Norovirus Outbreak Report 2011/12 - The Royal Wolverhampton ...
Norovirus Outbreak Report 2011/12 - The Royal Wolverhampton ...
Norovirus Outbreak Report 2011/12 - The Royal Wolverhampton ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS Trust<strong>Norovirus</strong> Activity <strong>Report</strong> <strong>2011</strong>-<strong>12</strong>Group / Committee Name: Infection Prevention and Control CommitteeDate of Group /Committee: 27 th July 20<strong>12</strong>Author of <strong>Report</strong>: Carolyn Wiley Operational Nurse Manager Infection Prevention.PURPOSE OF THE REPORT:<strong>Norovirus</strong> outbreaks cause disruption to care delivery across the health economyparticularly during the winter season. Effective management of outbreaks is essential toprevent spread.Case definition: Sudden onset diarrhoea and or vomiting self limiting to twelve to seventytwo hours with no other suspected cause.This report summarises the <strong>Norovirus</strong> activity between October <strong>2011</strong> and May 20<strong>12</strong> at the<strong>Royal</strong> <strong>Wolverhampton</strong> NHS Trust and the <strong>Wolverhampton</strong> care homes, the outbreakmanagement and monitoring systems and actions subsequently required to improvemanagement for coming year. Root cause analysis investigation reports have beencompleted and presented to the Infection Prevention Committee for the four RWHToutbreaks.Criteria Lead Monitoring Frequency Committee<strong>Norovirus</strong> Lead IPN IPCC Post outbreak IPCC<strong>Outbreak</strong>analysisRELEVANCE:Strategic objective in the infection prevention annual programme of work 20<strong>12</strong>-13 -<strong>The</strong> riskof outbreaks will be reduced to a minimum and subsequent organisational disruptionthrough local surveillance and detections of organisms. <strong>Outbreak</strong>s will be reported andmanaged as directed in the <strong>Outbreak</strong> Policy IP13. <strong>Outbreak</strong>s of <strong>Norovirus</strong> will be reportedand managed using <strong>Norovirus</strong> Policy IP18. NHLSA standard 1 Criterion 6 relates to riskmanagement and a Directorate risk assessment 1623 is in place for risk of outbreak.<strong>The</strong> Trust is at risk of an outbreak of infection which may disrupt normal activity and maygive rise to negative media attention and loss of reputation.<strong>Norovirus</strong> activity in care homes and admission avoidance is critical in preventing someoutbreaks in the acute Trust. <strong>Outbreak</strong> management and support for care homes isprovided by the Infection Prevention Team and the data for care home outbreaks istherefore included in this report.POLICY / ACTION PLAN REQUIREMENTSInstitutions and wards across the health economy affected with <strong>Norovirus</strong> or suspected<strong>Norovirus</strong> report outbreaks or potential outbreaks to the Infection Prevention and ControlTeam. As soon as an outbreak is declared the <strong>Outbreak</strong> Policy IP13 is active and dailyinformation is collated from affected areas and fed back through the <strong>Outbreak</strong> ManagementCommittee. <strong>The</strong> <strong>Outbreak</strong> Policy IP13 and the <strong>Norovirus</strong> Policy IP18 detail themanagement of the outbreak. <strong>The</strong> key information is cascaded on a daily basis to keyindividuals outlined in the <strong>Outbreak</strong> Policy including RWHT Capacity, Wards,
<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS TrustHousekeeping, institutions, care homes, Public Health, Environmental Health and theAmbulance Trust to ensure effective communication and management.METHODOLOGY:<strong>The</strong> Infection Prevention Team (IPT) is responsible for the daily intelligence and datacollection of symptomatic patients/residents, their locations and patient status and foradvising on closure of bays or wards. IPT are required to report to the Health ProtectionAgency West Midlands if outbreaks occur on a weekly or daily report depending onoutbreak activity to enable a regional surveillance system to operate. Occupational Healthand Wellbeing collect staff sickness data. Housekeeping are responsible for coordinatingthe environmental cleaning and environmental decontamination response liaising with theIPT.<strong>The</strong> <strong>Outbreak</strong> Management Committee meets daily to review the overall situation, risks andcoordinate the actions. Preventing admissions to the Acute Trust from community carehomes requires the community outbreak notification and management plan anddehydration clinical pathway for care homes to be operational and managed by the IPT.Communication for the Acute Trust is through a daily press bulletin.GP’s are communicated to via a Public Health cascade system.Care homes with confirmed or suspected outbreaks use an outbreak notification systemand an outbreak management plan/pack which includes an oral hydration plan with 15minute oral fluids being offered to prevent dehydration. This has proved effective with sipspreventing drips. <strong>The</strong> outbreak management plan is supported by IPT and includes analert for possible admissions to hospital.RESULTS:As of June 20<strong>12</strong> there were four <strong>Norovirus</strong> outbreaks in the acute Trust, two of which werecontained to individual wards. <strong>The</strong> outbreaks affected 380 people (219 patients, 161 staff)and lasted for 76 days, on average wards were closed for 6 days. This resulted in a loss of361 bed days for the Trust.<strong>Norovirus</strong> activity in care homes was observed to be slightly higher than in the previousyear. In total there were 24 outbreaks in 20 care homes between 11 th October <strong>2011</strong> and16 th March 20<strong>12</strong>. <strong>The</strong> average length of each outbreak was 10 days.In eleven outbreaks there were either insufficient samples or none were sent to be testedfor <strong>Norovirus</strong>. However the symptoms met the case definition and so these were managedas <strong>Norovirus</strong> and cases subsequently included in this report. <strong>Norovirus</strong> was confirmed in 7of the reported outbreaks. 254 residents and 107 staff were symptomatic over the period,and 827 bed days were lost. <strong>The</strong>re were no admissions reported of residents from<strong>Wolverhampton</strong> care homes being admitted due to dehydration secondary to <strong>Norovirus</strong>activity. Any resident admitted for another condition was isolated at the receivingemergency portal thus reducing significantly the risk of spread.<strong>The</strong> improvement in caring for the residents locally during outbreaks was due to aneducation and training plan/pack for care home staff cascaded out in <strong>2011</strong>-<strong>12</strong>. Educationand guidance in <strong>Norovirus</strong> Management was delivered via the Care Managers Link Groupbefore the start of the winter season and a copy of the <strong>Norovirus</strong> Toolkit was circulated tothe <strong>Wolverhampton</strong> care homes. <strong>The</strong> introduction of a revised outbreak notification and
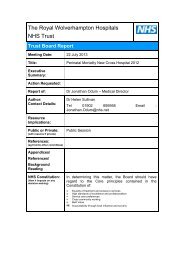
<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS Trustmanagement system that supported care homes throughout a seven day period waslaunched and implemented.Table 1. Monthly <strong>Outbreak</strong> Summary in <strong>Wolverhampton</strong> Community, <strong>2011</strong>-20<strong>12</strong>.Oct<strong>2011</strong>Nov<strong>2011</strong>Dec<strong>2011</strong>Jan20<strong>12</strong>Feb20<strong>12</strong>Mar20<strong>12</strong><strong>2011</strong>-20<strong>12</strong>Residents Affected 3 25 27 49 142 8 254Staff Affected 1 5 10 8 81 2 107Bed Days Lost due to <strong>Outbreak</strong> 6 62 106 238 415 0 827Average <strong>Outbreak</strong> Length 4 11 9 11 11 6 10Longest <strong>Outbreak</strong> - 19 15 14 20 7 20Shortest <strong>Outbreak</strong> - 5 6 7 5 5 5Care Homes <strong>Outbreak</strong>s 1 3 3 4 11 2 24Table 2. Characteristics of each outbreak in <strong>Royal</strong> <strong>Wolverhampton</strong>Hospitals NHS Trust, <strong>2011</strong>-20<strong>12</strong>.Ward D7 Feb 20<strong>12</strong> Apr 20<strong>12</strong> Ward D6 <strong>2011</strong>-<strong>12</strong>Length of <strong>Outbreak</strong> (days) 6 30 25 15 76Start DateEnd Date13-Jan-20<strong>12</strong>19-Jan-20<strong>12</strong>8-Feb-20<strong>12</strong>9-Mar-20<strong>12</strong>30-Mar-20<strong>12</strong>24-Apr -20<strong>12</strong>14-May-20<strong>12</strong>29-May-20<strong>12</strong>Bed Days Lost due to <strong>Outbreak</strong> 35 157 119 50 361Patients Affected 20 <strong>12</strong>5 55 19 219Staff Affected 8 89 63 1 161Staff symptomatic on ward 8 25 31 1 65Visitors Affected - <strong>12</strong> 9 - 21Average Ward <strong>Outbreak</strong> Length 8 8 8Longest Ward <strong>Outbreak</strong> 19 16 19Shortest Ward <strong>Outbreak</strong> 3 3 3Wards Affected 1 <strong>12</strong> 9 1 --An initial outbreak occurred on ward D7, with the first patients exhibiting symptoms ofdiarrhoea and vomiting on 13 th January 20<strong>12</strong>. Figure 1 illustrates the epidemic curve forthis outbreak.
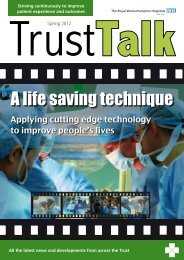
<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS TrustFigure 1. Epidemic curve during Ward D7 outbreak by onset of il lness,January 20<strong>12</strong> (n=28).<strong>The</strong> quick rise in symptomatic patients followed by a gradual reduction in cases ofdiarrhoea and vomiting shown in the outbreak curve is indicative of a single source ofexposure. <strong>The</strong> outbreak lasted 6 days, affected 20 patients and 8 staff, and was containedto a single ward.<strong>Report</strong>s to HPA Laboratory of <strong>Norovirus</strong> infections in England and Wales reveal thatFebruary 20<strong>12</strong> observed the highest level of <strong>Norovirus</strong> activity since January to March2010. During this month the largest outbreak of the year for the Trust occurred, beginningon 8 th February.Figure 2. Epidemic curve during outbreak by date of onset, February toMarch 20<strong>12</strong> (n=214).<strong>The</strong> outbreak lasted for 30 days, with 13 outbreaks over <strong>12</strong> wards ensuing. <strong>12</strong>5 patientswere affected and 25 staff were symptomatic on wards. <strong>The</strong> outbreak was likely to be
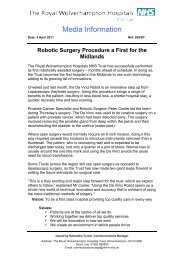
<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS Trustpropagated (person-to-person spread), illustrated by the number of wards involved andseveral peaks on the epidemic curve (Figure 2). This could be explained by staff reportingback to work to early following illness or be due to visitors becoming symptomatic whilstvisiting the hospital and vomiting on site of which there were several reports. <strong>The</strong> outbreakwas declared over on 9 th March 20<strong>12</strong>.Figure 3. Epidemic curve during outbreak by date of onset, March to April20<strong>12</strong> (n=118).Between 30 th March 20<strong>12</strong> and 24 th April 20<strong>12</strong> there was reporting of diarrhoea and vomitingon 9 different wards. This outbreak displayed similar characteristics to its predecessor.Progressively taller peaks in the epidemic curve (Figure 3) illustrates the virus was likelyspread by symptomatic staff and patients throughout the hospital after the index case wasadmitted.For this outbreak a slightly shorter outbreak length of 25 days resulted in 119 beds blockedover the period. 55 patients were affected and 31 staff were symptomatic on wards.<strong>The</strong> onset date of the last outbreak of the year was 14 th May 20<strong>12</strong>, lasting for 15 days until29 th May 20<strong>12</strong>. <strong>The</strong> number of patients with symptoms of diarrhoea and vomiting was 19. Intotal 50 bed days were lost due to blocked beds, but the outbreak was successfullyconfined to one ward.
<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS TrustFigure 4. Epidemic curve during Ward D6 outbreak by onset of illness, May20<strong>12</strong> (n=20).Although the full financial cost of the outbreaks cannot be quantified for the Trust, certaincosts can be reported.Under the National Payment by Results tariff the Trust would receive excess bed dayincome from the PCT if a certain healthcare resource group (HRG) lasts longer than theDepartment of Health expects (in addition to spell income received).<strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals’ excess bed day income for 20<strong>12</strong>-13 is expected to be£235 per bed day. This amount can be used to calculate an estimated loss of income of£84,800 due to the 361 beds closed during the period.Further costs have been incurred from bio-decontamination of areas in the hospital affectedby <strong>Norovirus</strong>. <strong>The</strong> cost of hydrogen peroxide vapour (HPV) has been calculated to beapproximately £35,000 for the period of the outbreaks, excluding staff time.Other indeterminate costs include staff absent from work due to <strong>Norovirus</strong>. 161 staffreported as sick with symptoms during the time period of the outbreaks. Of these, 61 weresymptomatic on wards, which would likely lead to additional costs of ward decontamination.Staff are not allowed to return to clinical areas for at least 48 hours after their symptomscease. This meant that wards may have had to hire bank staff to fill these roles duringabsences.Costs for additional personal protective equipment have been incurred.<strong>The</strong> Infection Prevention Team have sustained an increase in staff expenditure during theoutbreak period attributed to staff being on call at weekends and bank holidays.POST OUTBREAK ANALYSIS<strong>The</strong> root cause analysis investigations and post outbreak analysis identified promptrecognition and reporting of symptomatic patients to the Infection Prevention Team by wardstaff as an area of best practice. It enabled prompt closure of bays or ward areas as acontainment measure and enabled the <strong>Outbreak</strong> Management Committee to meet andcommence a coordinated approach without delay. <strong>The</strong> Infection Prevention Team worked aseven day rota to enable support for staff at the acute site and in care homes to supportstaff to prevent unnecessary admissions through the emergency portals. Communication
<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS Trustwith regards to admissions when they were required and discharges was improved. Thisresulted in an awareness of any pending admissions from care homes due to other medicalconditions and ensured isolation of the symptomatic patient on arrival. <strong>The</strong> AmbulanceTrust were also encouraged to keep any symptomatic patients in the ambulance at theemergency portal whilst an isolation facility was found to prevent spread.<strong>The</strong> Microbiology laboratory does not have the ability to test specimens for <strong>Norovirus</strong> onsite and sending samples away meant delays in confirming the virus. This meant that bayswere closed by infection prevention as a precaution when patients were symptomatic until aresult was available. <strong>The</strong> number of bed days lost was relatively low compared to thenumber of symptomatic patients and areas affected. <strong>The</strong> absence of in house <strong>Norovirus</strong>testing may have resulted in some unnecessary short term closures. <strong>The</strong> need for onsitetesting is a priority.Following discussion it was agreed that there is a need to improve the way outbreak data iscollected and analysed so that more information can be gained from the outbreak.<strong>The</strong> care homes experienced delays in sending stool specimens from symptomaticresidents due to lack of available specimen pots.Occupational Health and Wellbeing reported that staff were not consistently reportingsymptoms or were reporting them late due to the lack of a twenty four hour hotline. Thiswas made a priority and was made operational.<strong>The</strong> action plan appendix 1 details the response to the problems identified and the lessonslearned.RISKS<strong>The</strong> Inability to complete HPV decontamination of affected ward areas due tocapacity pressures means a risk of transmission and longer outbreaks due toinadequate environmental decontamination.An electronic data surveillance system is required to improve data collection andanalysis of trends.<strong>The</strong> lack of the ability to test stool specimens for <strong>Norovirus</strong> on site means that baysor wards may be closed on suspected cases which following testing are found to benegative.
ACTION PLAN: Appendix1<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS TrustRecommendation /SolutionRequests for side-wards tobe assessed as a priorityby the Capacity Teamwhen advised by InfectionPreventionAction Required Lead Officer Priority[H,M,L]All requests forbeds/side-wards andreasons to bedocumented withreasons for requestsso that a riskassessment made bemadeCapacityManagerTimescaleStart Date Target DateHow will thisaction bemonitored?High Immediate May 20<strong>12</strong> Incident reportsCare Homes must continueto be supported byInfection Prevention toreduce the risk ofadmissions due to<strong>Norovirus</strong>Care homes to have5 stool specimenpots for use duringoutbreaksCare homes to havea plan of how to getthe stool specimensto the GP surgery/microbiologyProjectManagerProjectManagerHighMediumImmediateIn place May20<strong>12</strong>In placeMay 20<strong>12</strong>RCA Investigation<strong>Report</strong> to IPCCJune 20<strong>12</strong>RCA investigation<strong>Report</strong> to IPCCCare Homes to beinvited to an updateon <strong>Norovirus</strong>management beforewinter 20<strong>12</strong>-13ProjectManagerMediumAugust 20<strong>12</strong>Quarterly ProjectUpdate report<strong>Report</strong> to IPCC
Onsite testing for <strong>Norovirus</strong>is required<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS TrustOn line testingbusinesscaserequiredMicrobiologyManagerJ.LargeHighMediumApril 20<strong>12</strong>October20<strong>12</strong>September20<strong>12</strong><strong>Report</strong> to IPCCMedical staff to be invitedto be part of the <strong>Outbreak</strong>management team toimprove understanding ofthe outbreak and highlightthe need for prompt patientreview and diagnosis.Sheltered accommodationunits had no informationon <strong>Norovirus</strong> managementBank staff will need to berestricted and not movebetween affected and nonaffectedwards duringoutbreaks.Improve communicationand monitoring of HPVdecontaminationAdd a medicalrepresentative to the<strong>Outbreak</strong>ManagementCommitteemembership via the<strong>Outbreak</strong> PolicyShelteredaccommodation unitsrequire informationon <strong>Norovirus</strong>managementBank staffcoordinator to beadded to theoutbreak committeeminutes circulationlist so thatinformation reachesthe bank staffallocation pointInvestigate thepossible trial of anelectronic processC WileyV WhatleyIPT R. JervisPublic HealthHighMediumImmediateCompletedC. Wiley High Immediate CompletedMay 20<strong>12</strong>S.Roberts Medium May 20<strong>12</strong> August 20<strong>12</strong> IPCC<strong>Outbreak</strong> IP13and <strong>Norovirus</strong>IP18PoliciesrevisedVia minutes ofmeetingsVia minutes ofmeetingsNo analyst available tocollate and analyse dataRecruit an analyst tosupport InfectionV.Whatley High May 20<strong>12</strong> Analyst recruitedand operational
collectionElectronic data surveillancesystem required for datacapture<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS TrustPrevention agendaIC NET outbreakmanagement modulebeing purchasedAugust 20<strong>12</strong>V Whatley High August20<strong>12</strong>IC Net businesscase approved.ICNET modulebeing introducedAugust 20<strong>12</strong>.
<strong>The</strong> <strong>Royal</strong> <strong>Wolverhampton</strong> Hospitals NHS TrustRecommendation in the report:<strong>The</strong> group / committee to consider any risks associated with results / findings of monitoringand whether or not they should be replaced on directorate, divisional or Trust risk register.