VRT of the Coronary arteries shows deep<br />
myocardial bridging of LAD (arrow).<br />
4<br />
4 MIP of the coronary artery tree with<br />
removed blood pool of the left ventricle<br />
reveals calcifications (arrow).<br />
2<br />
2 MIP of the LAD shows myocardial bridging<br />
(arrow).<br />
5 6<br />
5 A stenosis is present in the proximal<br />
segment of CX artery (arrow).<br />
3<br />
3 MIP of the first diagonal branch (D1) of the<br />
LAD, discovers plunge into myocardium.<br />
6 Cross-sectional view displays the<br />
stenotic area of CX artery.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 39
1<br />
Clinical Results Cardio-Vascular<br />
Case 5<br />
Utilizing Ultra Low Dose<br />
of 0.05 mSv for Premature Baby<br />
With Congenital Heart Disease<br />
By Jean-Francois Paul, MD 1 and Andreas Blaha 2<br />
1 Centre Chirurgical Marie Lannelongue, Le Plessis-Robinson, France<br />
2 Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
1 CT imaging with VRT technique shows ventricular septal defect (arrows)<br />
and persistent foramen ovale (PFO, arrowheads).<br />
HISTORY<br />
A premature baby was referred to the<br />
radiology department with diagnosis of<br />
congenital heart disease. An atrial and<br />
left ventricular septum defect could be<br />
detected with echocardiography but<br />
with a doubt about the exact origin and<br />
*Effective Dose was calculated using the published conversion factor for a pediatric (newborn) chest of 0.039 mSv (mGy cm) -1 [1].<br />
To take into account that <strong>Siemens</strong> calculates the CTDI in a 32 cm CTDI phantom an additional correction factor of 2 had to be applied.<br />
[1] McCollough CH et al. Strategies for Reducing Radiation Dose in CT, Radiol. Clin. N. Am. 47: (2009) 27-40.<br />
40 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
course of right pulmonary artery (RPA).<br />
Therefore a low dose CT examination<br />
was requested, utilizing low kilovoltage<br />
(kV) and low milliampere seconds (mAs)<br />
to achieve ultra low dose radiation<br />
values.<br />
DIAGNOSIS<br />
A mild stenosis present at the ostium<br />
of the right pulmonary artery could be<br />
observed. Although the RPA showed an<br />
irregularity it had a normal anatomical<br />
course. The ventricular septum defect as<br />
well as the still open atrial septum could<br />
be clearly revealed by using oblique planar<br />
reformations. The right coronary artery<br />
was well depicted despite a heart<br />
rate of 157 bpm.<br />
COMMENTS<br />
The data acquisition was performed<br />
with a <strong>SOMATOM</strong> Definition Flash using<br />
the ECG-triggered sequential mode<br />
(Flash Cardio Sequence) which resulted<br />
in an ultra low dose value. Calculated<br />
with the dose length product (DLP) of<br />
0.7, an estimated dose of 0.05 mSv could<br />
be achieved.*<br />
Using the Definition Flash low dose acquisition<br />
technique it was possible to detect<br />
this congenital heart disease (CHD)<br />
in a very early stage of the patients life.
2 3<br />
4<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong> Definition Flash<br />
5<br />
Cardio-Vascular Clinical Results<br />
2 Ventricular<br />
septal defect in<br />
MIP technique<br />
(caudo-cranial<br />
view, arrow); PFO<br />
(arrowhead).<br />
3 Caudo-cranial<br />
view MIP shows<br />
mild stenosis and<br />
irregularity of<br />
the RPA (arrow).<br />
4 Cranio-caudal<br />
view in VRT-technique.<br />
5 Fused VRT and<br />
MIP highlighting<br />
RPA (arrow).<br />
Scan mode Flash Cardio Sequence Effective Dose 0.05 mSv<br />
Scan area Thorax Rotation time 0.28 s<br />
Scan length 33 mm Feed/Rotation one rotation<br />
Scan direction Cranio-caudal Slice collimation 128 x 0.6 mm<br />
Scan time 0.18 s Slice width 0.75 mm<br />
Tube voltage 80 kV / 80 kV Reconstruction increment 0.4 mm<br />
Tube current 22 mAs / rot. Reconstruction kernel B26f<br />
CTDIvol 0.18 mGy Postprocessing CT Cardiac Engine<br />
DLP 0.7 mGy cm<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 41
Clinical Results Cardio-Vascular<br />
Case 6<br />
<strong>SOMATOM</strong> Defi nition Flash:<br />
Pediatric Patient Without Sedation<br />
and Breath-Holding<br />
By Kaori Takada, MD* and Tomoko Fujihara**<br />
* Department of Radiology, Sakakibara Heart Institute, Tokyo, Japan<br />
**<br />
Application Department CT Team, Customer Service Division, <strong>Siemens</strong>-Asahi Medical Technologies, Tokyo, Japan<br />
HISTORY<br />
A 4-year-old boy with Tetralogy of Fallot<br />
(TOF, Fig.1), pulmonary atresia (PA)<br />
and major aorto-pulmonary collateral<br />
arteries (MAPCAs) was referred to the<br />
radiology department of Sakakibara<br />
Heart Institute for a follow-up examination<br />
using a <strong>SOMATOM</strong> Definition Flash,<br />
Dual Source CT in Flash Spiral mode<br />
following treatment of his pulmonary<br />
artery stenosis.<br />
The patient was diagnosed shortly after<br />
birth with TOF, PA, MAPCA. When he<br />
was 10 months old, a stent was inserted<br />
in the largest MAPCA and a central shunt<br />
was placed when he was 16 months old.<br />
When he was 2 years old, he underwent<br />
right and left modified Blalock-Taussig<br />
1<br />
1 Ventricular septal defect that is one<br />
characteristic of TOF.<br />
shunt surgeries (therefore the subclavian<br />
artery is connected with the pulmonary<br />
artery) within 9 months. Then, at<br />
the age of 3, an artificial vessel was constructed<br />
from the right ventricle (RV)<br />
to the pulmonary artery by palliative<br />
Rastelli procedure.<br />
The patient now underwent a percutanous<br />
transluminal angioplasty (PTA)<br />
of pulmonary artery. A low dose, Dual<br />
Source CT scan in the Flash Spiral mode<br />
was ordered to confirm his postoperative<br />
condition, in particular concerning<br />
the pulmonary circulation. The patient’s<br />
weight was 15.6 kg (34.39 lb).<br />
He was not sedated and no breath-hold<br />
was needed during the scan. His mean<br />
heart rate was 95 bpm.<br />
DIAGNOSIS<br />
The Dual Source CT images showed that<br />
the RV-pulmonary artery conduit was<br />
patent and that the anastomosis site<br />
had no stenosis. Neither the right nor<br />
the left pulmonary arteries (about<br />
4 mm diameter) presented any significant<br />
stenosis (Fig. 2).<br />
A stent was confirmed in the biggest<br />
MAPCA, which bifurcated from the<br />
descending aorta at the level of the left<br />
atrium. It went to the right superior and<br />
inferior lung lobes, and connected one<br />
artery originating from right central pulmonary<br />
artery. Although the stent itself<br />
was patent, a stenotic part was seen distal<br />
of the stent (Fig. 3). The Dual Source<br />
42 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
CT images revealed a tortuous artery<br />
originating from a right subclavian artery<br />
that supplied the right and left inferior<br />
lung lobes. The left lung was perfused<br />
mainly by the left central pulmonary<br />
artery. The right middle lung lobe<br />
was perfused by the large right inferior<br />
diaphragmatic artery (its distal end was<br />
connected to an artery originating from<br />
the central pulmonary artery).<br />
Incidentally, the right coronary artery<br />
(RCA) was found to originate from the<br />
aorta at the upper level of left coronary<br />
artery, the left coronary cusp (Fig. 4),<br />
which could neither be seen in the previously<br />
performed catheter angiography<br />
nor in a 16-MSCT examination.<br />
Based on these findings a catheter PTA<br />
of the pulmonary artery stenosis at the<br />
distal part of the stent was planned.<br />
COMMENTS<br />
Dual Source CT Angiography has<br />
emerged as an essential diagnostic tool<br />
for the assessment of complex congenital<br />
heart disease. Nevertheless, dose has<br />
remained a concern, in particular when<br />
referring pediatric patients for cardiac<br />
CT. With the Flash Spiral mode of the<br />
second generation Dual Source CT,<br />
pediatric patients can be scanned at<br />
ultra low dose, as in this case at 1.63<br />
mGy (effective dose 0.644 mSv). Apart<br />
from dose concerns, additional challenges<br />
have been associated with imaging<br />
pediatric congenital heart disease
patients: the patients have high heart<br />
rates, the cardiac vessels are tiny, sedation<br />
often presents a risk and most patients<br />
cannot hold their breath. This<br />
Dual Source CT Flash scan of 211 mm<br />
2A 3A<br />
2B 3B<br />
4A<br />
4B<br />
2 Both, right and left pulmonary arteries (about 4 mm diameter)<br />
had now significant stenosis.<br />
4 RCA originated from left coronary cusp (arrows).<br />
length was taken in only 0.51 seconds<br />
without sedation or breath-hold. Vessels<br />
were clearly visualized without artifacts.<br />
Even coronary anomaly could be seen<br />
despite the patient’s high heart rate of<br />
Cardio-Vascular Clinical Results<br />
3 Stent was embedded in largest MAPCA that showed<br />
a stenosis (arrow) distal of stent (arrowhead).<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong> Definition Flash<br />
Scan mode Flash Spiral<br />
Scan area Thorax / Chest<br />
Scan length 211 mm<br />
Scan direction Cranio-caudal<br />
Scan time 0.52 s<br />
Tube voltage 80 kV<br />
Tube current 104 eff. mAs<br />
CTDIvol<br />
1.63 mGy<br />
Effective Dose 0.644 mSv<br />
Rotation time 0.28 s<br />
Pitch 3.4<br />
Slice collimation 128 x 0.6 mm<br />
Slice width 0.6 mm<br />
Reconstruction increment 0.3 mm<br />
Spatial resolution 0.33 mm<br />
Reconstruction Kernel B26f, B46f (stent)<br />
Contrast<br />
95 bpm. Pulmonary artery in-stent stenosis<br />
could also be evaluated. The Dual<br />
Source CT Flash images were extremely<br />
helpful for further treatment planning.<br />
Flow Rate 2.5 ml/s<br />
Start delay 17 s<br />
Volume 30 ml<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 43
Clinical Results Cardio-Vascular<br />
Case 7<br />
<strong>SOMATOM</strong> Defi nition Flash:<br />
Dual Energy Coronary CT Angiography<br />
for Evaluation of Chest Pain After RCA<br />
Revascularization<br />
By Ralf W. Bauer, MD, J. Matthias Kerl, MD, Thomas J. Vogl, MD<br />
Department of Diagnostic and Interventional Radiology, Clinic of the Goethe University, Frankfurt, Germany<br />
HISTORY<br />
A 54-year-old female patient underwent<br />
coronary stent percutaneous transluminal<br />
coronary angioplasty (PTCA) of<br />
the right coronary artery (RCA) four<br />
months ago for acute ST-elevation<br />
myocardial infarction of the inferioseptal<br />
wall. Now, the patient suffered from<br />
reduced physical power and labile blood<br />
1<br />
1 Prior to recanalization: Cardiac catheterization<br />
showed a prominent RV branch and<br />
in-stent occlusion of the mid and distal RCA<br />
(arrow).<br />
pressure and had an event of syncope<br />
three weeks ago. Invasive coronary angiography<br />
was performed to assess stent<br />
patency. In-stent occlusion of the mid<br />
and distal RCA with moderate collateralization<br />
from the left anterior descending<br />
(LAD) and left circumflex artery (LCX)<br />
and a patent right ventricular (RV)<br />
44 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
2<br />
2 Curved multiplanar reformates showed<br />
instent thrombosis with occlusion beginning<br />
in the proximal RCA. In the RV branch, which<br />
was clearly visible on pre-interventional cath<br />
images, no contrast material filling could be<br />
delineated (arrows).<br />
branch were found (Fig. 1). Recanalization<br />
was performed with placement of 2<br />
drug-eluting stents in the distal and mid<br />
RCA. During intervention, a small contrast<br />
material extravasation was seen<br />
near the ostium in the proximal RCA.<br />
A small intima dissection was suspected<br />
and another stent was placed to close<br />
3<br />
3 Dual Energy iodine mapping showed a<br />
large area with decreased perfusion in<br />
the arterial phase in the inferoseptal wall<br />
extending from the base to the apex of the<br />
heart (arrow).
4<br />
the leakage. Three hours after intervention,<br />
the patient developed chest tightness<br />
and retrosternal pain. ECG showed<br />
signs of the known old infarction<br />
inferiorseptally (Q waves in II, III and<br />
aVF) but no signs of acute ischemia.<br />
She was sent to CT to rule out aortic<br />
dissection.<br />
DIAGNOSIS<br />
Cardiac CT was performed in Dual Energy<br />
mode with retrospective ECG-gating.<br />
There was no sign of contrast material<br />
extravasation or aortic dissection. Dual<br />
Energy CT Angiography revealed in-stent<br />
thrombosis with occlusion of the RCA<br />
13 mm after its origin (Fig. 2). While<br />
on cardiac cath the RV branch was still<br />
open, DECT showed an occlusion of the<br />
vessel due to the thrombus in the proximal<br />
RCA, explaining the patient’s symptoms.<br />
Dual Energy myocardial iodine<br />
mapping showed a large hypoperfused<br />
4 Late enhancement was present in the inferoseptal<br />
wall corresponding to the perfusion<br />
defect in arterial phase.<br />
5<br />
area inferoseptal extending from the<br />
base down to the apex (Fig. 3). Low<br />
dose step-and-shoot late enhancement<br />
images 7 minutes after contrast injection<br />
showed corresponding delayed<br />
contrast material washout (Fig. 4). On<br />
regular anatomical multiplanar reformates,<br />
a moderate thinning of the left<br />
ventricular myocardium was present<br />
in that area (Fig. 5).<br />
COMMENTS<br />
In this case, Dual Energy coronary<br />
CT Angiography was used to image a<br />
complication of interventional recanalization,<br />
i.e. acute in-stent thrombosis,<br />
while the initial clinical diagnosis of<br />
acute aortic dissection could reliably<br />
be ruled out.<br />
A further complication was the occlusion<br />
of the RV branch (which was patent<br />
prior to intervention) due to the large<br />
thrombus formation beginning very<br />
5 Regular anatomical multiplanar reformates<br />
showed moderate thinning of the interoseptal<br />
wall consistent with chronic ischemia (arrow).<br />
Cardio-Vascular Clinical Results<br />
proximally in the RCA. The new hybrid<br />
reconstruction algorithm for coronary<br />
CTA images preserves the high temporal<br />
resolution of 75 ms of the Dual Source<br />
system and allows for motion-free imaging<br />
of the vascular structures. According<br />
to the clinical history of the patient,<br />
assessment of the myocardium with<br />
Dual Energy first-pass perfusion and<br />
late enhancement imaging showed signs<br />
of chronic infarction in the inferoseptal<br />
wall of the left ventricle. Increased tube<br />
power as well as improved separation of<br />
the spectra by using a tin filter (140 kV<br />
+ Sn filter) allowed for artifact-free imaging<br />
of myocardial perfusion. Complete<br />
diagnostic work-up of the coronary<br />
arteries and the myocardium was<br />
achieved with a total dose length product<br />
of only 294 mGy cm (227 mGy cm CTA +<br />
67 mGy cm late enhancement).<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong> Definition Flash<br />
Scan mode Dual Energy<br />
Scan area Heart<br />
Scan length 170 mm<br />
Scan direction Cranio-caudal<br />
Scan time 4.8 s<br />
Tube voltage A/B 100 kV/140 kV+Sn filter<br />
Tube current A/B 165 mAs/140 mAs<br />
CTDIvol<br />
13.29 mGy<br />
Rotation time 0.28 s<br />
Pitch 0.17<br />
Slice collimation 64 x 0.6 mm<br />
Slice width<br />
Reconstruction<br />
0.75 mm<br />
increment<br />
Reconstruction<br />
0.4 mm<br />
kernel D26f<br />
Volume 70 ml contrast media<br />
Flow rate 5 ml/s<br />
Start delay Test bolus<br />
Post processing syngo Dual Energy<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 45
Clinical Results Oncology<br />
Case 8<br />
3D Guided RF Ablation and<br />
CT Perfusion – a New Combination for<br />
Monitoring of Treatment Response<br />
By Hatem Alkadhi, MD* , ** and Jan Freund***<br />
* Institute of Diagnostic Radiology, University Hospital Zurich, Zurich, Switzerland;<br />
** Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA<br />
***<br />
Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
Today, there is a significant trend for<br />
more routine biopsies, as well as an increasing<br />
volume of more complex interventional<br />
procedures such as radio frequency<br />
(RF) ablations and minimally<br />
invasive surgical procedures. In addition,<br />
the need for large perfusion ranges is increasing<br />
with the demand for complete<br />
and comprehensive assessments of the<br />
whole disease in the entire organ. The<br />
current challenge in CT interventions is<br />
to overcome the limitations of conventional<br />
2D CT guidance where, especially<br />
in difficult cases, the safe navigation<br />
of the needle is a challenge.<br />
A more accurate overview of the needle<br />
position and surrounding organs has<br />
often been lacking during difficult pro-<br />
1<br />
1 Contrast-enhanced abdominal CT shows<br />
an exophytic mass in the left kidney (arrow).<br />
cedures, especially when using oblique<br />
needle positions in both fluoroscopic<br />
and non-fluoroscopic procedures.<br />
Strongly motivated by the increased volume<br />
of these interventions, radiologists<br />
have been looking for a solution that<br />
adds precision while reducing procedure<br />
time, freeing up the CT suite for more<br />
patients and procedures and, in addition,<br />
bringing new revenue opportunities.<br />
At University Hospital Zurich, radiologists<br />
are working on an impressive and promising<br />
solution utilizing <strong>Siemens</strong>’ realtime<br />
3D image guidance for minimally<br />
invasive procedures and CT Perfusion<br />
in combination with the innovative<br />
Adaptive 4D Spiral technology. The following<br />
case demonstrates a 3D guided<br />
2 The image shows the RFA procedure of<br />
the left kidney tumor.<br />
46 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
2<br />
RF ablation of a renal cell carcinoma<br />
with a combined monitoring of treatment<br />
response by Adaptive 4D Spiral<br />
volume perfusion CT.<br />
PATIENT HISTORY<br />
An 80-year-old female patient presented<br />
to the emergency department with macrohematuria.<br />
A CT of the abdomen<br />
revealed a mass in the left kidney that<br />
was suspicious of a renal cell carcinoma<br />
(Fig. 1). Because severe co-morbidities<br />
prevented open surgery, the patient was<br />
scheduled to undergo radio frequency<br />
ablation (RFA). Considering the large size<br />
of the tumor, embolization of the mass<br />
was performed prior to RFA (Fig. 3).<br />
3<br />
3 Selective catheter angiography of the left<br />
renal artery demonstrating the hyper-vascularized<br />
tumor of the lower pole (left). Angiography<br />
after embolization shows subtotal<br />
devascularization of the tumor (right).
4<br />
4 Blood volume map shows a largely devascularized tumor after<br />
embolization treatment, however, also a strongly perfused area<br />
in the medial, lower part of the tumor (red, yellow).<br />
DIAGNOSIS<br />
Due to the large size of the tumor, conventional<br />
CT Perfusion studies are normally<br />
unable to capture the entire tumor<br />
and therefore deliver only partial perfusion<br />
information. To circumvent this<br />
limitation, the patient was sent for a<br />
volume perfusion scan to the <strong>SOMATOM</strong><br />
Definition AS offering the Adaptive 4D<br />
Spiral scan modes. This allows CT Perfusion<br />
coverage of up to 7 cm. The Adaptive<br />
4D Spiral scan was performed one<br />
day after embolization. It showed the<br />
tumor to be largely devascularized.<br />
However, a small proportion in the medial<br />
lower part of the tumor still showed<br />
blood flow (Fig. 4).<br />
Two days later, a CT-guided RFA was performed<br />
using the Adaptive 3D Intervention<br />
Suite with its needle path planning<br />
and on-line tracking mode. Particularly<br />
the perfused tumor part as demonstrated<br />
by perfusion CT was targeted (Fig. 2).<br />
In order to safely reach the dedicated<br />
areas, a 3D visualization of axial, coronal<br />
and sagittal slices during the intervention<br />
was used. In combination with a 2-click<br />
path planning, a fast and precise needle<br />
navigation was ensured. Radiation exposure<br />
could be kept very low by applying<br />
an interventional sequence scan mode<br />
for needle navigation.<br />
A CT Perfusion study performed the<br />
day after RFA shows complete devascularization<br />
of the tumor (Fig. 5) indicating<br />
a successful treatment of the patient.<br />
With the ability to perform perfusion<br />
studies over the entire region of interest,<br />
it is now possible to assess the extent of<br />
the disease and visualize the function of<br />
potential metastases. The combination<br />
of CT Perfusion studies and CT guided<br />
RFAs allows the reading physician to<br />
more precisely assess the treatment<br />
success after RFA in a timely manner. This<br />
makes it possible to monitor devascularization<br />
of the kidney tumors only one<br />
day after RFA.<br />
COMMENTS<br />
5<br />
The increased precision of the 3D visualization<br />
especially helps to more precisely<br />
position RF needles to ensure the correct<br />
placement in the perfused tumor area.<br />
Oncology Clinical Results<br />
5 Blood volume map shows complete devascularization of the kidney<br />
tumor (purple, blue) after RF treatment.<br />
It gives a more accurate overview of the<br />
needle position and surrounding organs<br />
during difficult procedures, such as<br />
oblique needle positions of RFAs. This<br />
ensures a higher success rate of RF treatments.<br />
In addition, the automated needle<br />
guidance and tracking tool significantly<br />
helps to speed up the insertion and<br />
needle placement with a reduced patient<br />
exposure.<br />
The 3D minimal invasive suite in particular<br />
now offers the freedom to direct<br />
the entire procedure with just the touch<br />
of a button – without ever leaving the<br />
patient’s side. No ongoing, extensive<br />
communication with the technician for<br />
additional distance measurements,<br />
windowing and image adjustments is<br />
necessary. Since the user is now able<br />
to easily switch between fluoroscopic,<br />
sequential and spiral examinations<br />
without time-consuming scan protocol<br />
manipulation, the physician saves<br />
additional time reducing the overall<br />
interventional procedure time. This<br />
frees up the valuable CT suite more<br />
quickly for waiting patients and procedures.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 47
Clinical Results Oncology<br />
Case 9<br />
<strong>SOMATOM</strong> Defi nition Flash:<br />
Routine Re-staging of Oesophageal<br />
Carcinoma Utilizing IRIS Technology<br />
By Michael Lell, MD*and Andreas Blaha**<br />
*Department of Radiology and the Imaging Science Institute (ISI), University of Erlangen-Nuremberg, Erlangen, Germany<br />
**Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
HISTORY<br />
The 55-year-old male patient presented<br />
with a history of oesophageal cancer.<br />
He previously underwent combined radiochemotherapy.<br />
CT was requested for<br />
re-staging to discuss further therapy<br />
options for the patient.<br />
DIAGNOSIS<br />
A contrast enhanced CT revealed bilateral<br />
well-perfused lung, also the port catheter<br />
was well positioned in the vena cava<br />
superior. Following treatment, there was<br />
still prominent thickening of the wall<br />
of the distal oesophagus und enlarged<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong> Definition Flash<br />
lymph nodes in the mediastinum. In<br />
addition, a small pericardial effusion,<br />
most probably a side effect of radiotherapy,<br />
was visualized. There was no<br />
evidence of liver or lung metastases and<br />
there were no enlarged lymph nodes at<br />
the level of the celiac trunk. An isolated<br />
solitary cyst (Bosniak I) was located in<br />
the upper left kidney.<br />
COMMENTS<br />
Several measures to reduce dose were<br />
employed with this patient. Online tube<br />
current modulation (CARE Dose4D) and<br />
Scan mode Thorax DLP 260 mGy cm<br />
Scan area Thorax-Abdomen Effective Dose 3.9 mSv<br />
Scan length 656 mm Rotation time 0.33 s<br />
Scan direction Cranio-caudal Slice collimation 128 x 0.6 mm<br />
Scan time 21 ms Slice width 0.75 mm<br />
Tube voltage 120 kV Reconstruction increment 0.4 mm<br />
Tube current Ref.mAs 100 eff. mAs Reconstruction kernel I41<br />
Dose modulation CARE Dose4D Postprocessing syngo CT 3D<br />
48 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
iterative reconstruction in image space<br />
technology (IRIS) were utilized, which<br />
lead to a significant reduction in dose<br />
and noise as compared to conventional<br />
CT, improving image quality. This examination<br />
reliably demonstrated the<br />
possibility of acquiring excellent image<br />
quality at reduced dose levels (3.9 mSv /<br />
DLP: 260 mGy cm).
1<br />
3<br />
1 VRT and fused MPR show the extension of oesophageal<br />
wall thickening.<br />
3 Axial slice highlights wall thickening of the oesophagus<br />
(arrowhead), and pericardial effusion (arrows).<br />
2<br />
4<br />
Oncology Clinical Results<br />
2 Coronal cut demonstrates the solitary cyst (left kidney, arrow), and<br />
distal oesophageal wall thickening (arrowhead, IRIS reconstruction).<br />
4 Low and homogenous noise in the entire dataset using IRIS<br />
(coronal slice) reveals oesophageal thickening (arrows).<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 49
Clinical Results Neurology<br />
Case 10<br />
<strong>SOMATOM</strong> Defi nition AS+:<br />
CT Perfusion With Extended Coverage<br />
for Acute Ischemic Stroke<br />
By Ke Lin, MD<br />
Department of Radiology, New York University Langone Medical Center, New York, USA<br />
HISTORY<br />
A 53-year-old male with history of hypertension<br />
presented with sudden onset<br />
of expressive aphasia and weakness.<br />
The patient had experienced two similar<br />
but transient episodes in the previous<br />
1<br />
12 months. He arrived to the emergency<br />
department of NYU Langone Medical<br />
Center within 1 hour of symptom onset<br />
and was immediately evaluated for<br />
acute ischemic stroke by non-contrast<br />
50 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
head CT (NCCT), dynamic CT Perfusion<br />
(CTP) of the brain, and CT Angiography<br />
(CTA) of the cervical and intracranial<br />
arterial vasculature.<br />
1 Dynamic CT<br />
Perfusion (CTP)<br />
cerebral blood flow<br />
(CBF) map shows<br />
markedly decreased<br />
CBF to the left<br />
frontal operculum.<br />
CTP cerebral blood<br />
volume (CBV) map<br />
shows matched<br />
decreased CBV<br />
in this region<br />
indicating irreversible<br />
infarct core.<br />
A penumbra-core<br />
map generated by<br />
using thresholds of<br />
CBV ≤ 1.2 ml / 100 ml<br />
for core (red)<br />
and CBF ≤ 35 ml /<br />
100 ml / min<br />
and CBV >1.2 ml /<br />
100 ml for penumbra<br />
(yellow) shows<br />
little salvageable<br />
tissue at this level.
2<br />
DIAGNOSIS<br />
While NCCT showed only subtle blurring<br />
of the normal gray/white matter interface<br />
at the left frontal operculum, CTP<br />
with extended coverage revealed the full<br />
extent of the acute ischemia in the anterior<br />
left middle cerebral artery (MCA)<br />
territory. There was severe compromise<br />
of cerebral blood flow (CBF) to the mid<br />
and inferior left frontal lobe. At the level<br />
of the operculum (Broca’s area), there<br />
was a matched defect in low CBF and<br />
low cerebral blood volume (CBV) indicative<br />
of irreversible infarct core (Fig. 1).<br />
However, there was appreciable CBF/CBV<br />
mismatch on the other acquired slices,<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong> Definition AS+<br />
indicative of salvageable tissue at risk<br />
(Fig. 2). CTA showed embolic occlusion<br />
of the frontal opercular division of the<br />
left MCA secondary to plaque rupture<br />
at the left carotid bulb. The patient was<br />
then rapidly treated with intravenous<br />
thrombolytic therapy with mild improvement<br />
of symptoms.<br />
COMMENTS<br />
The <strong>SOMATOM</strong> Definition AS+ scanner<br />
with 128-slice configuration and Adaptive<br />
4D Spiral technology allows larger CTP<br />
coverage with a single bolus of contrast.<br />
2 The penumbra-core<br />
maps from selected slices<br />
above and below the<br />
level shown in Fig. 1:<br />
the extents of both the<br />
salvageable ischemic<br />
penumbra (yellow) and<br />
the irreversible infarct<br />
core (red) are fully depicted.<br />
Neurology Clinical Results<br />
In this case, the setting with 96 mm of<br />
z-direction coverage (and 1.5 seconds<br />
temporal resolution) covered nearly the<br />
entire supratentorial brain. syngo VPCT<br />
Neuro extracts first-pass data from the<br />
45 seconds dynamic acquisition enabling<br />
a rapid exam. The extents of both<br />
the salvageable ischemic penumbra and<br />
the irreversible infarct core were fully<br />
depicted. Rescue of ischemic penumbra<br />
is the main rationale for aggressive<br />
stroke intervention, and its identification<br />
through perfusion imaging may form the<br />
basis of patient selection for therapy in<br />
the near future.<br />
Scan mode Adaptive 4D Spiral Rotation time 0.3 s<br />
Scan area Head Slice collimation 64 x 0.6 mm<br />
Scan length 96 mm Slice width 10 mm<br />
Scan direction Caudo-cranial and cranio-caudal Reconstruction increment 5 mm<br />
Scan time 45 s Reconstruction kernel H20f<br />
Tube voltage 80 kV Contrast Volume 50 ml iodine<br />
Tube current 200 eff. mAs Flow rate 5 ml/s<br />
Dose modulation CARE Dose4D off Start delay 4 s<br />
CTDIvol 218.8 mGy Postprocessing syngo VPCT Neuro<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 51
Clinical Results Neurology<br />
Case 11<br />
Vasospasm After Subarachnoid<br />
Hemorrhage:<br />
Volume Perfusion CT Neuro<br />
By Bruno A. Policeni, MD<br />
Radiology Faculty, Neuroradiology, University of Iowa Hospitals and Clinics, Iowa City, Iowa, USA<br />
1<br />
HISTORY<br />
L R<br />
1 3D CT Angiography shows a right mid cerebral artery (MCA) bi-lobed aneurysm<br />
(arrow). No other aneurysms were found.<br />
A 36-year-old female with a history of<br />
migraine developed a sudden onset of<br />
the worst headache of her life, lost control<br />
of the entire right side of her body<br />
and fell to the floor. However she had<br />
no trauma to her head and did not lose<br />
consciousness. She was admitted to the<br />
emergency department where a head CT<br />
(Fig. 2) showed right sylvian fissure and<br />
inter-hemispheric fissure hyperdensity<br />
consistent with subarachnoid hemor-<br />
rhage. The temporal horns were mildly<br />
dilated due to early obstructing hydrocephalus<br />
and a small amount of intraventricular<br />
blood was present in the left<br />
occipital horn. A CT Angiography was<br />
performed and showed a 7 mm x 4 mm<br />
bi-lobed berry aneurysm with a narrow<br />
neck arising from the M1 segment of the<br />
right mid cerebral artery (MCA, Fig.1).<br />
The patient was transferred to the<br />
angiography suite for conventional<br />
52 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
angiography, confirming the right MCA<br />
aneurysm (Fig. 3). She underwent immediate<br />
aneurysm coil embolization. On<br />
day four after the intervention, her neurologic<br />
exam attested deterioration and<br />
she showed a left facial palsy, indicating<br />
suspected vasospasm. The patient was<br />
referred to the radiology department for<br />
comprehensive stroke imaging, including<br />
CT Angiography and Volume Perfusion<br />
CT (VPCT) of the brain to rule out<br />
vasospasm.<br />
DIAGNOSIS<br />
Using the Adaptive 4D Spiral technology<br />
a 9.6 cm volume perfusion scan covering<br />
the entire brain was performed and<br />
the resulting perfusion parameter maps<br />
were qualitatively and quantitatively<br />
evaluated in 3D. They demonstrated an<br />
impaired brain perfusion in the right<br />
MCA and ACA vascular territory distribution<br />
with prolonged Mean Transit Time<br />
(MTT), reduced Cerebral Blood Flow<br />
(CBF) in the same area and slightly<br />
increased Cerebral Blood Volume (CBV,<br />
Fig. 4). CT Angiography images were obtained<br />
from the dynamic VPCT data and<br />
showed areas of narrowing in the right<br />
MCA and anterior cerebral artery (ACA,<br />
Fig. 6). The following angiography confirmed<br />
the vasospasm findings consis-
2 3<br />
4<br />
Neurology Clinical Results<br />
2 Head CT without contrast<br />
demonstrates right sylvian<br />
fissure and interhemispheric<br />
fissure hyperdensity consistent<br />
with subarachnoid hemorrhage<br />
(arrows). The temporal<br />
horns are mildly dilated<br />
due to early obstructing<br />
hydrocephalus (arrowhead).<br />
3 Conventional angiography<br />
demonstrates the right MCA<br />
aneurysm in the right internal<br />
carotid artery injection (arrow).<br />
4 VPCT axial multi-parameter view showing a Maximum Intensity Projection (MIP), Cerebral Blood Flow (CBF), Cerebral Blood Volume (CBV), Time To Peak,<br />
Time To Drain (TTD) and Mean Transit Time (MTT), MTT and TTD (time to drain, a <strong>Siemens</strong> origin parameter) being the most useful parameters in this case.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 53
Clinical Results Neurology<br />
5<br />
5 3D view of the Time To Drain (TTD) parameter map of the entire brain. Time to drain is a <strong>Siemens</strong> unique deconvolution based parameter describing<br />
the time of the earliest washout of contrast medium in seconds. It is a very sensitve parameter to detect perfusion asymetries like MTT.<br />
tent with segmental narrowing in the<br />
right MCA/ACA and delayed capillary<br />
transit time (Fig. 7A). The patient was<br />
immediately treated with 8 mg intraarterial<br />
nicardipine for a period of 10<br />
minutes and balloon angioplasty was<br />
performed in the right MCA. Immediate<br />
follow-up confirmed a successful treatment<br />
(Fig. 7B) and there was also an improvement<br />
in the neurologic exam,<br />
specifically in the left facial palsy. The<br />
patient was discharged on day 17, neurologically<br />
stable with resolution of the<br />
facial droop, well-controlled pain and<br />
ambulating without assistance. She was<br />
scheduled for a follow-up exam in the<br />
clinic 6 weeks later.<br />
COMMENTS<br />
syngo VPCT Neuro offers dynamic perfusion<br />
analysis of the entire brain. That,<br />
as in this case, enables the detection of<br />
vasospasms – even those located in<br />
upper brain regions or in the posterior<br />
fossa, not covered by traditional Perfu-<br />
54 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
sion CT through the base of skull. Thus<br />
syngo VPCT Neuro in combination with<br />
the Adaptive 4D Spiral technology is enhancing<br />
the diagnostic application. The<br />
ability to obtain a CT Angiography with<br />
the same data acquisition is crucial for<br />
the correlation to the vascular territory<br />
showing prolonged MTT. Temporal parameter<br />
maps like MTT in 2D and 3D<br />
delivered by syngo VPCT Neuro may act<br />
as a sensible tool to detect perfusion<br />
asymmetries in the two hemispheres as<br />
an indicator for vasospasm.
6<br />
7A 7B<br />
6 Coronal CTA MIP reconstruction from<br />
the dynamic series demonstrates areas<br />
of severe vasospasm (arrows) in the right<br />
ICA and MCA compared to the normal left<br />
MCA (arrowhead).<br />
Neurology Clinical Results<br />
7 Conventional angiography confirmed severe vasospasm (arrows): segmental narrowing in the right MCA/ACA and a delayed capillary transit<br />
time (Fig. 7A). Follow up demonstrates resolution of the vasospasm after nicardipine injection and balloon angioplasty (Fig. 7B, arrows).<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong> Definition AS+<br />
Scan mode Adaptive 4D Spiral (spiral shuttle mode) Rotation time 0.3 s<br />
Scan area Head Slice collimation 128 x 0.6 mm<br />
Scan length 96 mm Slice width 5 mm for perfusion, 1 mm for CTA<br />
Scan direction Cranio-caudal and caudo-cranial Reconstruction kernel H20f<br />
Scan time 45 s; 30 scans total Volume 40 cc Isovue-370 and 50 cc normal saline<br />
Tube voltage 80 kV Flow rate 8 ml/s<br />
Tube current 200 mAs Start delay No delay<br />
CTDIvol 218 mGy Post processing syngo Volume Perfusion CT Neuro<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 55
Clinical Results Acute Care<br />
Case 12<br />
Dual Energy Scanning:<br />
Diagnosis of Ruptured Cocaine Capsule<br />
By Ralf W. Bauer, MD, J. Matthias Kerl, MD, Thomas J. Vogl, MD, Philipp Weisser, MD<br />
Department of Diagnostic and Interventional Radiology, Clinic of the Goethe University, Frankfurt, Germany<br />
HISTORY<br />
A 32-year-old male passenger on a flight<br />
from South America landed at Rhein-<br />
Main International Airport in Frankfurt.<br />
He showed a conspicuous and slightly<br />
delirious behavior. The customs and<br />
border police were alert and questioned<br />
him whether he was carrying or had<br />
consumed drugs. At first, he denied, but<br />
as his medical condition dramatically<br />
worsened, he admitted that he had<br />
swallowed 24 self-packed capsules with<br />
columbian cocaine. The patient developed<br />
heavy attacks of abdominal cramps<br />
and became more and more apathetic.<br />
He was transferred to the hospital to localize<br />
the capsules, to confirm the number,<br />
and to check, if one of the capsules<br />
had opened and cocaine had come into<br />
the bowel lumen – or if the capsules<br />
had caused an ileus.<br />
EXAMINATION PROTOCOL<br />
DIAGNOSIS<br />
Scanner <strong>SOMATOM</strong> Definition Flash<br />
A contrast-enhanced, Dual Energy CT<br />
(DECT) scan of the abdomen was performed.<br />
24 capsules with an average<br />
size of 2.5 x 3.5 cm and hyperdense<br />
content were found, confirming the<br />
patient’s story. Average CT values of the<br />
hyperdense content were 203 HU at<br />
80 kV and 140 HU at 140 kV. The capsules<br />
were spread all through the small<br />
bowel and colon. However, there was<br />
one capsule in the rectum, that was significantly<br />
larger than the others and its<br />
content showed lower attenuation values<br />
of 139 HU at 80 kV and 77 HU at<br />
140 kV. DECT further revealed a thin hyperdense<br />
layer-like structure that peeled<br />
off from that capsule, therefore the suspicion<br />
arose that the capsule actually<br />
had ruptured. Rectoscopy was performed<br />
immediately and the torn cap-<br />
56 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
sule was secured. The patient recovered<br />
on the intensive care unit without further<br />
major medical treatment and could<br />
be relieved from the rest of his freight<br />
with the use of laxatives.<br />
COMMENTS<br />
With the use of DECT, a reliable diagnosis<br />
of the ruptured cocaine capsule could<br />
be performed and immediate medical<br />
help provided. To our knowledge this<br />
is the first report on the Dual Energy<br />
behaviour of columbian cocaine. This<br />
might be of future relevance for in vivo<br />
differentiation of cocaine or heroin of<br />
different origin in uncommunicative<br />
body packers. However, further research<br />
in this field is needed to confirm our<br />
results.<br />
Scan mode Dual Energy Rotation time 0.5 s<br />
Scan area Abdomen Pitch 0.55<br />
Scan length 464 mm Slice collimation 14 x 1.2 mm<br />
Scan direction Cranio-caudal Slice width 1.5 mm<br />
Scan time 24 s Reconstruction increment 1.0 mm<br />
Tube voltage A/B 140 kV / 80 kV Reconstruction kernel D30f<br />
Tube current A/B 49 eff. mAs / 212 eff. mAs Contrast Volume 90 ml<br />
Dose modulation CARE Dose4D Flow rate 3 ml/s<br />
CTDIvol 9.14 mGy Postprocessing syngo Dual Energy
1<br />
3<br />
5<br />
1 Cocaine capsules distributed throughout the whole intestine.<br />
3 Color-coding of cocaine capsules facilitates detection and<br />
counting.<br />
5 ROI measurements demonstrate typical Dual Energy values of<br />
columbian cocaine.<br />
2<br />
4<br />
6<br />
2 Virtual colonoscopy view.<br />
Neuroradiology Clinical Results<br />
4 Ruptured cocaine capsule. Arrows point at the loose outer layer.<br />
6 The coronal reformate shows large amounts of fluid in the<br />
colon lumen. However, no ileus was present.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 57
Clinical Results Acute Care<br />
Case 13<br />
Progressive Kidney Hematoma<br />
Post-interventional Biopsy<br />
By Sebastian Leschka, MD * and Andreas Blaha **<br />
*Institute of Diagnostic Radiology, University Hospital Zurich, Zurich, Switzerland<br />
**Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
HISTORY<br />
To determine further therapy, the 21year-old<br />
patient, status after hepatitis B,<br />
was referred to the radiology department.<br />
Here a biopsy of the renal parenchyma<br />
was performed upon which a<br />
haemorrhage occurred, accompanied by<br />
the formation of a hematoma. A 3-phase<br />
kidney CT was performed. Due to the<br />
nephritic syndrome only 60 ml of contrast<br />
media with a flow rate of 4 ml/s<br />
followed by a 60 ml NaCl bolus (4 ml/s)<br />
was injected for the kidney CTA.<br />
1<br />
DIAGNOSIS<br />
In the native phase, an accumulation of<br />
liquid at the lower left renal pole was<br />
seen. The arterial phase showed an<br />
extravasation of contrast media out of<br />
the left kidney. An inhomogeneous<br />
hematoma measuring 15 x 7.5 x 5 cm<br />
was detected around the left kidney.<br />
Both kidneys were perfused symmetrically,<br />
unique renal arteries were seen<br />
bilaterally. In the venous phase a normal<br />
renal calyx developed on both sides.<br />
COMMENTS<br />
Despite the low quantity of applied contrast<br />
media, a contrast media enhancement<br />
in the left kidney could be identified<br />
due to a quick acquisition time of<br />
0.7 seconds. The <strong>SOMATOM</strong> Definition<br />
Flash allowed a precise and rapid<br />
diagnosis with a reduced given patient<br />
radiation dose of 3.3 mSv.<br />
1 Fused VRT/MPR<br />
highlight kidney<br />
hematoma.
EXAMINATION PROTOCOL<br />
2A<br />
Scanner <strong>SOMATOM</strong> Definition Flash<br />
Acute Care Clinical Results<br />
Scan mode 3-phase kidney Rotation time 0.28 s<br />
Scan area Abdomen Pitch 2.1<br />
Scan length 218 mm Slice collimation 128 x 0.6 mm<br />
Scan direction Cranio-caudal Slice width 2 mm<br />
Scan time 0.7 s Reconstruction increment 1 mm<br />
Tube voltage 120 kV / 120 kV Reconstruction kernel B30f<br />
Tube current 100 eff. mAs Contrast Volume 60 ml Iodine<br />
Dose modulation CARE Dose4D Flow rate 4 ml/s<br />
CTDIvol 7.71 mGy Postprocessing syngo CT 3D<br />
syngo InSpace<br />
2 Axial non-enhancement multiplanar reformation (MPR, Fig. 2A); axial early enhancement MPR shows haemorrhages in the<br />
kidney hematoma (arrow, Fig. 2B). Axial late state MPR shows persistent bleeding (arrow, Fig. 2C).<br />
3A<br />
2B<br />
3B<br />
3 Sagittal non-enhancement MPR (Fig. 3A); sagittal early enhancement MPR shows hemorrhages in the kidney hematoma<br />
(arrow, Fig. 3B); sagittal late state MPR shows persistent bleeding (arrow, Fig. 3C).<br />
2C<br />
3C<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 59
Clinical Results Acute Care<br />
Case 14<br />
<strong>SOMATOM</strong> Defi nition Dual Source<br />
High Pitch vs. Routine Pitch Scanning in<br />
a Pediatric Lung Low Dose Examination<br />
By Harald Seifarth, MD,* Walter Heindel, MD,* Andreas Blaha **<br />
*Department of Clinical Radiology, University Hospital, Münster, Germany<br />
**Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
HISTORY<br />
A 5-year-old male patient with a history<br />
of neutropenia after stem-cell transplantation<br />
was referred to the radiology<br />
department. The patient presented with<br />
persistent fever despite ongoing treatment<br />
with antibiotics. A CT examination<br />
was scheduled to exclude the presence of<br />
pulmonary mycosis. The CT examination<br />
was performed with a high pitch protocol<br />
(pitch = 3.0), resulting in a scan time<br />
of only 0.9 seconds.<br />
DIAGNOSIS<br />
The present CT examination showed no<br />
signs of any fungal pulmonary infection<br />
or other inflammatory changes. Minor<br />
bilateral, subpleural dystelectases could<br />
be observed.<br />
In the previous examination (pitch 1.4,<br />
scan time 4.5 seconds, scan length<br />
189 mm, 50 ref mAs), artifacts due to<br />
respiratory motion during the acquisition<br />
hampered the evaluability of the<br />
exam. The study showed small pulmonary<br />
infiltrates.<br />
60 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
1 2<br />
1 High pitch scan – axial slice of high pitch<br />
acquisition, no motion artifacts (arrow)<br />
due to breathing.<br />
3<br />
3 High pitch scan – entire lung in low<br />
dose technique (10 eff. mAs), no motion<br />
artifacts are visible.<br />
2 Regular scan – axial slice<br />
of high resolution regular scan.<br />
4<br />
4 Regulars scan – artifacts due<br />
to respiratory motion (arrows).
Acute Care Clinical Results<br />
5 6 COMMENTS<br />
Because of motion, the previous CT<br />
scan made diagnosis more difficult<br />
(Figs. 2, 4, 6). The fast acquisition<br />
speed made it possible to reliably<br />
rule out the presence of pulmonary<br />
infiltrations and mycosis. Although<br />
only 10 mAs were utilized, a high<br />
diagnostic image quality was preserved.<br />
Using the new high pitch<br />
scanning technique a significant reduction<br />
of radiation dose is feasible.<br />
7<br />
5 High pitch scan – sharp delineation<br />
of pulmonary segments.<br />
6 Regular scan – sagittal image shows<br />
motion artifact of the diaphragm due to<br />
breathing during the acquisition.<br />
7 Volume rendered image of the thorax, showing regular bronchial tree.<br />
*Effective Dose was calculated using the published conversion factor for an 5-year-old pediatric chest of 0.082 mSv (mGy cm) -1 [1].<br />
To take into account that <strong>Siemens</strong> calculates the CTDI in a 32 cm CTDI phantom an additional correction factor of 2 had to be applied.<br />
[1] McCollough CH et al. Strategies for Reducing Radiation Dose in CT, Radiol. Clin. N. Am. 47: (2009) 27-40.<br />
EXAMINATION PROTOCOL<br />
Scanner <strong>SOMATOM</strong><br />
Definition<br />
Scan mode Thorax HiPitch<br />
Scan area Thorax<br />
Scan length 159 mm<br />
Scan direction Cranio-caudal<br />
Scan time < 1s<br />
Tube voltage A/B 120 kV / 120 kV<br />
Tube current A/B 10 eff. mAs<br />
Dose modulation CARE Dose4D<br />
CTDIvol<br />
0.56 mGy<br />
DLP 9 mGy cm<br />
Effective Dose 0.37 mSv*<br />
Rotation time 0.33 s<br />
Pitch 3.0<br />
Slice collimation 64 x 0.6 mm<br />
Slice width<br />
Reconstruction<br />
1.0 mm<br />
increment<br />
Reconstruction<br />
0.5 mm<br />
kernel B60f<br />
Postprocessing syngo CT 3D<br />
syngo InSpace<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 61
Science<br />
CT in Pediatrics: Easier<br />
and Safer With the Flash<br />
The <strong>SOMATOM</strong> Defi nition Flash allows even squirming infants and small<br />
children to be scanned with maximum image quality at lightning speed,<br />
without movement artifacts, anesthesia, or ventilation. This makes<br />
computed tomography increasingly interesting for pediatric diagnostics,<br />
solely in the event of clear indications.<br />
By Hildegard Kaulen, PhD<br />
Being able to “freeze” movements in<br />
order to scan small children without sedation<br />
is every radiologist’s dream. Anesthesia<br />
transforms what would be a comparatively<br />
fast scan into a time-consuming,<br />
possibly risky affair. Therefore, Michael<br />
Lell, MD, Assistant Professor at the University<br />
Hospital in Erlangen, is extremely<br />
satisfied with the various pediatric<br />
options offered by the new <strong>SOMATOM</strong><br />
Definition Flash. As small patients are<br />
moved through the tube at a speed of<br />
almost half a meter per second, they no<br />
longer have to hold their breath or lie<br />
still for protracted periods. Sedation is<br />
no longer necessary either, and, as a<br />
result, the entire imaging process is reduced<br />
to a few minutes. Lell has been<br />
working with the Flash for 16 months.<br />
During this period, he has successfully<br />
scanned 50 infants and toddlers, and<br />
the same number of children and adolescents,<br />
without sedation or anesthesia.<br />
His experience with the Flash in<br />
the field of pediatric diagnostics is outstanding.<br />
Says Lell: “The image quality<br />
1A 1B<br />
1 Thorax CT scan for lung investigation of a 15-month-old child with cystic fibrosis with a 10-slice CT (Fig. 1A)<br />
and for follow-up 12 months later with the <strong>SOMATOM</strong> Definition Flash (Fig. 1B) showing artifact-free lung tissue.<br />
62 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
attained without sedation impresses us<br />
time and again. This is particularly striking<br />
during a direct comparison between<br />
the Flash and another CT. We examined<br />
a 15-month-old child with Down’s syndrome<br />
and cystic fibrosis using a 10-row<br />
CT. The images contained movement<br />
artifacts despite sedation. We examined<br />
the child once more at 27 months, this<br />
time using the Flash. The results? Razorsharp<br />
images without sedation (Fig.1).<br />
One child even attempted to sit up during<br />
the scan. Everyone was convinced
that the images would be blurred, but<br />
this wasn’t the case.”<br />
Young patients are usually examined<br />
using ultrasound or MRI devices. Children<br />
undergoing an MRI must be sedated.<br />
Lell comments: “Anesthesia and ventilation<br />
necessitate considerable time and<br />
effort. We are dependent on assistance<br />
from other specialist disciplines. The anesthetic<br />
must be induced, controlled and<br />
reversed by an anesthetist, and the children<br />
have to be monitored for several<br />
hours afterward. Whereas scanning time<br />
is relatively short, outpatient care is necessary<br />
for hours.” Medical treatment,<br />
care and logistics result in substantial<br />
costs, and the associated risks can also<br />
be considerable. Anesthesia is an invasive<br />
procedure. Complications may arise<br />
at any time. Says Lell: “Ventilation also<br />
leads to anesthesia-related pulmonary<br />
atelectasis, a condition which causes<br />
parts of the lungs to collapse, impeding<br />
gas exchange. It is difficult to assess these<br />
areas accurately during imaging. This issue<br />
becomes irrelevant if anesthesia and<br />
Indications for<br />
Pediatric CT Scans:<br />
�� Polytrauma<br />
�� Congenital heart disease<br />
�� Serious lung diseases such<br />
as cystic fibrosis or atypical<br />
pneumonias<br />
� Tumor staging<br />
Benefits of Flash CT<br />
in Pediatrics:<br />
� Images free of movement artifacts,<br />
even in the case of<br />
squirming children<br />
� No sedation or deep general<br />
anesthesia<br />
� Imaging possible without assistance<br />
from other disciplines<br />
such as anesthesia or nursing<br />
� No outpatient care or aftercare<br />
� No complications as a result<br />
of anesthesia<br />
ventilation are not used. If it’s a choice<br />
between performing CT with anesthesia<br />
or not, then the answer in the case of<br />
the Flash is a definite no.”<br />
Setting New Standards<br />
The <strong>SOMATOM</strong> Definition Flash is able<br />
to freeze movements due to its unique<br />
speed. Scanning speeds of up to 45.8 cm<br />
per second with a temporal resolution<br />
of 75 ms ensure that complete chest<br />
scans of young patients can be recorded<br />
in 0.4 to 0.5 seconds. No other device<br />
is as fast. The Flash also sets new standards<br />
when it comes to radiation exposure.<br />
The Adaptive Dose Shield reduces<br />
radiation exposure in every single spiral<br />
scan. But the most impressive dose reduction<br />
is possible in the field of cardiology<br />
where ultrafast Flash Spiral cuts<br />
down radiation compared to conventional<br />
ECG-gated examinations by up to 90 %.<br />
Lell believes that the Flash will make CT<br />
scans an increasingly attractive option<br />
for younger patients. The radiologist<br />
considers indications to be the decisive<br />
factor. In pediatrics, a CT would only be<br />
considered in the event of medical indications<br />
with few or no alternatives, such<br />
as polytrauma or tumor staging. In the<br />
case of multiple injuries, it is more important<br />
to clarify the extent of the trauma<br />
suffered than to contemplate a statistical<br />
increase in cancer risk in the distant<br />
future. Says Lell: “Some indications necessitate<br />
a CT examination, even if we are<br />
aware of the effective dose. We don’t<br />
know exactly how this dose may affect<br />
the cancer risk in any case as no longterm<br />
data is available based on medical<br />
imaging exposure levels.” Lell already<br />
insists on reduced dose protocols. He<br />
and his team have developed protocols<br />
like these for all pediatric indications. In<br />
Erlangen, children are always scanned<br />
with a tube voltage of 80 or 100 kV.<br />
Special anatomy adapted cushions are<br />
used to fix the small patients during the<br />
examination. Contrast agents are used<br />
very sparingly. Lell also ensures that the<br />
examination area is kept to a minimum,<br />
and strives to achieve the attention to<br />
detail necessary for diagnosis.<br />
Science<br />
Assistant Professor Michael Lell,<br />
MD, completed his medical studies<br />
at the universities of Regensburg and<br />
Munich with subsequent qualification<br />
as a consultant in radiology and<br />
habilitation. Employed by the University<br />
Hospital in Erlangen since 1999.<br />
Promoted to Chief Physician in 2009.<br />
One-year residency at the David<br />
Steffen School of Medicine at UCLA.<br />
Member of national and international<br />
professional associations; reviewer<br />
for various journals.<br />
Hildegard Kaulen, PhD, is a molecular biologist.<br />
After stints at the Rockefeller University in<br />
New York and the Harvard Medical School in<br />
Boston, she moved to the field of freelance<br />
science journalism in the mid-1990s and contributes<br />
to numerous reputable daily newspapers<br />
and scientific journals.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 63
Science<br />
Through the use of a <strong>SOMATOM</strong> Emotion 6 from <strong>Siemens</strong> <strong>Healthcare</strong>, an international research team discovered<br />
atherosclerosis in 3500 year old Egyptian mummies.<br />
Study Finds Atherosclerosis in<br />
3,500 Year old Egyptian Mummies<br />
By Steven Bell, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
A team of cardiologists led by Drs.<br />
Gregory S. Thomas of the University of<br />
California, Irvine and Adel H. Allam of<br />
Al Azhar University, Cairo, found that<br />
atherosclerosis is not only a disease<br />
of modern man, but was present in<br />
humans as far back as 1,530 BC.<br />
The team of cardiologists working<br />
closely with a team of Egyptologists<br />
undertook the most comprehensive CT<br />
study of vascular disease in Egyptian<br />
mummies to date by scanning 22 mummies<br />
over a four-day period in the Cairo<br />
Museum of Antiquities. The study was<br />
co-sponsored by <strong>Siemens</strong> <strong>Healthcare</strong> and<br />
aimed to investigate whether atherosclerosis,<br />
the precursor of heart disease, is an<br />
affliction of modern man or whether this<br />
disease existed thousands of years ago.<br />
The imaging for this project was undertaken<br />
on a <strong>SOMATOM</strong> Emotion 6-slice<br />
configuration that was donated to the<br />
Museum as part of an earlier study in<br />
conjunction with National Geographic<br />
to image the famous mummified remains<br />
of King Tutankhamun.<br />
The researchers were able to locate and<br />
identify vascular tissue in 16 out of the<br />
22 mummies imaged in this study. Of<br />
these 16, 9 had visible signs of arterial<br />
calcification, considered to be pathognomonic<br />
of atherosclerosis, from which the<br />
researchers were able to conclude that<br />
atherosclerosis is not a disease exclusive<br />
to modern humans. Findings of calcification<br />
were made in men and women who<br />
lived between 1570 BC and 364 AD. The<br />
social status of most patients included in<br />
64 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
the study was shown to be of an elevated<br />
nature, which may have contributed<br />
to the process of disease due to lifestyle<br />
issues. The main aim of this project was<br />
to identify the presence or absence of<br />
atherosclerosis in an ancient patient<br />
population, however, the study also<br />
offered prominent Egyptologists the<br />
opportunity to view the mummified<br />
remains of these patients in a way that<br />
was not damaging to these ancient<br />
artifacts, the protection of which is<br />
central to the thinking of all members<br />
of this research study.<br />
The results of this project were published<br />
in the November 18, 2009 edition<br />
of the JAMA and also presented at the<br />
November AHA Meeting in Orlando,<br />
Florida, USA.
Independent Validation of<br />
Perfusion Evaluation Software<br />
By Katharina Otani, PhD and Toshihide Itoh<br />
Research Collaboration Development, <strong>Siemens</strong> Asahi Medical Technologies, Tokyo, Japan<br />
A study by an independent Japanese<br />
research group reported that <strong>Siemens</strong> CT<br />
Perfusion software syngo VPCT Neuro,<br />
using the maximum slope model to derive<br />
cerebral blood flow (CBF), delivered<br />
among the most accurate results in the<br />
assessment of stroke infarct size compared<br />
to other commercial software. 1<br />
Kohsuke Kudo, MD, PhD, from Iwate<br />
Medical University and his colleagues<br />
from five other universities in Japan used<br />
data of 10 stroke patients acquired with a<br />
four-detector-row scanner and applied<br />
different algorithms to generate CT Perfusion<br />
maps, in particular CBF, cerebral<br />
blood volume (CBV) and mean transit<br />
time (MTT) or time to peak (TTP) maps:<br />
A – singular-value decomposition (SVD,<br />
CT Perfusion 3, GE <strong>Healthcare</strong>)<br />
B – inverse filter IF (Version 2.0, Hitachi<br />
Medical Systems)<br />
C – singular-value decomposition (SVD,<br />
Version 1.201, Philips <strong>Healthcare</strong>)<br />
D – maximum slope (MS, VA70A,<br />
<strong>Siemens</strong> <strong>Healthcare</strong>)<br />
E – box modular transfer function (bMTF,<br />
Ph 7, Toshiba Medical Systems).<br />
Kudo compared the perfusion maps with<br />
the results from free software (Perfusion<br />
Mismatch Analyzer, PMA) distributed<br />
by the Acute Stroke Imaging Standardization<br />
Group (ASIST) Japan that applies<br />
two well-documented deconvolution<br />
algorithms: standard singular-value decomposition<br />
(sSVD) and block-circulant<br />
singular-value decomposition (bSVD).<br />
sSVD and bSVD algorithms differ with respect<br />
to their sensitivity to contrast tracer<br />
delay effects. bSVD is considered the<br />
“gold standard” since it is relatively insensitive<br />
to tracer delay.<br />
Kudo found that commercial software<br />
could be classified in two groups: those<br />
giving similar results to the CBF maps<br />
obtained with sSVD (A, C, E) and those<br />
giving similar results to the CBF maps<br />
obtained with bSVD (B, D). Abnormal<br />
MTT/TTP areas appeared larger than<br />
those in bSVD for maps of all commercial<br />
software (A, C, D, E) except for one vendor’s<br />
software (B). An editorial in the<br />
same journal issue commented: 2 “The<br />
results of the study by Kudo et al. 1 also<br />
support the use of the maximum slope<br />
method for CT perfusion post-processing.<br />
Indeed, a recent MR imaging study 3 of<br />
“True multi-center<br />
trials on stroke<br />
assessment by CT<br />
Perfusion and optimization<br />
of patient<br />
management will<br />
only be possible<br />
once every vendor’s<br />
software delivers<br />
the same<br />
perfusion maps.”<br />
Kohsuke Kudo, MD, PhD, Iwate Medical<br />
University<br />
Science<br />
acute stroke patients reported higher positive<br />
predictive values for infarction by<br />
using maximum slope-derived parameters<br />
(first moment, TTP), versus both delaysensitive<br />
and delay-insensitive deconvolution-derived<br />
parameters. These results<br />
highlight the delay-insensitive nature of<br />
perfusion maps derived from maximumslope<br />
algorithms. At present, however,<br />
there remains insufficient evidence to suggest<br />
whether maximum-slope methods<br />
outperform delay-insensitive deconvolution<br />
algorithms.” Kudo started working on<br />
standardization of perfusion software<br />
after he programmed his own software<br />
and discovered that his results differed not<br />
only from the results of one commercial<br />
software but that the results from all software<br />
packages also differed from each<br />
other. With Makoto Sasaki, MD, he set up<br />
ASIST Japan supported by a grant from the<br />
Japanese governement. ASIST Japan has<br />
introduced a color look-up table for perfusion<br />
maps. Kudo emphasizes that “true<br />
multicenter trials on stroke assessment by<br />
CT Perfusion and optimization of patient<br />
management will only be possible once<br />
every vendor’s software delivers the same<br />
perfusion maps”.<br />
In his study, Kudo used earlier perfusion<br />
software versions such as <strong>Siemens</strong> “Neuro<br />
PCT”. In the meantime however, <strong>Siemens</strong><br />
has developed “syngo VPCT Neuro”, a volume<br />
perfusion software that gives the option<br />
to also apply a new tracer delay insensitive<br />
deconvolution algorithm in addition<br />
to the as well delay insensitive maximum<br />
slope model used in this study. Kudo is<br />
currently working on further multi-vendor<br />
comparison studies.<br />
1 Kudo K, et al . Radiology. 2010 Jan; 254(1):200-9<br />
2 Konstas A A, et al. Radiology, 2010; 254(1):22-25<br />
3 Christensen S, et al. Stroke 2009, 40 : 2055 – 2061<br />
http://asist.umin.jp/index-e.htm<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · Mai 2010 · www.siemens.com/healthcare-magazine 65
Science<br />
Reduced Procedure Time<br />
and Radiation Dose in Inter-<br />
ventional CT Workflow<br />
By Prof. A.H. Mahnken, MD and F. Schoth, MD<br />
RWTH Aachen University Hospital, Aachen, Germany<br />
Percutaneous lung biopsy is one of the<br />
most common CT-guided procedures.<br />
This technique can be performed using<br />
sequential CT-scanning or CT-fluoroscopy.<br />
Because CT-fluoroscopy may result in<br />
significant radiation exposure to the<br />
patient as well as the interventionalist,<br />
repeated sequential CT-scanning is common<br />
practice due to the minimal radiation<br />
exposure to the operating physician.<br />
However, this approach requires several<br />
breath holds, with the target lesion mov-<br />
ing during in- and expiration. For many<br />
patients, it is virtually impossible to repeatedly<br />
come back to the same breath<br />
hold position. Therefore, small lesions<br />
in particular, will often move out of<br />
plane. This problem is particularly pronounced<br />
in the basal sections of the<br />
lung and is a major issue when dealing<br />
with small lesions of 1 cm or less.<br />
Combining CT-guided procedures with<br />
the Interactive Breath-Hold Control<br />
device (IBC) has been shown to increase<br />
1A 1B<br />
45 15<br />
30<br />
66 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
the radiologists’ accuracy and confidence<br />
with needle biopsy of the lung. A simple<br />
light display allows the patients to monitor<br />
their breathing level and consistently<br />
return to their reference breath-hold<br />
position during their biopsies. The IBC<br />
was developed to assist with CT interventional<br />
procedures, but may also be<br />
very useful for PET CT, radiation therapy,<br />
ultrasound, fusion imaging, and other<br />
procedures and modalities where respiratory<br />
motion is an issue. At the depart-<br />
1 The IBC system brings down the total procedure time. In this example, the time from placing the reference grid to harvesting three samples<br />
from a small lung nodule was less than 50 seconds.<br />
60
2<br />
2 Combining CT-guided procedures with the Interactive Breath-Hold Control device (IBC) has been shown to increase the radiologists’ accuracy<br />
and confidence with needle biopsy of the lung.<br />
ment of Diagnostic Radiology, RWTH<br />
Aachen University Hospital in Germany,<br />
a study was conducted to evaluate the<br />
IBC system in CT-guided lung biopsy.<br />
Schoth and colleagues assessed the effect<br />
of an IBC system on procedure time and<br />
technical success in trans-thoracic CTguided<br />
lung biopsies. In 36 patients with<br />
a pulmonary nodule, CT-guided biopsy<br />
was done using a <strong>SOMATOM</strong> Definition<br />
scanner, the Adaptive 3D Intervention<br />
Suite from <strong>Siemens</strong> and the breath-hold<br />
device. In a two-arm study with and<br />
without the device, the biopsy was visually<br />
successful in all patients. The diameter<br />
of the target lesion was comparable<br />
in both groups (IBC: 30 +/– 19 mm; control:<br />
28 +/– 15 mm). But the number of<br />
imaging steps was significantly smaller<br />
(p < 0.05) and the intervention time was<br />
significantly shorter (p < 0.05) in the IBC<br />
group (IBC: 9 +/– 5 steps, 17 +/– 10 min;<br />
control: 13 +/– 5 steps, 26 +/– 12 min).<br />
Application of the IBC unit reduced the<br />
intervention time and radiation expo-<br />
sure in CT-guided biopsy of pulmonary<br />
nodules while reducing the procedure<br />
steps.<br />
In combination with optimized planning<br />
using the new Adaptive 3D Intervention<br />
software from <strong>Siemens</strong> for 3D CT-guided<br />
interventions, biopsy of smaller nodules<br />
becomes much easier, resulting in a<br />
higher technical success rate. With the<br />
early detection and histological proof of<br />
lung cancer, treatment is more effective.<br />
Prognosis significantly improves when<br />
lung cancer is detected and treated before<br />
metastases occur. Therefore, a high<br />
success rate of diagnostic punctures<br />
during the diagnostic workup greatly<br />
supports therapy. Moreover, IBC is a relevant<br />
support to therapeutic procedures<br />
such as radiofrequency ablation or stereotactic<br />
radiation therapy of small lung<br />
tumors.<br />
Regarding dose reduction, the IBC integrates<br />
and supplements perfectly into<br />
the huge expertise that <strong>Siemens</strong> has<br />
accumulated to reduce radiation dose in<br />
* The device will be distributed by Medspira (USA) (www.medspira.com) and <strong>Siemens</strong> AG.<br />
Science<br />
CT-guided examinations with such applications<br />
as CARE Dose4D and HandCARE,<br />
protecting patients and physicians from<br />
radiation exposure during CT interventions.<br />
Schoth F, Plumhans C, Kraemer N, Mahnken A,<br />
Friebe M, Günther RW, Krombach G. – Evaluation<br />
of an Interactive Breath-Hold Control System<br />
in CT-Guided Lung Biopsy. Rofo. 2010 Feb 8.<br />
3<br />
3 Interactive Breath-Hold Control System was<br />
developed by Mayo Clinic Rochester, USA to assist<br />
CT-guided interventional procedures.*<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 67
Science<br />
Scientifi c Validation of the<br />
<strong>SOMATOM</strong> Defi nition Flash<br />
One of the cornerstones of <strong>Siemens</strong> CT activities has always been the<br />
scientifi c validation of <strong>Siemens</strong>’ products and solutions. Independent peerreview<br />
of publications in scientifi c journals provides an unbiased and<br />
objective assessment of the capabilities of the systems.<br />
By Stefan Ulzheimer, PhD, and Peter Seitz<br />
Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
Since the introduction of the <strong>Siemens</strong><br />
<strong>SOMATOM</strong> Definition Flash at RSNA<br />
2008, and its commercial availability in<br />
July 2009, the CT scanner has been covered<br />
in 15 presentations at the annual<br />
meeting of the Radiological Society<br />
of North America in 2009 and ten peerreviewed<br />
publications in renowned<br />
journals.<br />
These presentations and publications<br />
prominently feature the notable advantages<br />
of the <strong>SOMATOM</strong> Definition Flash<br />
that enhance efficiency and significantly<br />
improve patient care.<br />
Split-second Thorax – Lell et al. from<br />
the University Hospital of Erlangen demonstrated<br />
the <strong>SOMATOM</strong> Definition<br />
Flash’s capabilities with its high-pitch<br />
scan mode in thorax examinations. 1<br />
Twenty-four consecutive patients who<br />
presented with chest pain received a<br />
high-pitch thorax scan (Pitch 3.2) to<br />
exclude coronary artery disease, pulmonary<br />
embolism and aortic dissection.<br />
The average dose was 1.6 mSv for patients<br />
who were scanned with a 100 kV<br />
protocol and 3.2 mSv for patients who<br />
were scanned with a 120 kV protocol.<br />
The authors conclude that the “[…] highpitch<br />
scan mode allows motion artifact<br />
free and accurate visualization of the<br />
thoracic vessels and diagnostic image<br />
quality of the coronary arteries in patients<br />
with low and stable heart rates at<br />
a very low radiation exposure.”<br />
The dose saving potential of the highpitch<br />
scan mode of <strong>SOMATOM</strong> Definition<br />
Flash was also evaluated by Sommer et<br />
al. in a study using an anthropomorphic<br />
phantom and the data of 31 patients. 2<br />
The average scan time for the complete<br />
thorax was 0.7 seconds, the average<br />
dose 4.1 mSv, only one fifth of the dose<br />
of a conventional gated chest scan.<br />
Sub-mSv Heart – The robust visualization<br />
of the coronary arteries with excellent<br />
image quality at ultra low doses of<br />
below 1 mSv was the focus of three publications<br />
by researchers from Zurich,<br />
Switzerland 3 and Erlangen, Germany. 4,5<br />
The latest study from Erlangen used the<br />
Flash Spiral scan mode in 50 consecutive<br />
patients with body weight up to 100 kg<br />
and heart rates up to 60 beats per minute<br />
with an average effective dose of<br />
0.78 to 0.99 mSv and excellent image<br />
quality. 5 The average dose was 0.87<br />
mSv. In a similar study from Zurich,<br />
Leschka et al. found an average dose of<br />
0.9 mSv in 35 consecutive patients. 3 In<br />
both studies 99% of all coronary segments<br />
could be evaluated 3,5 and the image<br />
quality was rated excellent in 94 %<br />
of the segments or as, “at least good,” in<br />
5 % of the segments. 5<br />
Assessment of Myocardial Perfusion –<br />
The <strong>SOMATOM</strong> Definition Flash offers<br />
completely new possibilities to assess<br />
perfusion deficits in the myocardium<br />
68 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
due to its unmatched temporal resolution<br />
and high volume coverage even at<br />
high heart rates in stressed patients.<br />
Bastarrika et al. showed that “[…] this<br />
technique can demonstrate subendocardial<br />
infarction not seen on SPECT but<br />
confirmed by MRI and can detect ischemia<br />
in good correlation with stressperfusion<br />
MRI and SPECT.” 6 Fig. 1 shows<br />
a short axis view of the myocardium<br />
comparing stress perfusion measured<br />
with the <strong>SOMATOM</strong> Definition Flash<br />
(Fig. 1A) and SPECT (Fig. 1B).<br />
Single Dose Dual Energy – The latest<br />
innovation in the area of Dual Energy CT<br />
(DECT), the Selective Photon Shield, is<br />
based on an additional tin filter (TF)<br />
for the high energy spectrum on the<br />
<strong>SOMATOM</strong> Definition Flash. The Selective<br />
Photon Shield allows for the acquisition<br />
of Dual Energy data without any<br />
dose penalty compared to standard single<br />
energy scans and significantly improves<br />
the separation of the energy spectra.<br />
A group of scientists from Zurich confirmed<br />
this for the syngo application,<br />
“Calculi Characterization,” using it for the<br />
differentiation of uric acid (UA) and non-<br />
UA stones and concluded: “DECT with TF<br />
and 80-140 kV tube voltage settings<br />
significantly improves the discrimination<br />
between UA-containing and non-UA<br />
containing urinary stones as compared<br />
with DECT without using the TF […].” 7<br />
Lell et al. from the University of Erlangen
1A<br />
1 New frontiers in cardiac diagnosis with CT: stress-perfusion images of the heart using the unmatched temporal resolution of the<br />
<strong>SOMATOM</strong> Definition Flash compared to SPECT. A stress perfusion scan on the <strong>SOMATOM</strong> Definition Flash nicely depicts a perfusion<br />
defect in the myocardium (Fig. 1A). The perfusion defect could be confirmed using SPECT (arrows, Fig. 1B). Courtesy of Joseph Schoepf,<br />
MD, Medical University of South Carolina, USA.<br />
evaluated the application of DECT to<br />
create bone-free data sets to assess the<br />
supraaortic arteries. 8 Automatic bone<br />
removal allows for a faster and more reliable<br />
diagnosis of vessels close to boney<br />
structures. The authors conclude that<br />
“[…] excellent bone suppression could<br />
be achieved” using the improved scan<br />
modes and evaluation methods on the<br />
<strong>SOMATOM</strong> Definition Flash.<br />
By combining multi-phase protocols to<br />
one Dual Energy exam, the dose-saving<br />
potential of DECT was evaluated by<br />
Sommer et al. in patients after endovascular<br />
aneurism repair using virtual noncontrast<br />
images. They achieved a dose<br />
reduction of 44 % compared to a biphase<br />
protocol. In 70 examinations, all<br />
24 endoleaks were detected and correctly<br />
classified. 9<br />
More to Come – In addition to the<br />
above mentioned publications, many<br />
others are in the pipeline, promising to<br />
validate the technical advancements of<br />
the <strong>SOMATOM</strong> Definition Flash and,<br />
even more importantly, how this translates<br />
into clinical and workflow advan-<br />
tages. For example, a special issue of<br />
“Investigative Radiology” on “Advances<br />
in CT technology,” specifically focusing<br />
on Dual Source, Dual Energy CT and<br />
multi-slice CT with 128 or more slices,<br />
is scheduled for this summer.<br />
1 Lell M, Hinkmann F, Anders K, Deak P, Kalender<br />
WA, Uder M, Achenbach S. High-pitch electrocardiogram-triggered<br />
computed tomography of<br />
the chest: initial results, Invest Radiol. 2009<br />
Nov;44(11):728-33.<br />
2 Sommer WH, Schenzle JC, Becker CR, Nikolaou<br />
K, Graser A, Michalski G, Neumaier K, Reiser MF,<br />
Johnson TR. Saving Dose in Triple-Rule-Out Computed<br />
Tomography Examination Using a High-<br />
Pitch Dual Spiral Technique. Invest Radiol. 2010<br />
Feb;45(2):64-71.<br />
3 Leschka S, Stolzmann P, Desbiolles L, Baumueller<br />
S, Goetti R, Schertler T, Scheffel H, Plass A, Falk V,<br />
Feuchtner G, Marincek B, Alkadhi H. Diagnostic<br />
accuracy of high-pitch dual-source CT for the<br />
assessment of coronary stenoses: first experience.<br />
Eur Radiol. 2009 Dec;19(12):2896-903.<br />
4 Lell M, Marwan M, Schepis T, Pflederer T, Anders<br />
K, Flohr T, Allmendinger T, Kalender W, Ertel D,<br />
Thierfelder C, Kuettner A, Ropers D, Daniel WG,<br />
Achenbach S. Prospectively ECG-triggered highpitch<br />
spiral acquisition for coronary CT Angiography<br />
using dual source CT: technique and initial<br />
experience. Eur Radiol. 2009 Nov;19(11):2576-83.<br />
5 Achenbach S, Marwan M, Ropers D, Schepis T,<br />
Pflederer T, Anders K, Kuettner A, Daniel WG,<br />
1B<br />
Science<br />
Uder M, Lell MM. Coronary computed tomography<br />
angiography with a consistent dose below<br />
1 mSv using prospectively electrocardiogramtriggered<br />
high-pitch spiral acquisition. Eur Heart<br />
J. 2010 Feb;31(3):340-6.<br />
6 Bastarrika G, Ramos-Duran L, Schoepf UJ, Rosenblum<br />
MA, Abro JA, Brothers RL, Zubieta JL, Chiaramida<br />
SA, Kang DK Adenosine-stress dynamic<br />
myocardial volume perfusion imaging with second<br />
generation dual-source computed tomography:<br />
Concepts and first experiences. JCCT 2010<br />
DOI: 10.1016/j.jcct.2010.01.015.<br />
7 Stolzmann P, Leschka S, Scheffel H, Rentsch K,<br />
Baumüller S, Desbiolles L, Schmidt B, Marincek<br />
B, Alkadhi H. Characterization of Urinary Stones<br />
With Dual-Energy CT: Improved Differentiation<br />
Using a Tin Filter. Invest Radiol. 2010 Jan;<br />
45(1):1-6.<br />
8 Lell M, Hinkmann F, Nkenke E, Schmidt B,<br />
Seidensticker P, Kalender WA, Uder M, Achenbach<br />
S. Dual energy CTA of the supraaortic arteries:<br />
Technical improvements with a novel dual<br />
source CT system. Eur J Radiol. 2009 Oct 8<br />
[Epub ahead of print].<br />
9 Sommer WH, Graser A, Becker CR, Clevert DA,<br />
Reiser MF, Nikolaou K, Johnson TR. Image quality<br />
of virtual noncontrast images derived from dualenergy<br />
CT Angiography after endovascular<br />
aneurysm repair. J Vasc Interv Radiol. 2010 Mar;<br />
21(3):315-21.<br />
10 Johnson TR, Schenzle JC, Sommer WH, Michalski<br />
G, Neumaier K, Lechel U, Nikolaou K, Becker H-C,<br />
Reiser MF. Dual energy CT: How about the dose?<br />
Invest Radiol. 2010 (in press).<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 69
Life<br />
Behind the Scenes:<br />
CT Scan Protocols<br />
Standard scan protocols are by far more sophisticated than CT users might<br />
realize. Christiane Koch is the scan protocol designer for <strong>Siemens</strong> <strong>Healthcare</strong>,<br />
Computed Tomography and knows what is important in this fi eld.<br />
By Heike Theessen<br />
Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
How would you describe your job<br />
as a scan protocol designer?<br />
Koch: My task is to create scan protocols<br />
for all scanners and all software versions.<br />
Together with colleagues from<br />
departments of physics, product definition,<br />
marketing, development and the<br />
application specialists, I design and set<br />
up <strong>Siemens</strong> default scan protocols.<br />
In doing so, dose and other guidelines<br />
of various radiological societies from<br />
different countries need to be observed.<br />
Scan protocols have to be comparable<br />
through different software versions and<br />
scanner models. For example a protocol<br />
called “AbdomenRoutine” on a<br />
<strong>SOMATOM</strong> Emotion is similar to the<br />
protocol on a <strong>SOMATOM</strong> Definition.<br />
I consolidate the data for the scan protocols<br />
in a comprehensive data base.<br />
These files become translated to a database<br />
called, “ModeLibrary”, and afterwards<br />
as usable scan protocol to the<br />
user interface.<br />
I am in close collaboration with customers<br />
and application specialists worldwide,<br />
both during the development<br />
phase and after systems are installed.<br />
How do you validate scan protocols<br />
before a new scanner is released?<br />
Koch: Functionality and performance are<br />
tested with phantoms in our laboratory<br />
during the development phase. For intuitive<br />
tests, we do invite Radiographers in<br />
order to simulate a real live scenario.<br />
This is all done before new scanners are<br />
delivered to any customer. Then, during<br />
the so-called “Market Entrance Phase”,<br />
our collaboration partners begin scanning<br />
patients and the scan protocols are<br />
clinically tested. The results are reviewed<br />
and validated by radiologists and physicists.<br />
Before the new CT system is finally<br />
released, scan protocols are adapted<br />
according to the results of all prior tests.<br />
70 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
Christiane Koch is the scan protocol designer for <strong>Siemens</strong> CT.<br />
What is important to know when<br />
users want to change parameters in<br />
a default scan protocol?<br />
Koch: Around 50% of all scan protocol<br />
parameters run in the background.<br />
These parameters are, for example, dose<br />
modulation types and additional reconstruction<br />
algorithms. It would be ideal if<br />
our customers would use the default protocols.<br />
In this manner, following the
Data for the scan protocols are being consolidated in a comprehensive<br />
data base.<br />
ALARA principle, the best possible image<br />
quality at the lowest possible dose can<br />
be achieved. But, of course, all users need<br />
to adapt certain parameters to fit their<br />
individual needs such as breathing<br />
instructions for the patient or transfer<br />
rules indicating where images should<br />
be sent.<br />
If the operator wants to change any<br />
parameters within a scan protocol, it is<br />
important to select the correct base protocol.<br />
For example an “AbdomenRoutine”<br />
protocol should not be changed to<br />
fit a neck examination and vice versa.<br />
Also, if an institute has scanners from<br />
different vendors or different scanner<br />
models, tube current values can not be<br />
compared when it comes to dose. Only<br />
the CTDIvol value represents a comparable<br />
figure. The CTDIvol is a measured<br />
value of the dose absorbed during a<br />
CT examination.<br />
Dedicated children protocols are provided<br />
on all <strong>Siemens</strong> CT scanners. What<br />
is so special about these protocols?<br />
Koch: Children scan protocols are developed<br />
in cooperation with pediatric<br />
radiologists in order to ensure even<br />
lower dose values as compared to adult<br />
protocols. By using children protocols,<br />
the user does not have to adjust dose<br />
values to the age or weight of the child.<br />
In these protocols, CARE Dose4D automatically<br />
adapts the tube current to the<br />
individual patient’s anatomical charac-<br />
teristics. However, children older than<br />
6 years or heavier than 55 kg can be<br />
examined with regular adult protocols.<br />
Fast scan times are very helpful when<br />
scanning children since they probably<br />
will not, or cannot, hold still for the<br />
duration of the scan. An increased pitch<br />
value or faster rotation time also support<br />
fast acquisitions. Repeated scanning<br />
can be avoided.<br />
Where can users find more information<br />
about CT scan protocols?<br />
Koch: The Workflow Assistant is included<br />
within the CT Life Card. It is available for<br />
the <strong>SOMATOM</strong> Definition family starting<br />
with software version syngo CT 2007B<br />
(VA11). Application Guides do exist for<br />
older scanner models. These media<br />
include valuable facts about scan protocols,<br />
physical fundamentals, dose measures<br />
and practical tips and tricks.<br />
Life<br />
“The best possible image<br />
quality at the lowest dose<br />
can be achieved by using<br />
the default scan protocols.”<br />
Christiane Koch, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>,<br />
Forchheim, Germany.<br />
Tips from the expert:<br />
� Do not use a protocol from a certain<br />
body region and change it to<br />
a protocol to fit another body<br />
region.<br />
� When comparing dose values of<br />
different scanner models and<br />
different vendors, it is important<br />
to compare CTDIvol values, not<br />
tube current values. Tube current<br />
values are related primarily to<br />
filter settings and the scanner<br />
geometry.<br />
� Customized scan protocols can be<br />
exported through the Scan Protocol<br />
Assistant to Excel to be used on<br />
a PC for further documentation,<br />
e.g. documentation of dose values.<br />
� All or certain scan protocols can<br />
be copied from one scanner to<br />
another scanner via the Scan Protocol<br />
Assistant. Pre-conditions are<br />
the same scanner model and identical<br />
software version.<br />
www.siemens.com/life-courses<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 71
Life<br />
First syngo.via Hands-on<br />
Workshops at ECR 2010<br />
By Heike Theessen, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
For the 6th consecutive year, <strong>Siemens</strong><br />
<strong>Healthcare</strong> offered hands-on workshops<br />
in the experience lounge at ECR 2010.<br />
Participants could benefit from very<br />
comprehensive sessions for CT, MR as<br />
well as PET and SPECT CT.<br />
Unlike previous years however, the new<br />
imaging software syngo.via* was used<br />
for the sessions CT Cardiology, CT Oncology<br />
and CT Colonography. During the 90<br />
minute sessions, Tobias Pflederer, MD,<br />
from Erlangen University and Thomas<br />
Mang, MD, from Vienna University, demonstrated<br />
how they can use syngo.via<br />
for their daily reporting.<br />
At the beginning of each session, a theoretical<br />
introduction into the topic was<br />
given by the speakers. Pflederer pointed<br />
out the various dose reduction possibilities<br />
for Cardiac CT while Mang gave an<br />
overview of patient preparation and<br />
reading techniques for CT Colonography.<br />
After a brief demonstration of syngo.via<br />
by <strong>Siemens</strong> application specialists, the<br />
Upcoming Events & Congresses<br />
72 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
T. Mang, MD, hold the session on CT Colonography using syngo.via<br />
participants could experience <strong>Siemens</strong><br />
new imaging software for themselves.<br />
The instructing physicians guided them<br />
step-by-step through the applications,<br />
explaining the benefits of syngo.via.<br />
Customers particularly liked the automated<br />
case preparation, where all coronary<br />
arteries are automatically labelled<br />
and functional evaluations for left and<br />
right ventricle are already done.<br />
Next workshops with syngo.via are<br />
planned for ESC 2010 in Stockholm.<br />
* syngo.via can be used as a standalone device or together with a variety of syngo.via based software options, which are medical devices in their own rights.<br />
Title Location Short Description Date Contact<br />
ASNR Boston, USA 48th Annual Meeting May 15-20, 2010 www.asnr.org<br />
ISCT San Francisco, 12th International May 18–21, 2010 www.isct.org<br />
USA Symposium on<br />
Multidetector-Row CT<br />
WCC Bejing, China World Congress of June 16–19, 2010 www.worldheart.org<br />
Cardiology Scientific<br />
<strong>Sessions</strong> 2010<br />
SCCT Las Vegas, USA 5th Annual July 14–15, 2010 www.scct.org<br />
Scientific Meeting<br />
ESC Stockholm, Cardiology August 28 – www.escardio.org<br />
Sweden Congress September 01, 2010<br />
ESNR Bologna, Italy Neuroradiology October 04–09, 2010 www.esnr.org<br />
Congress<br />
RSNA Chicago, USA Annual Meeting of November 28– www.rsna.org<br />
Radiological Society December 03, 2010<br />
of North America
Training Website for Knowledge Improvement<br />
By Jakub Mochon, Computed Tomography Division, <strong>Siemens</strong> Medical Solutions, Malvern, Pennsylvania, USA<br />
Recent years have brought significant<br />
progress to the area of ischemic stroke<br />
therapy. Equally important developments<br />
have taken place on the diagnostic<br />
side. With availability of Adaptive4D<br />
Spiral on all <strong>SOMATOM</strong> Definition scanners,<br />
coverage for perfusion imaging<br />
has been extended beyond the limitation<br />
of the detector size. Physicians can<br />
now adjust the coverage to the specific<br />
needs of the patient and the indications<br />
of the neurological exam. New syngo<br />
Volume Perfusion CT Neuro software<br />
offers improved guided workflow and<br />
enables rapid sharing of perfusion data<br />
and maps utilizing syngo Expert-i. In order<br />
to improve the knowledge on <strong>Siemens</strong><br />
offerings in this area, <strong>Siemens</strong> USA<br />
<strong>Siemens</strong>’ newest application for neurological<br />
imaging, syngo Volume Perfusion<br />
CT Neuro, can now be tried for 90 days<br />
at no cost.<br />
syngo Volume Perfusion CT Neuro facilitates<br />
quantitative 3D volume evaluation<br />
for differential diagnosis of brain tumors<br />
and ischemic stroke. In combination<br />
with Adaptive 4D Spiral technology, extended<br />
brain coverage is feasible.* It is<br />
the most complete 3D stroke evaluation<br />
software on the market and the only application<br />
with both maximum slope and<br />
deconvolution models integrated, supporting<br />
diagnostic results even in critical<br />
situations. With the 3D Auto Stroke functionality,<br />
therapeutic decisions can be<br />
made without complex user interac-<br />
has launched a dedicated website:<br />
https://www.med.usa.siemens.com/<br />
stroke. Particularly beneficial is the three<br />
part Webcast presented by Ke Lin, MD,<br />
from New York University: https://www.<br />
med.usa.siemens.com/stroke/webcast/<br />
Part 1: Appropriateness of perfusion in<br />
stroke diagnosis: Where and when to<br />
use it.<br />
Part 2: Workflow, Acquisition and Post<br />
Processing.<br />
Part 3: How to read and interpret studies.<br />
<strong>Siemens</strong> is also working closely with Applied<br />
Radiology: http://www.appliedradiology.com/<br />
on an educational stroke<br />
forum that will further discuss the diverse<br />
needs of the stroke teams at the clinics<br />
and particularly emphasize the beneficial<br />
Free Trial Licenses for Neuro Imaging<br />
By Marion Meusel, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
tions. All relevant perfusion parameters<br />
(CBF, CBV, TTP, MTT) are shown in one<br />
view. The integrated “3D Tissue at Risk<br />
Evaluation” gives confidence in the differentiation<br />
between cerebral tissue at<br />
risk and core infarct. All these features<br />
make syngo Volume Perfusion CT Neuro<br />
night shift and 24/7 service ready.<br />
role and utility of CT imaging in<br />
stroke care.<br />
Life<br />
In order to improve the knowledge on <strong>Siemens</strong><br />
offerings, <strong>Siemens</strong> USA has launched a dedicated<br />
website https://www.med.usa.siemens.com/stroke<br />
Similar free-trial licenses are available<br />
for many more clinical applications.<br />
International:<br />
www.siemens.com/DiscoverCT<br />
USA only: www.usa.siemens.com/<br />
webShop/CT<br />
syngo Volume<br />
Perfusion CT Neuro –<br />
All dynamic information<br />
in one view.<br />
*Available for the<br />
<strong>SOMATOM</strong> Definition<br />
family only.
Frequently Asked Questions<br />
By Ivo Driesser, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
In the Scan Protocol Assistant (SPA),<br />
the user has access to all scan protocols.<br />
These protocols can be adapted, changed<br />
or deleted. Everything is clearly listed<br />
as in the patient model dialog. The<br />
layout is comparable to the examination<br />
<strong>Siemens</strong> <strong>Healthcare</strong> will offer a workshop<br />
on Dual Energy CT in cooperation<br />
with Thorsten Johnson, MD, Associate<br />
Professor of Radiology and Head of Computed<br />
Tomography at Munich University<br />
Hospital, Campus Großhadern, Germany.<br />
The course will take place in Forchheim,<br />
Germany from September 10th to September<br />
11th 2010.<br />
The field of Dual Energy CT scanning<br />
is expanding incredibly fast. Twelve different<br />
FDA cleared Dual Energy applications<br />
have already been introduced since<br />
the launch of Dual Source CT in 2005,<br />
creating both clinical and educational<br />
demand. <strong>Siemens</strong> <strong>Healthcare</strong> will provide<br />
a comprehensive overview to those who<br />
are just starting to integrate Dual Energy<br />
CT into their daily routine with emphasis<br />
on understanding the principles and fully<br />
card, which makes it easy to find the<br />
entries which should be changed.<br />
How can SPA help in daily routine?<br />
1. The entry “CTDIvol”, for example, can<br />
be added for all scan protocols as follows:<br />
First the SPA has to be opened, via<br />
Dual Energy CT: Learning From the Experts<br />
By Heike Theessen, Business Unit CT, <strong>Siemens</strong> <strong>Healthcare</strong>, Forchheim, Germany<br />
utilizing the potential of Dual Energy CT.<br />
The two-day training session will include<br />
presentations on both the physical principles<br />
and the clinical benefits of Dual<br />
Energy CT. A hands-on session at a<br />
<strong>SOMATOM</strong> Definition scanner, as well as<br />
on a workstation for extended case review<br />
is also part of the workshop. “Some<br />
of the things covered in the workshop<br />
During a workshop<br />
Thorsten Johnson, MD<br />
will present both the<br />
physical principles<br />
and clinical benefits<br />
of Dual Energy CT.<br />
74 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
Example of<br />
the Trigger<br />
card of<br />
<strong>SOMATOM</strong><br />
Definition<br />
scanner.<br />
“Options”, “Configuration” and “Scan<br />
Protocol Assistant”.<br />
Step 1: Select “Change Protocols.”<br />
Step 2: Select all protocols.<br />
Step 3: Go to “scan” where you see all<br />
the scan parameters. Click on the configuration<br />
icon (marked in red on the image).<br />
Select the “CTDIvol” box and place in<br />
the menu bar via the arrow (marked in<br />
green). Click on the configuration icon<br />
again. If desired the“CTDIvol” entry can be<br />
selected in the menu bar and moved to<br />
the preferred location.<br />
2. For 3D reconstructions it is preferable<br />
to have a non-square matrix. Select in<br />
Step 2 all the affected protocols by using<br />
the filter “3D recon jobs”. In in Step 3<br />
you can change the matrix size. Select<br />
the column “Matrix size” and in the l ower<br />
part, make your changes. All selected<br />
protocols will now be changed.<br />
In this way, protocols are easily and quickly<br />
adapted to the users preferences.<br />
have been used reliably in daily routine<br />
for years. Some others are only a couple<br />
of months old. Upon completion of the<br />
workshop, participants will be at the forefront<br />
of Dual Energy technology,” says<br />
course director Johnson.<br />
www.siemens.com/life-courses
Clinical Workshops 2010<br />
As a cooperation partner of many renowned hospitals,<br />
<strong>Siemens</strong> <strong>Healthcare</strong> offers continuing CT training programs.<br />
A wide range of clinical workshops keeps participants at<br />
the forefront of clinical CT imaging.<br />
Workshop Title Dates Location Course Course<br />
language director<br />
Clinical Workshop on July, 28–30 2010 Erlangen, English Prof. Stephan Achenbach, MD<br />
Cardiac CT / Erlangen Germany<br />
Clinical Workshop on July, 07–09 2010 Munich, English PD Konstantin Nikolaou, MD<br />
Cardiac CT / Munich December, Germany Prof. Christoph Becker, MD<br />
15 –17 2010 Alexander Becker, MD<br />
Clinical CTA Interpretation November, Erlangen, English Prof. Stephan Achenbach, MD<br />
Course / Erlangen 18–19 2010 Germany<br />
Hands-on Workshop September, St. Gallen, German PD Hatem Alkadhi, MD<br />
Cardiac CT 23–25 2010 Switzerland PD Sebastian Leschka, MD<br />
Clinical Training Course June, 26–27 2010 Kuching, English Prof. Sim Kui Hian, MD<br />
on Cardiac CT October, 30–31 2010 Malaysia Ong Tiong Kiam, MD<br />
Virtual CT-Colonography June, 11–12 2010 Berlin, German Prof. Bernd Lünstedt, MD<br />
November, 05–06 2010 Germany<br />
Dual Energy Workshop September, Forchheim, English PD Thorsten Johnson, MD<br />
10 –11 2010 Germany<br />
ESGAR CT-Colonography September, Lisbon (Cascais), English<br />
Workshops 23–24 2010 Portugal Prof. Filippe Caseiro-Alves, MD<br />
April Dublin, Prof. Helen Fenlon, MD<br />
13–15, 2011 Ireland Martina Morrin, MD<br />
September Gothenburg, Prof. Mikael Hellström, MD<br />
14 –16, 2011 Sweden<br />
Cardiac-CT Workshop/ Autumn 2010 Dubai, UAE English PD Christoph Becker, MD<br />
Dubai Alexander Becker, MD<br />
Hands-on Workshops August, Stockholm, English n.a.<br />
during ESC 2010 28–31 2010 Sweden<br />
Experience Lounge November, 28 – Chicago, English n.a.<br />
at RSNA 2010 December, 2 2010 USA<br />
In addition, you can always fi nd the latest CT courses offered by <strong>Siemens</strong> <strong>Healthcare</strong> at www.siemens.com/<strong>SOMATOM</strong>Educate<br />
Life<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 75
Life<br />
<strong>Siemens</strong> <strong>Healthcare</strong> – Customer Magazines<br />
Our customer magazine family offers the latest information and background for every<br />
healthcare fi eld. From the hospital director to the radiological assistant – here, you can<br />
quickly fi nd information relevant to your needs.<br />
Medical Solutions<br />
The Magazine for <strong>Healthcare</strong> Leadership<br />
May 2010<br />
Medicine in 2050<br />
How today’s babies will grow into the future of healthcare<br />
Inhalt_May_10_eng.indd 1 23.04.10 09:10<br />
AXIOM Innovations<br />
Everything from the worlds<br />
of interventional radiology,<br />
cardiology, fluoroscopy,<br />
and radiography. This semiannual<br />
magazine is primarily<br />
designed for physicians,<br />
physicists, researchers, and<br />
medical technical personnel.<br />
Medical Solutions<br />
Innovation and trends<br />
in healthcare. The<br />
magazine, published<br />
three times a year, is<br />
designed especially<br />
for members of the<br />
hospital management,<br />
administration personnel,<br />
and heads of<br />
medical departments.<br />
MAGNETOM Flash<br />
Everything from the world<br />
of magnetic resonance<br />
imaging. The magazine<br />
presents case reports,<br />
technology, product news,<br />
and how-to’s. It is primarily<br />
designed for physicians,<br />
physicists, and medical<br />
technical personnel.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong><br />
Everything from the world<br />
of computed tomography.<br />
With its innovations, clinical<br />
applications, and visions,<br />
this semiannual magazine<br />
is primarily designed for<br />
physicians, physicists,<br />
researchers, and medical<br />
technical personnel.<br />
For current and prior issues and to order the magazines, please visit www.siemens.com/healthcare-magazine<br />
76 <strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine<br />
News<br />
Our latest topics<br />
such as product<br />
news, reference<br />
stories, reports,<br />
and general<br />
interest topics are<br />
always available at<br />
www.siemens.com/<br />
healthcare-news<br />
Perspectives<br />
Everything from the world<br />
of clinical diagnostics. This<br />
semi-annual publication provides<br />
clinical labs with diagnostic<br />
trends, technical innovations,<br />
and case studies.<br />
It is primarily designed for<br />
laboratorians, clinicians and<br />
medical technical personnel.
<strong>SOMATOM</strong> <strong>Sessions</strong> – IMPRINT<br />
© 2010 by <strong>Siemens</strong> AG, Berlin and Munich<br />
All Rights Reserved<br />
Publisher:<br />
<strong>Siemens</strong> AG<br />
<strong>Healthcare</strong> Sector<br />
Business Unit Computed Tomography<br />
<strong>Siemens</strong>straße 1, 91301 Forchheim, Germany<br />
Chief Editors:<br />
Monika Demuth, PhD<br />
(monika.demuth@<br />
siemens.com)<br />
Stefan Wünsch, PhD<br />
(stefan.wuensch@<br />
siemens.com)<br />
Responsible for Contents: André Hartung<br />
Editorial Board:<br />
Andreas Blaha<br />
Helge Bohn<br />
Andreas Fischer<br />
Thomas Flohr, PhD<br />
Julia Hoelscher<br />
Klaudija Ivkovic<br />
Axel Lorz<br />
Peter Seitz<br />
Stefan Ulzheimer, PhD<br />
Alexander Zimmermann<br />
Authors of this Issue<br />
H. Alkadhi, MD, Institute of Diagnostic Radiology,<br />
University Hospital Zurich, Zurich, Switzerland<br />
F. Bamberg, MD, Department of Clinical Radiology,<br />
University of Munich, Campus Großhadern,<br />
Munich, Germany<br />
R. W. Bauer, MD, Department of Diagnostic and<br />
Interventional Radiology, Clinic of the Goethe<br />
University, Frankfurt, Germany<br />
Note in accordance with § 33 Para.1 of the German Federal Data Protection Law:<br />
Despatch is made using an address file which is maintained with the aid of an<br />
automated data processing system.<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> with a total circulation of 35,000 copies is sent free of charge<br />
to <strong>Siemens</strong> Computed Tomography customers, qualified physicians and radiology<br />
departments throughout the world. It includes reports in the English language<br />
on Computed Tomography: diagnostic and therapeutic methods and their application<br />
as well as results and experience gained with corresponding systems and<br />
solutions. It introduces from case to case new principles and procedures and discusses<br />
their clinical potential.<br />
The statements and views of the authors in the individual contributions do not<br />
necessarily reflect the opinion of the publisher.<br />
The information presented in these articles and case reports is for illustration only<br />
and is not intended to be relied upon by the reader for instruction as to the practice<br />
of medicine. Any health care practitioner reading this information is reminded<br />
that they must use their own learning, training and expertise in dealing with<br />
their individual patients. This material does not substitute for that duty and is not<br />
intended by <strong>Siemens</strong> Medical Solutions to be used for any purpose in that regard.<br />
A. Becker, MD, Department of Clinical Radiology,<br />
University of Munich, Campus Großhadern,<br />
Munich, Germany<br />
C. R. Becker, MD, Department of Clinical Radiology,<br />
University of Munich, Campus Großhadern,<br />
Munich, Germany<br />
G. Feuchtner, MD, Institute of Diagnostic Radiology,<br />
University Hospital Zurich, Zurich, Switzerland<br />
M. Fischer, MD, Institute of Diagnostic Radiology,<br />
University Hospital Zurich, Zurich, Switzerland<br />
R. Goetti, MD, Institute of Diagnostic Radiology,<br />
University Hospital Zurich, Zurich, Switzerland<br />
W. Heindel, MD, Department of Clinical Radiology,<br />
University Hospital, Münster, Germany<br />
J. M. Kerl, MD, Department of Diagnostic and<br />
Interventional Radiology, Clinic of the Goethe<br />
University, Frankfurt, Germany<br />
M. Lell, MD, Department of Radiology and<br />
the Imaging Science Institute (ISI), University<br />
of Erlangen-Nuremberg, Erlangen, Germany<br />
S. Leschka, MD, Institute of Diagnostic Radiology,<br />
University Hospital Zurich, Zurich, Switzerland<br />
K. Lin, MD, Department of Radiology, New York<br />
University Langone Medical Center, New York,<br />
NY, USA<br />
A. H. Mahnken, MD, RWTH Aachen University<br />
Hospital, Aachen, Germany<br />
Y. Mizutani, MD, Department of Radiology,<br />
Sakakibara Heart Institute, Tokyo, Japan<br />
K. Nikolaou, MD, Department of Clinical Radiology,<br />
University of Munich, Campus Großhadern,<br />
Munich, Germany<br />
J.-F. Paul, MD, Centre Chirurgical Marie<br />
Lannelongue, Le Plessis-Robinson, France<br />
A. Plass, MD, Clinic of Cardiovascular Surgery,<br />
University Hospital Zurich, Zurich, Switzerland<br />
B. Policeni, MD, Radiology Faculty, Neuroradiology,<br />
University of Iowa Hospitals and Clinics, Iowa<br />
City, Iowa, USA<br />
H. Scheffel, MD, Institute of Diagnostic Radiology,<br />
University Hospital Zurich, Zurich, Switzerland<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> is also available on the internet: www.siemens.com/<strong>SOMATOM</strong>World<br />
F. Schoth, MD, RWTH Aachen University Hospital,<br />
Aachen, Germany<br />
F. Schwarz, MD, Department of Clinical Radiology,<br />
University of Munich, Campus Großhadern,<br />
Munich, Germany<br />
H. Seifarth, MD, Department of Clinical Radiology,<br />
University Hospital, Münster, Germany<br />
K. Takada, MD, Department of Radiology,<br />
Sakakibara Heart Institute, Tokyo, Japan<br />
T. J. Vogl, MD, Department of Diagnostic and<br />
Interventional Radiology, Clinic of the Goethe University,<br />
Frankfurt, Germany<br />
P. Weisser, MD, Department of Diagnostic and Interventional<br />
Radiology, Clinic of the Goethe<br />
University, Frankfurt, Germany<br />
M. Wieser, MD, Clinic of Cardiovascular Surgery,<br />
University Hospital Zurich, Zurich, Switzerland<br />
C. Wyss, MD, Cardiology Division, University<br />
Hospital Zurich, Zurich, Switzerland<br />
Sameh Fahmy, freelance medical and technology<br />
journalist Tony DeLisa, freelance author<br />
Wiebke Kathmann, PhD, freelance scientific journalist<br />
Hildegard Kaulen, PhD, freelance scientific journalist<br />
Oliver Klaffke, freelance scientific journalist<br />
Annette Tuffs, MD, medical journalist<br />
Peter Aulbach; Karin Barthel; Andreas Blaha;<br />
Steven Bell; Ivo Driesser; Kerstin Fellenzer; Tomoko<br />
Fujihara; Jan Freund; Tanja Gassert; Toshihide<br />
Itoh; Christiane Koch, Rami Kusama; Marion<br />
Meusel; Jakub Mochon; Katharina Otani, PhD;<br />
Kerstin Putzer; Heike Theessen; Peter Seitz; Stefan<br />
Ulzheimer PhD; Fernando Vega-Higuera;<br />
Stefan Wünsch, PhD; all <strong>Siemens</strong> <strong>Healthcare</strong><br />
Photo Credits: Greg Morris, Yohanne Lamoulére/<br />
Agentur Focus, Harald Krieg, Thorsten Rother<br />
Production: Norbert Moser, <strong>Siemens</strong> AG,<br />
Medical Solutions<br />
Design and Editorial Consulting:<br />
Independent Medien-Design, Munich, Germany<br />
In cooperation with Primafila AG, Zurich,<br />
Switzerland;<br />
Managing Editor: Christa Löberbauer;<br />
Photo Editor: Susanne Nips; Layout: Claudia<br />
Diem, Mathias Frisch; All at: Widenmayerstraße<br />
16, 80538 Munich, Germany<br />
The drugs and doses mentioned herein are consistent with the approval labeling<br />
for uses and/or indications of the drug. The treating physician bears the sole<br />
responsibility for the diagnosis and treatment of patients, including drugs and<br />
doses prescribed in connection with such use. The Operating Instructions must<br />
always be strictly followed when operating the CT System. The sources for the<br />
technical data are the corresponding data sheets. Results may vary.<br />
Partial reproduction in printed form of individual contributions is permitted, provided<br />
the customary bibliographical data such as author’s name and title of the<br />
contribution as well as year, issue number and pages of <strong>SOMATOM</strong> <strong>Sessions</strong> are<br />
named, but the editors request that two copies be sent to them. The written consent<br />
of the authors and publisher is required for the complete reprinting of an article.<br />
We welcome your questions and comments about the editorial content of<br />
<strong>SOMATOM</strong> <strong>Sessions</strong>. Manuscripts as well as suggestions, proposals and information<br />
are always welcome; they are carefully examined and submitted to the editorial<br />
board for attention. <strong>SOMATOM</strong> <strong>Sessions</strong> is not responsible for loss, damage,<br />
or any other injury to unsolicited manuscripts or other materials. We reserve the<br />
right to edit for clarity, accuracy, and space. Include your name, address, and<br />
phone number and send to the editors, address above.<br />
Imprint<br />
<strong>SOMATOM</strong> <strong>Sessions</strong> · May 2010 · www.siemens.com/healthcare-magazine 77<br />
unsubscribe from info service<br />
“Neuro BestContrast<br />
allows radiologists to<br />
better visualize subtle<br />
edemas as well as<br />
subtle signs of stroke,<br />
and to better delineate<br />
the cortical margin.”<br />
David S. Enterline, MD,<br />
Duke University Medical Center in Durham, North Carolina, USA<br />
Country<br />
State<br />
Yes, I consent to the above information being used<br />
for future contact regarding product updates and other<br />
important news from <strong>Siemens</strong>.<br />
City<br />
Postal Code<br />
E-mail<br />
Street<br />
the monthly healthcare e-newsletter<br />
Please print clearly!<br />
Name<br />
Stay up to date with the latest information<br />
Register for:<br />
Title<br />
AXIOM Innovations<br />
Function<br />
<strong>SOMATOM</strong> <strong>Sessions</strong><br />
Department<br />
MAGNETOM Flash<br />
Medical Solutions<br />
Institution<br />
Please enter your business address<br />
Please include me in your mailing list for the<br />
following <strong>Siemens</strong> <strong>Healthcare</strong> customer magazine(s):<br />
Subscription
SUBSCRIBE NOW!<br />
– and get your free copy of future<br />
<strong>SOMATOM</strong> <strong>Sessions</strong>! Interesting information<br />
from the world of computed tomography – gratis<br />
to your desk. Send us this postcard, or subscribe<br />
online at www.siemens.com/ct-news<br />
<strong>SOMATOM</strong><br />
<strong>Sessions</strong><br />
Rapid evaluation is<br />
critical after trauma and<br />
with symptoms such as<br />
weakness, headache,<br />
and dizziness, which is<br />
why CT is the modality<br />
of choice in these<br />
scenarios. Exceptional<br />
image quality is key to<br />
optimize diagnosis, and<br />
lower dose imaging<br />
minimizes risk to the<br />
patient.<br />
<strong>Siemens</strong> AG<br />
Halthcare Sector<br />
H CC 11<br />
Henkestraße 127<br />
91052 Erlangen<br />
Germany<br />
Global <strong>Siemens</strong> Headquarters<br />
<strong>Siemens</strong> AG<br />
Wittelsbacherplatz 2<br />
80333 Muenchen<br />
Germany<br />
www.siemens.com/healthcare-magazine<br />
On account of certain regional limitations of<br />
sales rights and service availability, we cannot<br />
guarantee that all products included in this<br />
brochure are available through the <strong>Siemens</strong><br />
sales organization worldwide. Availability and<br />
packaging may vary by country and is subject<br />
to change without prior notice. Some/All of<br />
the features and products described herein may<br />
not be available in the United States.<br />
The information in this document contains<br />
general technical descriptions of specifications<br />
and options as well as standard and optional<br />
features which do not always have to be present<br />
in individual cases.<br />
<strong>Siemens</strong> reserves the right to modify the design,<br />
packaging, specifications and options described<br />
herein without prior notice.<br />
Please contact your local <strong>Siemens</strong> sales<br />
representative for the most current information.<br />
Note: Any technical data contained in this<br />
document may vary within defined tolerances.<br />
Original images always lose a certain amount<br />
of detail when reproduced.<br />
Not for distribution in the US.<br />
Global <strong>Siemens</strong><br />
<strong>Healthcare</strong> Headquarters<br />
<strong>Siemens</strong> AG<br />
<strong>Healthcare</strong> Sector<br />
Henkestraße 127<br />
91052 Erlangen<br />
Germany<br />
Phone: +49 9131 84 - 0<br />
www.siemens.com/healthcare<br />
Order No. A91CT-41011-14M1-7600 | Printed in Germany | CC CT 41011 ZS 0510/27. | © 05.2010, <strong>Siemens</strong> AG<br />
Global Business Unit<br />
<strong>Siemens</strong> AG<br />
Medical Solutions<br />
Computed Tomography<br />
<strong>Siemens</strong>straße 1<br />
91301 Forchheim<br />
Germany<br />
Phone: +49 9191 18 - 0<br />
www.siemens.com/healthcare<br />
Local Contact Information<br />
Asia/Pacific:<br />
<strong>Siemens</strong> Medical Solutions<br />
Asia Pacific Headquarters<br />
The <strong>Siemens</strong> Center<br />
60 MacPherson Road<br />
Singapore 348615<br />
Phone: +65 9622 - 2026<br />
www.siemens.com/healthcare<br />
Canada:<br />
<strong>Siemens</strong> Canada Limited<br />
Medical Solutions<br />
2185 Derry Road West<br />
Mississauga ON L5N 7A6<br />
Canada<br />
Phone: +1 905 819 - 5800<br />
www.siemens.com/healthcare<br />
Europe/Africa/Middle East:<br />
<strong>Siemens</strong> AG<br />
Medical Solutions<br />
Henkestraße 127<br />
D-91052 Erlangen<br />
Germany<br />
Phone: +49 9131 84 - 0<br />
www.siemens.com/healthcare<br />
Latin America:<br />
<strong>Siemens</strong> S.A.<br />
Medical Solutions<br />
Avenida de Pte. Julio A. Roca No 516, Piso 7<br />
C1067ABN Buenos Aires Argentina<br />
Phone: +54 11 4340 - 8400<br />
www.siemens.com/healthcare<br />
USA:<br />
<strong>Siemens</strong> Medical Solutions U.S.A., Inc.<br />
51 Valley Stream Parkway<br />
Malvern, PA 19355-1406<br />
USA<br />
Phone: +1-888-826 - 9702<br />
www.siemens.com/healthcare<br />
<strong>SOMATOM</strong> <strong>Sessions</strong><br />
ISCT-Edition May 2010 26


![WalkAway plus Technical Specifications [41 KB] - Siemens Healthcare](https://img.yumpu.com/51018135/1/190x253/walkaway-plus-technical-specifications-41-kb-siemens-healthcare.jpg?quality=85)