Preventing Alcohol-related Harm in Australia - Department of Health
Preventing Alcohol-related Harm in Australia - Department of Health
Preventing Alcohol-related Harm in Australia - Department of Health

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Preventative <strong>Health</strong> TaskforceNational Preventative<strong>Health</strong> TaskforceTechnical Report No 3<strong>Prevent<strong>in</strong>g</strong> <strong>Alcohol</strong>-<strong>related</strong> <strong>Harm</strong> <strong>in</strong> <strong>Australia</strong>:a w<strong>in</strong>dow <strong>of</strong> opportunityPrepared for the National Preventative <strong>Health</strong> Taskforceby the <strong>Alcohol</strong> Work<strong>in</strong>g Group
AcknowledgementsThe technical report on alcohol was prepared on behalf <strong>of</strong>the National Preventative <strong>Health</strong> Taskforce:Pr<strong>of</strong>essor Rob Moodie, ChairPr<strong>of</strong>essor Mike Daube, Deputy ChairMs Kate Carnell AODr Christ<strong>in</strong>e ConnorsMr Shaun Lark<strong>in</strong>Dr Lyn Roberts AMPr<strong>of</strong>essor Leonie SegalDr L<strong>in</strong>da SelveyPr<strong>of</strong>essor Paul Zimmet AOThe report was prepared with advice from the NationalPreventative <strong>Health</strong> Taskforce <strong>Alcohol</strong> Work<strong>in</strong>g Group:Pr<strong>of</strong>essor Rob Moodie (Chair)Pr<strong>of</strong>essor Steve AllsopMs Kate Carnell AOMr David CrosbiePr<strong>of</strong>essor Margaret Hamilton AOMr Todd HarperPr<strong>of</strong>essor Leonie SegalDr L<strong>in</strong>da SelveyAssociate Pr<strong>of</strong>essor Ted WilkesPr<strong>of</strong>essor Paul Zimmet AOWriter: Mr Brian VandenbergWe would also like to thank the follow<strong>in</strong>g people for their contributions to the report:Pr<strong>of</strong>essor Rob<strong>in</strong> Room (Director), and Mr Michael Liv<strong>in</strong>gston, AER Centre for <strong>Alcohol</strong> Policy Researchand Turn<strong>in</strong>g Po<strong>in</strong>t, <strong>Alcohol</strong> & Drug Centre MelbourneMs Meriel Schultz, Adviser, National Preventative <strong>Health</strong> TaskforceMs Michelle Scollo, Senior Adviser, Cancer Council VictoriaThe Population <strong>Health</strong> Strategy Unit and the Publications Unit and Communications Branch,<strong>Australia</strong>n Government <strong>Department</strong> <strong>of</strong> <strong>Health</strong> and Age<strong>in</strong>g
Contents1 Introduction: chang<strong>in</strong>g the dr<strong>in</strong>k<strong>in</strong>g culture <strong>in</strong> <strong>Australia</strong> 11.1 Purpose 11.2 The dr<strong>in</strong>k<strong>in</strong>g culture <strong>in</strong> <strong>Australia</strong> 21.3 Determ<strong>in</strong>ants <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g behaviour 21.4 <strong>Alcohol</strong> policy and programs <strong>in</strong> <strong>Australia</strong> 31.5 Recent developments <strong>in</strong> <strong>Australia</strong> 42 Key trends <strong>in</strong> alcohol consumption 52.1 <strong>Alcohol</strong> consumption <strong>in</strong> <strong>Australia</strong> and other countries 52.2 Dr<strong>in</strong>k<strong>in</strong>g patterns among <strong>Australia</strong>ns 62.3 Product preferences 82.4 <strong>Alcohol</strong> prices and consumer spend<strong>in</strong>g 93 Key trends <strong>in</strong> alcohol-<strong>related</strong> harm 113.1 <strong>Health</strong> impacts 113.2 Social impacts 133.3 <strong>Health</strong> <strong>in</strong>equalities 154 Best practice <strong>in</strong> prevention 174.1 Current activity 174.2 Regulat<strong>in</strong>g the physical availability <strong>of</strong> alcohol 234.3 Taxation and pric<strong>in</strong>g 274.4 Dr<strong>in</strong>k-driv<strong>in</strong>g countermeasures 274.5 Treatment and early <strong>in</strong>tervention 284.6 Alter<strong>in</strong>g the dr<strong>in</strong>k<strong>in</strong>g context 304.7 Regulat<strong>in</strong>g promotion 324.8 Education and persuasion 35ii
5 Policy Imperatives 375.1 The state <strong>of</strong> alcohol policy <strong>in</strong> <strong>Australia</strong> 375.2 The best mix <strong>of</strong> <strong>in</strong>terventions 385.3 Challenges <strong>in</strong> implementation 405.4 Opportunities for action 425.5 Priorities 43References 45iii
1. Introduction:chang<strong>in</strong>g thedr<strong>in</strong>k<strong>in</strong>g culture<strong>in</strong> <strong>Australia</strong>1.1 PurposeThis paper has been prepared for the NationalPreventative <strong>Health</strong> Taskforce to provide upto-dateand evidence-based <strong>in</strong>formation onpolicies and programs to prevent alcohol<strong>related</strong>harm <strong>in</strong> <strong>Australia</strong>. While the paper is<strong>in</strong>tended as an overview <strong>of</strong> the most relevantand generally available evidence, <strong>in</strong> the<strong>in</strong>terests <strong>of</strong> brevity it covers many issues <strong>in</strong>summary only.The paper attempts to answer three questions:nnnWhat are the key trends <strong>in</strong> alcoholconsumption and <strong>related</strong> harm <strong>in</strong> <strong>Australia</strong>?What are the most effective approachesto prevent<strong>in</strong>g and reduc<strong>in</strong>g alcohol<strong>related</strong>harm?What are the gaps and opportunities forpreventative action <strong>in</strong> <strong>Australia</strong>?The paper is <strong>in</strong>formed by the most currentand readily available <strong>in</strong>formation on alcoholconsumption and <strong>related</strong> harm, and thescientific literature on approaches to prevent<strong>in</strong>gand reduc<strong>in</strong>g alcohol-<strong>related</strong> harm. It drawsupon evidence and examples <strong>of</strong> approachesfrom both with<strong>in</strong> <strong>Australia</strong> and <strong>in</strong>ternationally.The paper summarises and acknowledgespreventative work address<strong>in</strong>g alcohol-<strong>related</strong>harm already under way <strong>in</strong> <strong>Australia</strong>, and<strong>in</strong>cludes some commentary on its effectiveness,and also attempts to highlight gaps andopportunities for further preventative action.The range <strong>of</strong> <strong>in</strong>terventions that are reviewed <strong>in</strong>some detail <strong>in</strong> the paper <strong>in</strong>clude:nnnnnnnRegulat<strong>in</strong>g physical availabilityTaxation and pric<strong>in</strong>gDr<strong>in</strong>k-driv<strong>in</strong>g countermeasuresTreatment and early <strong>in</strong>terventionAlter<strong>in</strong>g the dr<strong>in</strong>k<strong>in</strong>g contextRegulat<strong>in</strong>g promotionEducation and persuasion.An emerg<strong>in</strong>g theme from the paper is that thereis currently a unique w<strong>in</strong>dow <strong>of</strong> opportunity <strong>in</strong><strong>Australia</strong> for a significant expansion <strong>of</strong> activity<strong>in</strong> the prevention <strong>of</strong> alcohol-<strong>related</strong> harm. Inpart, this opportunity grows from <strong>in</strong>creasedcommunity and political concern about theharmful consumption <strong>of</strong> alcohol (especiallyfocused on youth dr<strong>in</strong>k<strong>in</strong>g) and a heightenedwill<strong>in</strong>gness from all levels <strong>of</strong> government to takeaction <strong>in</strong> the area.Furthermore, there is an <strong>in</strong>creas<strong>in</strong>gly solid base<strong>of</strong> evidence upon which policy decisions canbe made – even from the brief review presented<strong>in</strong> this paper, it is clear which <strong>of</strong> the variouspolicies and programs hold the most promise <strong>of</strong>be<strong>in</strong>g effective, and those which <strong>of</strong>fer the least.It is also apparent that there are potentialsynergies with other public health efforts toaddress tobacco, obesity and a range <strong>of</strong>chronic diseases.1
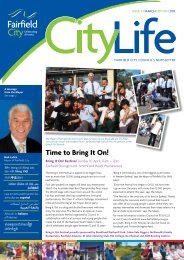
The priorities for preventative action that aresuggested <strong>in</strong> this paper are reflected <strong>in</strong> theoverarch<strong>in</strong>g discussion paper <strong>Australia</strong>: the<strong>Health</strong>iest Country by 2020.1.2 The dr<strong>in</strong>k<strong>in</strong>g culture <strong>in</strong> <strong>Australia</strong><strong>Alcohol</strong> plays many roles <strong>in</strong> contemporary<strong>Australia</strong>n society – as a relaxant, as anaccompaniment to socialis<strong>in</strong>g and celebration,as a source <strong>of</strong> employment and exports, and asa generator <strong>of</strong> tax revenue. It is <strong>in</strong>tr<strong>in</strong>sically part<strong>of</strong> <strong>Australia</strong>n culture. The majority <strong>of</strong> <strong>Australia</strong>nswho regularly dr<strong>in</strong>k, do so <strong>in</strong> moderation.Around three-quarters (72.6%) <strong>of</strong> <strong>Australia</strong>nsdr<strong>in</strong>k below levels for long-term risk <strong>of</strong> harm.[1]However, short-term consumption <strong>of</strong> alcoholat harmful levels, while only occasional, is alsoa prom<strong>in</strong>ent feature <strong>of</strong> the dr<strong>in</strong>k<strong>in</strong>g culture <strong>in</strong><strong>Australia</strong>. One <strong>in</strong> five <strong>Australia</strong>ns (20.4%) dr<strong>in</strong>k atshort-term risky/high-risk levels at least once amonth.[2] Put another way, this equates to morethan 42 million occasions <strong>of</strong> b<strong>in</strong>ge dr<strong>in</strong>k<strong>in</strong>g <strong>in</strong><strong>Australia</strong> each year.While overall levels <strong>of</strong> alcohol consumption anddr<strong>in</strong>k<strong>in</strong>g patterns have not changed markedlyover the past decade, there is an <strong>in</strong>creas<strong>in</strong>gcommunity awareness <strong>of</strong> the problem <strong>of</strong> harmfulconsumption <strong>of</strong> alcohol. These patterns cont<strong>in</strong>ueto produce substantial costs to the health <strong>of</strong><strong>Australia</strong>ns. <strong>Alcohol</strong> consumption accounts for3.2% <strong>of</strong> the total burden <strong>of</strong> disease and <strong>in</strong>jury<strong>in</strong> <strong>Australia</strong>: 4.9% <strong>in</strong> males and 1.6% <strong>in</strong> females.[3] Beyond its impacts on the health andwellbe<strong>in</strong>g <strong>of</strong> <strong>in</strong>dividuals and communities, theharmful consumption <strong>of</strong> alcohol also impactssignificantly across a range <strong>of</strong> other areas,<strong>in</strong>clud<strong>in</strong>g workforce productivity, healthcareservices such as hospitals and ambulances, roadaccidents, law enforcement, property damageand <strong>in</strong>surance adm<strong>in</strong>istration.The annual cost to the <strong>Australia</strong>n communityfrom alcohol-<strong>related</strong> harm is estimated to bemore than $15 billion.[4] In <strong>Australia</strong>, concern<strong>in</strong> the general community about alcohol’sadverse health and social effects is grow<strong>in</strong>g.A recent survey <strong>of</strong> <strong>Australia</strong>ns revealed that 84%<strong>of</strong> people are concerned about the impact <strong>of</strong>alcohol on the community.[5]1.3 Determ<strong>in</strong>ants <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g behaviourThe current national alcohol strategy[6] observesthat <strong>Australia</strong>’s dr<strong>in</strong>k<strong>in</strong>g cultures are drivenby a mix <strong>of</strong> powerful, <strong>in</strong>tangible social forces,such as habits, customs, images and norms,and other <strong>in</strong>terlock<strong>in</strong>g and equally powerfultangible forces relat<strong>in</strong>g to the social, economicand physical availability <strong>of</strong> alcohol, <strong>in</strong>clud<strong>in</strong>gpromotion and market<strong>in</strong>g, age restrictions, price,outlets, hours <strong>of</strong> access and service practices[6](see Fig. 1). Certa<strong>in</strong>ly, there is no s<strong>in</strong>gle factorthat determ<strong>in</strong>es why people dr<strong>in</strong>k at harmfullevels. <strong>Health</strong>-damag<strong>in</strong>g behaviours <strong>related</strong>to poor diet, <strong>in</strong>adequate exercise, cigarettesmok<strong>in</strong>g, excessive dr<strong>in</strong>k<strong>in</strong>g and illicit drug useappear to be embedded <strong>in</strong> a complex network<strong>of</strong> social determ<strong>in</strong>ants and risk and protectivefactors, and behaviours are also mediated bycultural <strong>in</strong>fluences.[7]2
ModifiableDeterm<strong>in</strong>ants:Cultural Place and Availability:• Price• Outlet locations• Open<strong>in</strong>g hours• M<strong>in</strong>imum purchase age• Service practices• Law enforcement• Promotion• Social norms & valuesTargetBahaviours:Dr<strong>in</strong>k<strong>in</strong>g to Intoxication:(BAC > 0.08)Long TermHeavy Dr<strong>in</strong>k<strong>in</strong>gOutcomes:Public Safety and Amenity:• Violence• Property damage• Anti-social behaviour• Perceptions <strong>of</strong> safetyPublic Safety and Amenity:• Road <strong>in</strong>juries• Assaults• Drown<strong>in</strong>g• Suicides• Falls• Fire/smoke <strong>in</strong>juries• Sexually transmitted<strong>in</strong>fectionsLong-term (Chronic)<strong>Health</strong> Impacts:• Cancers• Cirrhosis <strong>of</strong> the liver• Dependence• Mental IllnessFigure 1: <strong>Alcohol</strong>-<strong>related</strong> harm: determ<strong>in</strong>ants, behaviours and outcomesSource: National <strong>Alcohol</strong> Strategy 2006–2009[6]1.4 <strong>Alcohol</strong> policy andprograms <strong>in</strong> <strong>Australia</strong>nSupport whole-<strong>of</strong>-community <strong>in</strong>itiatives toreduce alcohol-<strong>related</strong> health problems<strong>Prevent<strong>in</strong>g</strong> alcohol-<strong>related</strong> harm is a responsibilityshared among all levels <strong>of</strong> government. The<strong>Australia</strong>n Government and the states andterritories are work<strong>in</strong>g together through themechanisms <strong>of</strong> the M<strong>in</strong>isterial Council onDrug Strategy to implement <strong>in</strong>itiatives as part<strong>of</strong> the National <strong>Alcohol</strong> Strategy 2006–2009.[6] The strategy is a plan for action developedcollaboratively between governments, <strong>in</strong>dustryand community partners. Key action areas<strong>in</strong>itially identified for the strategy <strong>in</strong>clude:nnnMonitor and review <strong>of</strong> alcohol promotionsIncrease community awareness andunderstand<strong>in</strong>g <strong>of</strong> the extent and impacts<strong>of</strong> <strong>in</strong>toxicationImprove enforcement <strong>of</strong> liquorlicens<strong>in</strong>g regulationsnDevelop and implement socialmarket<strong>in</strong>g campaigns to reducealcohol-<strong>related</strong> harms.At a state and territory level, key alcohol policyand program responsibilities <strong>in</strong>clude lawenforcement, licens<strong>in</strong>g regulation, the provision<strong>of</strong> treatment services and drug education <strong>in</strong>schools. Additionally, all states and territorieshave strategic plans to address alcohol, whichvary <strong>in</strong> scope and fund<strong>in</strong>g. Given the diverserange <strong>of</strong> adverse outcomes <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g <strong>of</strong>tenexperienced at a local community level,local governments also play an importantrole, <strong>in</strong>clud<strong>in</strong>g their functions <strong>in</strong> environmentalhealth, plann<strong>in</strong>g, community development,waste disposal and youth services.3
Local governments can contribute to themanagement <strong>of</strong> the physical availability <strong>of</strong>alcohol and the creation <strong>of</strong> safer dr<strong>in</strong>k<strong>in</strong>gsett<strong>in</strong>gs, and engage <strong>in</strong> environmental designand plann<strong>in</strong>g that contributes to and supportscommunity wellbe<strong>in</strong>g. There are many examples<strong>of</strong> <strong>in</strong>novative, locally responsive measures <strong>in</strong><strong>Australia</strong>, <strong>in</strong> part to respond to the modernphenomena <strong>of</strong> ‘night-time economies’.[8]Throughout <strong>Australia</strong>, there is also aconsiderable amount <strong>of</strong> community-basedactivity under way <strong>in</strong> prevent<strong>in</strong>g alcohol-<strong>related</strong>harm, some <strong>of</strong> which is government fundedand some <strong>of</strong> which is led by charitable groups.The contribution <strong>of</strong> community-level actionis significant, and is <strong>in</strong>tegral to the effectiveimplementation <strong>of</strong> federal, state and localgovernment polices and programs.Overall, while rhetoric is aimed at prevention,and there is currently a mood to address thenegative side <strong>of</strong> alcohol use, there is greatdifficulty <strong>in</strong> ga<strong>in</strong><strong>in</strong>g coherent, cooperative,strategic and effective action. This situationmight be compared to the place <strong>of</strong> andresponses to tobacco smok<strong>in</strong>g <strong>in</strong> <strong>Australia</strong><strong>in</strong> the 1960s.1.5 Recent developments <strong>in</strong> <strong>Australia</strong>National B<strong>in</strong>ge Dr<strong>in</strong>k<strong>in</strong>g StrategyOn 28 March 2008, the Prime M<strong>in</strong>isterannounced a new national strategy to addressthe b<strong>in</strong>ge dr<strong>in</strong>k<strong>in</strong>g epidemic among young<strong>Australia</strong>ns.[9]Council <strong>of</strong> <strong>Australia</strong>n Governments(COAG) B<strong>in</strong>ge Dr<strong>in</strong>k<strong>in</strong>g AgreementThe Council <strong>of</strong> <strong>Australia</strong>n Governments (COAG)recently agreed on the importance <strong>of</strong> tackl<strong>in</strong>gthe harmful consumption <strong>of</strong> alcohol amongyoung people and asked the M<strong>in</strong>isterialCouncil on Drug Strategy to report to it <strong>in</strong>December 2008 on options to reduce b<strong>in</strong>gedr<strong>in</strong>k<strong>in</strong>g, <strong>in</strong>clud<strong>in</strong>g <strong>in</strong> relation to clos<strong>in</strong>g hours,the responsible service <strong>of</strong> alcohol, recklesssecondary supply and the alcohol content<strong>in</strong> ready-to-dr<strong>in</strong>k beverages. The <strong>Australia</strong>New Zealand Food Regulation M<strong>in</strong>isterialCouncil is to request Food Standards <strong>Australia</strong>New Zealand to consider mandatory healthwarn<strong>in</strong>gs on packaged alcohol.[10]M<strong>in</strong>isterial Council onDrug Strategy (MCDS)The work <strong>of</strong> the M<strong>in</strong>isterial Council on DrugStrategy (MCDS) <strong>in</strong>cludes a focus on theassessment <strong>of</strong> late-night lock-outs for licensedpremises and the development <strong>of</strong> a preferredframework to more effectively target policeresources on b<strong>in</strong>ge dr<strong>in</strong>k<strong>in</strong>g hot spots. It is als<strong>of</strong>ocused on a national policy framework forthe responsible service <strong>of</strong> alcohol, a preferredregulatory model to address the secondarysupply <strong>of</strong> alcohol to m<strong>in</strong>ors, options for reduc<strong>in</strong>gthe alcohol content <strong>in</strong> products (<strong>in</strong>clud<strong>in</strong>g thoseaimed at young people), possible standards andcontrols for alcohol advertis<strong>in</strong>g target<strong>in</strong>g youngpeople, and advice regard<strong>in</strong>g the impact <strong>of</strong>health warn<strong>in</strong>gs on alcohol products.[11]Northern Territory <strong>in</strong>itiative and otherAborig<strong>in</strong>al and Torres Strait Islanderspecific <strong>in</strong>itiativesPerhaps the most radical experiments <strong>in</strong>respond<strong>in</strong>g to problems, especially amongAborig<strong>in</strong>al <strong>Australia</strong>ns, have been carried out<strong>in</strong> the Northern Territory. Most recently, theNorthern Territory Initiative was implementedby the then M<strong>in</strong>ister for Aborig<strong>in</strong>al Affairs <strong>of</strong> theprevious <strong>Australia</strong>n government, and is soon tobe reviewed after one year <strong>of</strong> implementation.This is a complex area and this paper will notattempt to summarise <strong>in</strong>terventions specific toIndigenous <strong>Australia</strong>ns or presume to providecomprehensive <strong>in</strong>formation <strong>in</strong> this area.4
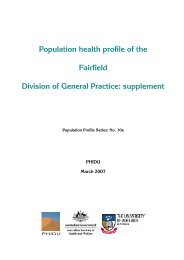
2. Key trends <strong>in</strong> alcoholconsumption2.1 <strong>Alcohol</strong> consumption <strong>in</strong> <strong>Australia</strong>and other countriesInformation on levels and patterns <strong>of</strong> alcoholconsumption is diverse, and it can be difficultto identify the key features for the purposes <strong>of</strong>monitor<strong>in</strong>g trends <strong>in</strong> dr<strong>in</strong>k<strong>in</strong>g and <strong>related</strong> harm,and the possible opportunities for <strong>in</strong>tervention.Unfortunately, <strong>in</strong> <strong>Australia</strong> at the current time,some <strong>of</strong> the most significant and valuable datais not readily available to the public health field.[12] For example, alcohol sales data, while it isknown to be collected and analysed by thealcohol beverage <strong>in</strong>dustry, is not available forthe purposes <strong>of</strong> this paper, nor <strong>in</strong>deed is it easilyaccessed for public health research purposes <strong>in</strong>general. The Taskforce notes with some concernthat the cont<strong>in</strong>uation <strong>of</strong> the most accessibledata sets on alcohol consumption levels <strong>in</strong><strong>Australia</strong>, collected and compiled by the<strong>Australia</strong>n Bureau <strong>of</strong> Statistics (ABS), is currentlyunder review. Efforts are therefore urgentlyrequired to seek the cont<strong>in</strong>uation <strong>of</strong> thesevaluable data sets.Per capita consumption <strong>of</strong> alcohol is animportant measure from a public healthperspective because it is ‘to a considerableextent, <strong>related</strong> to the prevalence <strong>of</strong> heavyuse, which <strong>in</strong> turn is associated with negativeeffects’.[13] Total per capita consumption <strong>of</strong>alcohol <strong>in</strong> <strong>Australia</strong> alcohol grew rapidly <strong>in</strong> the1970s and has not returned to low levels s<strong>in</strong>cethen; <strong>in</strong> 2007 it was estimated to be 9.88 litres<strong>of</strong> alcohol per capita (see Fig. 2). Among thedifferent alcoholic beverage categories, therehave been significant changes <strong>in</strong> per capitaconsumption over the past 70 years. S<strong>in</strong>cepeak<strong>in</strong>g at over 6.4 litres <strong>of</strong> alcohol per capita<strong>in</strong> the mid-1970s, per capita consumption<strong>of</strong> beer has steadily decl<strong>in</strong>ed and is now ata level similar to that <strong>of</strong> the late 1950s.This reduction partly reflects changes <strong>in</strong>consumer tastes towards w<strong>in</strong>e, and the <strong>in</strong>crease<strong>in</strong> the availability <strong>of</strong> relatively low-priced w<strong>in</strong>e.Consumption <strong>of</strong> w<strong>in</strong>e has <strong>in</strong>creased almostfourfold s<strong>in</strong>ce the late 1940s, when <strong>in</strong>take was0.77 litres <strong>of</strong> alcohol per capita. In 2005 w<strong>in</strong>econsumption <strong>in</strong> <strong>Australia</strong> reached an all timerecord <strong>of</strong> 3.13 litres <strong>of</strong> alcohol per capita. When<strong>in</strong>terpret<strong>in</strong>g the trend <strong>in</strong> per capita consumption<strong>in</strong> <strong>Australia</strong>, it should be noted that the datadoes not take <strong>in</strong>to account the age<strong>in</strong>g <strong>of</strong> thepopulation; as people age, they generallyconsume less alcohol. Hence, as the <strong>Australia</strong>npopulation cont<strong>in</strong>ues to age over the com<strong>in</strong>gdecades, it is expected that per capita alcoholconsumption will most likely decrease.Figure 2: Apparent per capita consumption <strong>of</strong> alcohol (litres <strong>of</strong>alcohol), <strong>Australia</strong>n persons aged 15+ years, 1994 to 2007 (yearsend<strong>in</strong>g 30 June)Source: ABS unpublished data and ABS 2008Per capita consumption <strong>of</strong> alcohol <strong>in</strong> <strong>Australia</strong> ishigh by world standards. <strong>Australia</strong> is ranked with<strong>in</strong>the top 30 highest alcohol-consum<strong>in</strong>g nations, out<strong>of</strong> a total <strong>of</strong> 180 countries. Table 1 shows <strong>Australia</strong>’slevel <strong>of</strong> per capita alcohol consumption (9.02 litres<strong>of</strong> pure alcohol) and rank<strong>in</strong>g (#30) comparedto other selected countries <strong>in</strong> 2003. More recentestimates <strong>of</strong> per capita alcohol consumptionfor <strong>Australia</strong> (9.88 litres <strong>of</strong> pure alcohol <strong>in</strong> 2007)suggest that our <strong>in</strong>ternational rank<strong>in</strong>g is now likelyto be even higher.5
Table 1: Per capita consumption <strong>of</strong> alcohol by country and rank (out <strong>of</strong> 180 countries),selected countries*RankCountryPer capitaconsumption † Rank CountryPer capitaconsumption †1 Luxembourg 15.56 31 Greece 9.012 Ireland 13.69 33 USA 8.617 Germany 11.99 37 Italy 8.028 UK 11.75 42 Japan 7.5910 Spa<strong>in</strong> 11.68 52 South Africa 6.7214 France 11.43 63 Sweden 5.9620 Russian Federation 10.32 70 Thailand 5.5923 Netherlands 9.68 74 Ch<strong>in</strong>a 5.2024 New Zealand 9.68 120 Papua New Gu<strong>in</strong>ea 1.6230 <strong>Australia</strong> 9.02 168 Indonesia 0.09* Values are for various years before and <strong>in</strong>clud<strong>in</strong>g 2003† Per capita alcohol consumption (litres <strong>of</strong> pure alcohol) among adultsSource: WHO 2008[14]2.2 Dr<strong>in</strong>k<strong>in</strong>g patternsamong <strong>Australia</strong>nsIt is estimated that 83% <strong>of</strong> <strong>Australia</strong>ns aredr<strong>in</strong>kers, and that 1.4 million <strong>Australia</strong>nsconsume alcohol on a daily basis.[2] In 2007,males (10.8%) were almost twice as likely asfemales (5.5%) to dr<strong>in</strong>k daily.Two <strong>in</strong> every five <strong>Australia</strong>ns dr<strong>in</strong>k on a weeklybasis. However, there is a sizable proportion<strong>of</strong> the population (10.1% <strong>in</strong> 2007) who, forvarious reasons, have never drunk any alcohol(see Table 2).Table 2: Frequency <strong>of</strong> alcohol consumption, proportion <strong>of</strong> the population aged 14+ years,<strong>Australia</strong>, 1991 to 2007Frequency 1991 1993 1995 1998 2001 2004 2007Daily 10.2 8.5 8.8 8.5 8.3 8.9 8.1Weekly 41.0 39.9 35.2 40.1 39.5 41.2 41.3Less 30.4 29.5 34.3 31.9 34.6 33.5 33.5Ex-dr<strong>in</strong>ker 12.0 9.0 9.5 10.0 8.0 7.1 7.0Never 6.5 13.0 12.2 9.4 9.6 9.3 10.1Source: AIHW, National Drug Strategy Household Surveys,[2] various yearsAlmost three-quarters (72.6%) <strong>of</strong> <strong>Australia</strong>nsdr<strong>in</strong>k below levels that would <strong>in</strong>cur long-termrisk <strong>of</strong> harm. However, among young adults(aged 20–29 years), the prevalence <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>gat levels pos<strong>in</strong>g long-term risk <strong>of</strong> harm issignificantly higher (16%) than among otherage groups (see Fig. 3).This pattern <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g is the equivalent <strong>of</strong>consum<strong>in</strong>g 29 or more standard dr<strong>in</strong>ks per weekfor males and 15 or more standard dr<strong>in</strong>ks perweek for females. Among <strong>Australia</strong>n teenagers<strong>in</strong> 2007, this dr<strong>in</strong>k<strong>in</strong>g pattern was considerablyhigher among females (10.6%) than amongmales (7%).6
Figure 3: Dr<strong>in</strong>k<strong>in</strong>g at risky/high risk <strong>of</strong> harm <strong>in</strong> thelong term by age and year, proportion <strong>of</strong> thepopulation aged 14+ years, <strong>Australia</strong>, 2007Source: AIHW National Drug Strategy Household Survey[2]While almost half (48.3%) <strong>of</strong> the <strong>Australia</strong>npopulation dr<strong>in</strong>k at low risk levels, one <strong>in</strong> five<strong>Australia</strong>ns (20.4%) dr<strong>in</strong>k at short-term risky/highrisklevels at least once a month. This pattern <strong>of</strong>dr<strong>in</strong>k<strong>in</strong>g is the equivalent <strong>of</strong> consum<strong>in</strong>g seven ormore standard dr<strong>in</strong>ks on any one day for males,and consum<strong>in</strong>g five or more standard dr<strong>in</strong>ks onany one day for females. In short, this generallyequates to dr<strong>in</strong>k<strong>in</strong>g to the po<strong>in</strong>t <strong>of</strong> <strong>in</strong>toxication,or what is <strong>of</strong>ten termed as ‘b<strong>in</strong>ge dr<strong>in</strong>k<strong>in</strong>g’.This sort <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g is most prevalent amongadults aged 20–29 years, one-quarter (24.9%) <strong>of</strong>whom do so on at least a monthly basis. Overall,<strong>Australia</strong>n males are more likely than femalesto dr<strong>in</strong>k at short-term risky/high-risk levels onregular (at least once a month) occasions(17.1% <strong>of</strong> females compared to 23.6% <strong>of</strong> males).However, among teenagers, females are morelikely than males to regularly dr<strong>in</strong>k at levels <strong>of</strong>risky/high-risk <strong>of</strong> harm <strong>in</strong> the short term: 28.3% <strong>of</strong>female teenagers compared to 24.5% <strong>of</strong> maleteenagers (see Figs. 4 and 5). Between 2001and 2007 there were only slight changes <strong>in</strong> theprevalence <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g at risky/high risk <strong>of</strong> harm<strong>in</strong> the short term across the age groups.Figure 4: Monthly dr<strong>in</strong>k<strong>in</strong>g at risky/high risk<strong>of</strong> harm <strong>in</strong> the short term* by age and year,proportion <strong>of</strong> the male population aged 14+years, 2001 to 2007Source: AIHW National Drug Strategy Household Survey[2]Figure 5: Monthly dr<strong>in</strong>k<strong>in</strong>g at risky/high risk<strong>of</strong> harm <strong>in</strong> the short term* by age and year,proportion <strong>of</strong> the female population aged 14+years, 2001 to 2007Source: AIHW National Drug Strategy Household Survey[2](*Risky/high-risk dr<strong>in</strong>k<strong>in</strong>g <strong>in</strong> the short term =seven or more standard dr<strong>in</strong>ks on any one dayfor males; five or more standard dr<strong>in</strong>ks on anyone day for females.)7
2.3 Product preferencesThe most preferred types <strong>of</strong> alcoholicbeverages among <strong>Australia</strong>n female dr<strong>in</strong>kers,<strong>in</strong> descend<strong>in</strong>g order, are bottled w<strong>in</strong>e, bottledspirits and liqueurs, ready-to-dr<strong>in</strong>k beverages(RTDs) <strong>in</strong> a bottle and RTDs <strong>in</strong> a can. Over the2001 to 2007 period, the preference for bottledw<strong>in</strong>e had the greatest <strong>in</strong>crease among females,grow<strong>in</strong>g from 57.3% to 63.8%. Among males, themost preferred types <strong>of</strong> alcoholic beverages,<strong>in</strong> descend<strong>in</strong>g order, are full-strength beer,bottled w<strong>in</strong>e, bottled spirits and liqueurs, andRTDs <strong>in</strong> a can. Over the 2001 to 2007 period, thepreference for RTDs <strong>in</strong> a can had the greatest<strong>in</strong>crease among males, grow<strong>in</strong>g from 18.2% to24.3% (see Figs. 9 and 10).With regard to which types <strong>of</strong> alcoholicbeverages are most commonly <strong>in</strong>volved <strong>in</strong>the harmful consumption <strong>of</strong> alcohol, Stockwellet al. have estimated[16] that straight spirits(79.7%), alcoholic cider (78.9%), pre-mixed spirits(71.8%) and regular strength beer (72.6%) arethe top four types <strong>of</strong> beverages consumed by<strong>Australia</strong>n dr<strong>in</strong>kers on days when they drank atrisky/high-risk levels. Among 12- to 17-year-olds,the top three types <strong>of</strong> beverages are straightspirits (98.9%), regular beer (78.9%) and RTDs(76.7%). Spirit-based beverages held the highestmarket share, represent<strong>in</strong>g 62.7% <strong>of</strong> total alcoholconsumption among this age group, with slightlymore consumed as straight spirits than as RTDs.Figure 9: Preference for selected alcoholicbeverages by year, proportion <strong>of</strong> the malepopulation, <strong>Australia</strong>, 2001 to 2007Source: AIHW[15]Figure 10: Preference for selected alcoholicbeverages by year, proportion <strong>of</strong> the femalepopulation, <strong>Australia</strong>, 2001 to 2007Source: AIHW[15]8
2.4 <strong>Alcohol</strong> prices andconsumer spend<strong>in</strong>gThe real price <strong>of</strong> alcohol <strong>in</strong> <strong>Australia</strong> hasrema<strong>in</strong>ed relatively low compared to othercommodities, and <strong>in</strong> some cases has dropped.For example, a glass <strong>of</strong> w<strong>in</strong>e cost<strong>in</strong>g $1 <strong>in</strong> June1999 dropped <strong>in</strong> real terms to $0.90 <strong>in</strong> March2008 (see Fig. 6).The affordability <strong>of</strong> alcohol <strong>in</strong> <strong>Australia</strong> today isreflected <strong>in</strong> the fact that, on average, <strong>Australia</strong>nhouseholds are spend<strong>in</strong>g proportionatelyless on alcohol nowadays compared to theamount they spent 20 years ago, despite totalper capita consumption <strong>of</strong> alcohol chang<strong>in</strong>glittle over the same period. The proportion <strong>of</strong>average weekly expenditure by <strong>Australia</strong>nhouseholds on alcoholic beverages <strong>in</strong> 1984was 3.4% ($12.30), compared to 2.6% ($23.32) <strong>in</strong>2003–2004 (ABS 2005).[17]Figure 6: Prices <strong>of</strong> alcoholic beverages relativeto other consumption (June 1999 $1.00),<strong>Australia</strong>, September 1980 to March 2008Source: ABS, various years9
3. Key trends <strong>in</strong> alcohol<strong>related</strong>harm3.1 <strong>Health</strong> impactsIt is important to consider both the shorttermand long-term health impacts <strong>of</strong> theharmful consumption <strong>of</strong> alcohol, as bothresult <strong>in</strong> significant morbidity and mortality.The typical effects <strong>of</strong> moderate alcoholconsumption are those on the bra<strong>in</strong>, suchas feel<strong>in</strong>gs <strong>of</strong> relaxation, wellbe<strong>in</strong>g and loss<strong>of</strong> <strong>in</strong>hibitions. However, as <strong>in</strong>take <strong>in</strong>creases,pleasant effects are lessened by adverseeffects such as drows<strong>in</strong>ess, loss <strong>of</strong> balance,nausea and vomit<strong>in</strong>g, and other more seriousharmful effects such as aggressive behaviours,unconsciousness, kidney failure and <strong>in</strong>creasedrisk <strong>of</strong> accidents and <strong>in</strong>jury [18]. Overall, morepeople die from the acute effects <strong>of</strong> alcoholthan the long-term or chronic effects.[18]<strong>Alcohol</strong> consumption accounts for 3.2% <strong>of</strong> thetotal burden <strong>of</strong> disease and <strong>in</strong>jury <strong>in</strong> <strong>Australia</strong>:4.9% <strong>in</strong> males and 1.6% <strong>in</strong> females.[19]It should be noted that although thispercentage is lower than the contributionfrom tobacco smok<strong>in</strong>g (7.8%) and high bodymass (7.5%), there rema<strong>in</strong>s some debate overthe method to calculate the disease burdenattributable to alcohol. That the <strong>Australia</strong>nfigure may be an underestimate is suggestedby the higher reported burden <strong>of</strong> disease fromalcohol for New Zealand (10% for men and 4%for women).[20]<strong>Alcohol</strong> has been causally l<strong>in</strong>ked to more than60 different medical conditions.[13] In <strong>Australia</strong>,alcohol was l<strong>in</strong>ked to 3430 deaths per year and85,435 disability-adjusted life years (DALYs) peryear.[3]In the 10 years between 1992 and 2001, morethan 31,000 <strong>Australia</strong>ns died from alcoholattributable<strong>in</strong>jury and disease – a greaternumber died from acute (usually <strong>in</strong> the context<strong>of</strong> acute <strong>in</strong>toxication) rather than chronicconditions (<strong>of</strong>ten <strong>related</strong> to longer termdependence on alcohol).Table 3: Deaths and burden (DALYs) attributable to alcohol by specific cause, <strong>Australia</strong>, 2003Specific causeNumberDeathsProportion <strong>of</strong>total (%)NumberDALYsProportion<strong>of</strong> total (%)<strong>Alcohol</strong> abuse 918 0.7% 34,116 1.3%Suicides & self-<strong>in</strong>flicted <strong>in</strong>juries 553 0.4% 12,245 0.5%Road traffic accidents 396 0.3% 11,121 0.4%Oesophagus cancer 368 0.3% 4,594 0.2%Breast cancer 184 0.1% 4,152 0.2%Other 1,012 0.8% 19,207 0.7%Total harm 3,430 2.6% 85,435 3.2%Source: Begg et al. 2005The most common cause <strong>of</strong> death due to<strong>in</strong>toxication was road crash <strong>in</strong>jury, and amongthe chronic conditions alcohol-<strong>related</strong> livercirrhosis accounted for the majority <strong>of</strong> deaths.[21]Deaths from acute causes are most commonamong young people, particularly thoseaged 15–29 years, while deaths from alcoholattributablechronic diseases are morecommon among people aged over 45 years.11
More males than females died from both acuteand chronic alcohol-attributable conditions [21.]Over half a million hospitalisations were causedby risky and high-risk dr<strong>in</strong>k<strong>in</strong>g <strong>in</strong> <strong>Australia</strong> <strong>in</strong> theeight years between 1993/94 and 2000/01.[21]The most numerous conditions among thesehospitalisations were for alcohol dependence(87,186), <strong>in</strong>juries caused by assault (76,115), roadcrash <strong>in</strong>juries (47,167) and attempted suicide(20,374). As many as 10,094 hospitalisations wereattributed to some form <strong>of</strong> ‘alcoholic overdose’from very high blood alcohol levels, <strong>in</strong>clud<strong>in</strong>galcohol poison<strong>in</strong>g and aspiration vomitus.Overall, the majority <strong>of</strong> hospitalisations were foracute conditions (67.8%).[21]Future projections <strong>of</strong> the lead<strong>in</strong>g causes <strong>of</strong>disease burden predict that the proportiondue to alcohol will rema<strong>in</strong> stable and with<strong>in</strong> thetop 14 lead<strong>in</strong>g causes among <strong>Australia</strong>n malesby 2023 (see Fig. 7). The proportion <strong>of</strong> diseaseburden caused by anxiety and depression isalso expected to rema<strong>in</strong> stable by 2023, whileischaemic heart disease and lung cancerare expected to decl<strong>in</strong>e. Type 2 diabetes ispredicted to be the lead<strong>in</strong>g cause <strong>of</strong> diseaseburden among <strong>Australia</strong>n males by 2023.Figure 7: Lead<strong>in</strong>g causes <strong>of</strong> burden (DALYs) <strong>in</strong>males, <strong>Australia</strong>, 1993 to 2023Source: Begg et al. 2007[19]At low levels <strong>of</strong> consumption, alcohol mayalso have some benefits – various studieshave found reductions <strong>in</strong> some forms <strong>of</strong> heartdisease (particularly <strong>in</strong> middle-aged and oldermales) and ischaemic stroke (<strong>in</strong> older females),diabetes, gallstones and dementia.The extent and even the existence <strong>of</strong> suchbenefits rema<strong>in</strong> controversial.[22, 23] In terms <strong>of</strong>population, health, heart disease and stroke arethe most important <strong>of</strong> these potential benefits.Nearly all the potential benefits are conf<strong>in</strong>edto males over the age <strong>of</strong> 45 and women pastmenopause, and can be ga<strong>in</strong>ed with a dr<strong>in</strong>k<strong>in</strong>gpattern <strong>of</strong> as little as one dr<strong>in</strong>k every secondday. S<strong>in</strong>ce alternative means <strong>of</strong> prevent<strong>in</strong>gheart and vascular disease are available, thecl<strong>in</strong>ical consensus is that people need not takeup or ma<strong>in</strong>ta<strong>in</strong> dr<strong>in</strong>k<strong>in</strong>g for health benefits.Dr<strong>in</strong>k<strong>in</strong>g dur<strong>in</strong>g pregnancyRecent data show that 59% <strong>of</strong> <strong>Australia</strong>nwomen drank alcohol at some time dur<strong>in</strong>gtheir pregnancy and that 14% reporteddr<strong>in</strong>k<strong>in</strong>g five or more dr<strong>in</strong>ks <strong>in</strong> a sitt<strong>in</strong>g <strong>in</strong>the three months prior to pregnancy – 58%dur<strong>in</strong>g the first and second trimester and54% <strong>in</strong> the third trimester.[18] Maternalalcohol consumption can result <strong>in</strong> aspectrum <strong>of</strong> harms to the fetus. Althoughthe risk <strong>of</strong> birth defects is greatest with high,frequent maternal alcohol <strong>in</strong>take dur<strong>in</strong>g thefirst trimester, alcohol exposure throughoutpregnancy (<strong>in</strong>clud<strong>in</strong>g before a pregnancy isconfirmed) can have consequences for thedevelopment <strong>of</strong> the fetal bra<strong>in</strong>. It is not clearwhether the effects <strong>of</strong> alcohol are <strong>related</strong>to the dose <strong>of</strong> alcohol and whether thereis a threshold above which adverse effectsoccur.[24] This uncerta<strong>in</strong>ty is reflected <strong>in</strong>policy regard<strong>in</strong>g alcohol use <strong>in</strong> pregnancywith<strong>in</strong> <strong>Australia</strong> and overseas.[25] Althoughthe risks from low-level dr<strong>in</strong>k<strong>in</strong>g (such as oneor two dr<strong>in</strong>ks per week) dur<strong>in</strong>g pregnancyare likely to be low, a ‘no-effect’ level hasnot been established, and limitations <strong>in</strong> theavailable evidence make it impossible toset a ‘safe’ or ‘no-risk’ dr<strong>in</strong>k<strong>in</strong>g level forwomen to follow <strong>in</strong> order to avoid caus<strong>in</strong>gharm to their unborn baby.12
In 2005–2006 there were a total <strong>of</strong> 145,000drug treatment episodes recorded <strong>in</strong> <strong>Australia</strong>,<strong>of</strong> which 56,000 (or 39%) were for alcoholproblems.[15] While this figure is high, it isperhaps relatively low given the estimated585,000 <strong>Australia</strong>ns who dr<strong>in</strong>k at levelsconsidered to be high risk to health <strong>in</strong> thelong term, many whom might be consideredthe potential target group for treatment.[15]Females accounted for 31% <strong>of</strong> alcoholtreatment episodes <strong>in</strong> 2005–2006. Personsaged 20–29 years received 22% <strong>of</strong> treatmentepisodes. For persons aged 10–19 yearsreceiv<strong>in</strong>g treatment, the proportion treatedfor alcohol problems has <strong>in</strong>creased from 15%to 23% between 2001–2002 and 2005–2006.The <strong>in</strong>teractions between other drugs(tobacco, illicit and prescription) and alcoholare complex. <strong>Australia</strong>n studies reveal a closeassociation between hero<strong>in</strong> overdose andalcohol consumption at harmful levels at thetime <strong>of</strong> overdose. <strong>Australia</strong>n research has als<strong>of</strong>ound that among cannabis users, alcohol wasalmost universally used on a regular basis, withmost users consum<strong>in</strong>g alcohol at harmful levels.There are also parallels <strong>in</strong> aetiological researchregard<strong>in</strong>g the uptake <strong>of</strong> one psycho-activesubstance <strong>in</strong>creas<strong>in</strong>g the likelihood <strong>of</strong> use <strong>of</strong>others. There has also been some work doneregard<strong>in</strong>g parents’ attitudes and behaviour asa factor <strong>in</strong> <strong>in</strong>fluenc<strong>in</strong>g tobacco, alcohol andother drug use. For all <strong>of</strong> these substances, itis important that prevention efforts focus ondelay<strong>in</strong>g the uptake <strong>of</strong> regular use. This paperdoes not attempt to deal with the obviouscrossover between mental health issues andthe harmful consumption <strong>of</strong> alcohol, and the<strong>in</strong>creas<strong>in</strong>g problem <strong>of</strong> poly-drug use, but anypreventative action needs to bear these factors<strong>in</strong> m<strong>in</strong>d.3.2 Social impactsThe effects <strong>of</strong> alcohol consumption go beyonddiseases, accidents and <strong>in</strong>juries to a range<strong>of</strong> adverse social consequences, both forthe dr<strong>in</strong>ker and for others <strong>in</strong> the community.These consequences <strong>in</strong>clude harm to familymembers (<strong>in</strong>clud<strong>in</strong>g children) and to friendsand workmates, as well as to bystanders andstrangers. <strong>Alcohol</strong>-<strong>related</strong> disturbance andassault ranges from acts <strong>of</strong> vandalism, <strong>of</strong>fensivebehaviour and disruption to far more seriousantisocial behaviour, which can result <strong>in</strong>violence or <strong>in</strong>jury to others.[18,23] While it isnot a perfect description <strong>of</strong> the wider socialimpacts <strong>of</strong> the harmful consumption <strong>of</strong> alcohol,some commentators have co<strong>in</strong>ed the term‘passive dr<strong>in</strong>k<strong>in</strong>g’, ak<strong>in</strong> to passive smok<strong>in</strong>g, torefer to the impact <strong>of</strong> drunken behaviour onthird parties.13
Families and childrenIt is a reality that the most visible effects<strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g on others, <strong>in</strong>clud<strong>in</strong>g children,result from accidents and <strong>in</strong>jury(<strong>in</strong>clud<strong>in</strong>g violence) dur<strong>in</strong>g or afterdr<strong>in</strong>k<strong>in</strong>g occasions.[18, 23) When familieshave to deal with a relative’s alcoholism,violence, <strong>in</strong>jury or even death, theseserious consequences can cause greatsuffer<strong>in</strong>g.[18, 30) Dr<strong>in</strong>k<strong>in</strong>g with<strong>in</strong> familiesis an important consideration because,depend<strong>in</strong>g upon the circumstances, it canbe either a positive or negative <strong>in</strong>fluenceon the dr<strong>in</strong>k<strong>in</strong>g behaviour <strong>of</strong> young people.It is estimated that 13% <strong>of</strong> <strong>Australia</strong>nchildren aged twelve years or less areexposed to an adult who is a regular b<strong>in</strong>gedr<strong>in</strong>ker.[26] It has been estimated that 31%<strong>of</strong> parents <strong>in</strong>volved <strong>in</strong> substantiated cases<strong>of</strong> child abuse or neglect experiencesignificant problems with alcohol use.[27]In <strong>Australia</strong>, it is estimated that 47% <strong>of</strong> allperpetrators <strong>of</strong> assault and 43% <strong>of</strong> all victims <strong>of</strong>assault were <strong>in</strong>toxicated prior to the event.[28]It has also been reported that 34% <strong>of</strong> homicideperpetrators and 31% <strong>of</strong> homicide victims werealcohol affected at the time <strong>of</strong> the homicide. Inaddition, it has been estimated that alcohol isan important factor <strong>in</strong> 50% <strong>of</strong> cases <strong>of</strong> domesticphysical and sexual violence.[29] In a s<strong>in</strong>gleyear (1998–1999), there were 8661 peopleadmitted to <strong>Australia</strong>n hospitals with <strong>in</strong>juriesfrom alcohol-<strong>related</strong> assaults; 62,534 alcohol<strong>related</strong>assaults were reported to police <strong>in</strong> thesame year, and it is estimated that many morewent unreported. Of the hospitalisations with<strong>in</strong>juries from alcohol-<strong>related</strong> assaults, 74% weremale and two-thirds were aged 15–34 years.[30]An important factor <strong>in</strong> alcohol-<strong>related</strong> violenceis the sett<strong>in</strong>g where dr<strong>in</strong>k<strong>in</strong>g occurs. <strong>Australia</strong>nstudies have generally confirmed that alcohol<strong>related</strong>violence most commonly occurs <strong>in</strong> andaround <strong>in</strong>ner-city hotels, <strong>in</strong> the early hours <strong>of</strong>Saturday and Sunday morn<strong>in</strong>gs, and usuallyamong young adult males.[31]Furthermore, it has been shown that themajority <strong>of</strong> alcohol-<strong>related</strong> <strong>in</strong>cidents occur<strong>in</strong> a m<strong>in</strong>ority <strong>of</strong> high-risk licensed venues.[32]It is not surpris<strong>in</strong>g that much <strong>of</strong> the time andresources <strong>of</strong> polic<strong>in</strong>g <strong>in</strong> <strong>Australia</strong> is <strong>related</strong> to<strong>in</strong>cidents <strong>in</strong>volv<strong>in</strong>g alcohol. One study reportedthat alcohol is <strong>in</strong>volved <strong>in</strong> 62% <strong>of</strong> all policeattendances, 73% <strong>of</strong> assaults, 77% <strong>of</strong> street<strong>of</strong>fences, 40% <strong>of</strong> domestic violence <strong>in</strong>cidentsand 90% <strong>of</strong> late-night calls, from 10.00pm to2.00am.[31]The total social cost <strong>of</strong> the harmful consumption<strong>of</strong> alcohol is estimated to be more than$15 billion each year.[4] The majority <strong>of</strong> thesecosts are for tangible social costs such as crime($1.6 billion), health ($1.9 billion), productivity<strong>in</strong> the workplace ($3.5 billion), productivity <strong>in</strong>the home ($1.5 billion) and road accidents($2.2 billion) (see Table 4).Table 4: Estimated social costs <strong>of</strong> alcohol abuse,<strong>Australia</strong>, 2004–2005Type <strong>of</strong> cost $mReduction <strong>in</strong> workforce and absenteeism 3,579Labour <strong>in</strong> the household 1,571Medical 541Hospital 662Nurs<strong>in</strong>g homes 401Pharmaceuticals 298Ambulances 75Road accidents 2,202Police 747Crim<strong>in</strong>al courts 86Prisons 142Property 67Insurance adm<strong>in</strong>istration 14Productivity <strong>of</strong> prisoners 368Resources used <strong>in</strong> abusive consumption 1,689Loss <strong>of</strong> life 4,135Pa<strong>in</strong> and suffer<strong>in</strong>g (road accidents) 354Source: Coll<strong>in</strong>s & Lapsley 2008[4]14
3.3 <strong>Health</strong> <strong>in</strong>equalitiesGeographicThere are variations <strong>in</strong> alcohol consumptionacross <strong>Australia</strong> and different impacts onspecific high-risk population groups. Per capitaalcohol consumption varies significantlybetween urban and rural areas, and between<strong>Australia</strong>n states and territories. For <strong>in</strong>stance,while the prevalence <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g at short-termrisky/high-risk levels at least monthly is 18.7%<strong>in</strong> New South Wales and 19.4% <strong>in</strong> Victoria, itis 28.4% <strong>in</strong> the Northern Territory.[1] <strong>Alcohol</strong>consumption levels (and alcohol-attributablemortality and morbidity) are consistently foundto be lower for people liv<strong>in</strong>g with<strong>in</strong> majorcities when compared to outer regions. In2004 it was estimated that the proportion <strong>of</strong><strong>Australia</strong>ns who drank at risky/high-risk levelsfor short-term harm, resid<strong>in</strong>g <strong>in</strong> outer regional(24%) and remote/very remote (28%) locationswas between 20% and 40% greater than forresidents <strong>of</strong> major cities. The proportion <strong>of</strong>the population resid<strong>in</strong>g <strong>in</strong> outer regional andremote/very remote locations who drank atrisky/high-risk levels for long-term harm were11% and 16% respectively, compared to 9.5%<strong>in</strong> major cities. Not surpris<strong>in</strong>gly, there are alsogeographic differences <strong>in</strong> the rates <strong>of</strong> alcohol<strong>related</strong>harm <strong>in</strong> <strong>Australia</strong>. The Northern Territoryhas the highest rate <strong>of</strong> alcohol-attributabledeaths and hospitalisations <strong>in</strong> the country.Indigenous <strong>Australia</strong>nsIndigenous <strong>Australia</strong>ns are about twice as likelyto absta<strong>in</strong> from alcohol as non-Indigenous<strong>Australia</strong>ns, but those who do dr<strong>in</strong>k may beup to six times more likely to dr<strong>in</strong>k at high-risklevels than non-Indigenous people.[34] A surveyestimated that 38% <strong>of</strong> Indigenous people aged14 and over drank at risky/high-risk levels foracute harm, compared to 20% among non-Indigenous people; and that 23% drank at risky/high-risk levels for chronic harm, comparedto about 10% <strong>of</strong> non-Indigenous people.[35]However, a less recent, but better designed,Indigenous-specific survey <strong>of</strong> substancemisuse found that about 58% <strong>of</strong> all Indigenousrespondents drank at risky/high-risk levels.[36]Among Indigenous people who live <strong>in</strong> remoteparts <strong>of</strong> <strong>Australia</strong>, levels <strong>of</strong> alcohol consumptionare particularly high.In 2002–2003 the rate <strong>of</strong> hospital admissionamong Indigenous males for conditions <strong>related</strong>to high levels <strong>of</strong> alcohol use was betweentwo and seven times greater than for non-Indigenous males. Such conditions <strong>in</strong>cludeacute alcohol <strong>in</strong>toxication, alcoholic liverdisease, harmful use and alcohol dependence.In addition, between 1999 and 2003 about71% <strong>of</strong> Indigenous homicides occurred <strong>in</strong>situations where both the perpetrator andvictim were dr<strong>in</strong>k<strong>in</strong>g (as opposed to 19% <strong>of</strong>non-Indigenous homicides).[29] Other studieshave shown that the rates <strong>of</strong> death from whollyalcohol-caused conditions among residents<strong>of</strong> Western <strong>Australia</strong>, South <strong>Australia</strong> and theNorthern Territory are almost eight times greaterfor Indigenous males than for non-Indigenousmales and 16 times greater for Indigenousfemales than for other females.[37] The level<strong>of</strong> alcohol-attributable death among youngIndigenous <strong>Australia</strong>ns (15–24 years) has alsobeen shown to be almost three times greaterthan for their non-Indigenous counterparts– with the divergence between the twopopulations apparently <strong>in</strong>creas<strong>in</strong>g <strong>in</strong> recentyears.[38]15
Young <strong>Australia</strong>nsRates <strong>of</strong> risky dr<strong>in</strong>k<strong>in</strong>g <strong>in</strong> <strong>Australia</strong> peakamongst young people,[2] and alcohol<strong>related</strong>harm is substantial for both adolescentsand young adults. Dr<strong>in</strong>k<strong>in</strong>g contributes tothe three lead<strong>in</strong>g causes <strong>of</strong> death amongadolescents – un<strong>in</strong>tentional <strong>in</strong>juries, homicideand suicide – along with risk-tak<strong>in</strong>g behaviour,unsafe sex choices, sexual coercion andalcohol overdose.[18] A recent study <strong>of</strong> selfreportedharm found that dr<strong>in</strong>kers under theage <strong>of</strong> 15 years are much more likely thanolder dr<strong>in</strong>kers to experience risky or antisocialbehaviour connected with their dr<strong>in</strong>k<strong>in</strong>g, andthe rates are also somewhat elevated amongdr<strong>in</strong>kers aged 15–17 years.[39] Furthermore,<strong>in</strong>itiation <strong>of</strong> alcohol use at a young age may<strong>in</strong>crease the likelihood <strong>of</strong> negative physicaland mental health conditions, social problemsand alcohol dependence. Regular dr<strong>in</strong>k<strong>in</strong>g<strong>in</strong> adolescence is an important risk factor forthe development <strong>of</strong> dependent and riskypatterns <strong>of</strong> use <strong>in</strong> young adulthood. Childhoodand adolescence are critical times for bra<strong>in</strong>development and the bra<strong>in</strong> is more sensitive toalcohol-<strong>in</strong>duced damage dur<strong>in</strong>g these times,while be<strong>in</strong>g less sensitive to cues that couldmoderate alcohol <strong>in</strong>take.Like adolescents, young adults cont<strong>in</strong>ue to begreater risk takers than older adults, but theirdecision-mak<strong>in</strong>g skills rema<strong>in</strong> undeveloped –factors that are reflected <strong>in</strong> the high levels <strong>of</strong><strong>in</strong>juries susta<strong>in</strong>ed by this age group. <strong>Alcohol</strong>affects bra<strong>in</strong> development <strong>in</strong> young people;thus, dr<strong>in</strong>k<strong>in</strong>g, particularly ‘b<strong>in</strong>ge dr<strong>in</strong>k<strong>in</strong>g’, atany time before bra<strong>in</strong> development is complete(which is not until around 25 years <strong>of</strong> age) mayadversely affect later bra<strong>in</strong> function. In addition,young adults are also the adult age group mostlikely to take mood-alter<strong>in</strong>g drugs.[2]Trends <strong>in</strong> youth dr<strong>in</strong>k<strong>in</strong>g are unclear, withneither school survey data (ASSADS) nor theNational Drug Strategy Household Survey(NDSHS) demonstrat<strong>in</strong>g clear trends <strong>in</strong> dr<strong>in</strong>k<strong>in</strong>gamongst adolescents or young adults <strong>in</strong> thelast decade. While a recent exam<strong>in</strong>ation <strong>of</strong>Victorian data relat<strong>in</strong>g to young people agedbetween 12 and 24 found no clear trend <strong>in</strong>rates <strong>of</strong> risky dr<strong>in</strong>k<strong>in</strong>g, it revealed that rates <strong>of</strong>hospitalisation and presentation at emergencydepartments have <strong>in</strong>creased dramaticallyover recent years. The study suggests that therelationship between survey-derived estimates<strong>of</strong> alcohol consumption and rates <strong>of</strong> alcohol<strong>related</strong>harms is not as clear-cut as expected,and raises concerns about the sensitivity <strong>of</strong>population surveys <strong>in</strong> detect<strong>in</strong>g changes <strong>in</strong>harmful dr<strong>in</strong>k<strong>in</strong>g patterns.[40]Dr<strong>in</strong>k<strong>in</strong>g can also lead to poorer outcomes forpeople who have a mental health condition,whether it is a high-prevalence condition suchas depression or a low-prevalence conditionsuch as schizophrenia.There has been little analysis <strong>of</strong> the patterns<strong>of</strong> consumption and trends <strong>in</strong> alcohol-<strong>related</strong>dysfunction or harm <strong>in</strong> older people <strong>in</strong> <strong>Australia</strong>.Older people are more vulnerable to theeffects <strong>of</strong> alcohol due to changes <strong>in</strong> their bodycomposition, decreased metabolic capacity,the presence <strong>of</strong> co-morbid conditions and themedications that regulate these conditions.Older people express concern about reducedperceptions <strong>of</strong> safety associated with publicplace dr<strong>in</strong>k<strong>in</strong>g. Women <strong>in</strong> the baby boomer agegroup, now aged <strong>in</strong> their 50s to 70s, are morelikely than their parents to be alcohol consumersand it might be anticipated that this will producean <strong>in</strong>crease <strong>in</strong> alcohol-<strong>related</strong> morbidity <strong>in</strong> theirolder years, but this is yet to be documented.Certa<strong>in</strong> occupational groups are also known toregularly dr<strong>in</strong>k at risky/high-risk levels, especiallytradespeople and unskilled workers, and thosework<strong>in</strong>g <strong>in</strong> the hospitality, agricultural andm<strong>in</strong><strong>in</strong>g <strong>in</strong>dustries.16
4. B est practice<strong>in</strong> prevention4.1 Current activityConsiderable activity aim<strong>in</strong>g to preventalcohol-<strong>related</strong> harm is currently under way <strong>in</strong><strong>Australia</strong>. The extent to which the considerablepreventative desire and activity (planned orunder way) is likely to be effective, and howwell this activity reflects an evidence-basedapproach, is considered <strong>in</strong> the next section <strong>of</strong>this paper. In general, the measures that aremost <strong>of</strong>ten called for by community memberstend to be the least effective, while the mosteffective measures are the least popular and arethus probably the most difficult for governmentsto <strong>in</strong>troduce, usually requir<strong>in</strong>g strong leadershipand well-planned implementation.What is prevention <strong>in</strong> this area?The stated aim <strong>of</strong> <strong>Australia</strong>’s current NationalDrug Strategy is to ‘prevent the uptakeand m<strong>in</strong>imise the harmful effects <strong>of</strong> druguse <strong>in</strong> <strong>Australia</strong>n society’. Known as ‘harmm<strong>in</strong>imisation’, this approach has been def<strong>in</strong>edas encompass<strong>in</strong>g:nnnSupply reduction strategies designedto restrict the harmful supply <strong>of</strong> drugsDemand reduction strategies designedto prevent the uptake <strong>of</strong> harmful drug use<strong>Harm</strong> reduction strategies to reducedrug-<strong>related</strong> harm for <strong>in</strong>dividualsand communities.The approach <strong>of</strong> harm m<strong>in</strong>imisation, whilecomplex and requir<strong>in</strong>g cont<strong>in</strong>u<strong>in</strong>g supportfrom public advocates, is based on scientificevidence and underp<strong>in</strong>s the def<strong>in</strong>ition <strong>of</strong>prevention adopted for the review <strong>of</strong> alcohol<strong>related</strong><strong>in</strong>terventions <strong>in</strong> this paper. It canencompass universal as well as targeted<strong>in</strong>terventions (both selective: particular highrisksub-populations; and <strong>in</strong>dicated: those withemerg<strong>in</strong>g problems).Though not explored <strong>in</strong> detail <strong>in</strong> this paper, theconcept <strong>of</strong> the prevention paradox assists <strong>in</strong>understand<strong>in</strong>g prevention approaches <strong>in</strong> theareas <strong>of</strong> public health and public safety. Thisapproach suggests that more (net) harm maybe prevented through universal <strong>in</strong>terventions –focus<strong>in</strong>g on the majority who are less seriously<strong>in</strong>volved <strong>in</strong> harmful alcohol/drug use, ratherthan through <strong>in</strong>terventions that only target thesmaller proportion <strong>of</strong> high-risk users.What works <strong>in</strong> alcohol<strong>related</strong>prevention?The follow<strong>in</strong>g discussion is <strong>in</strong>formed by recentreviews <strong>of</strong> the available research evidence.This <strong>in</strong>cludes:nnnthe World <strong>Health</strong> Organization’s (WHO)<strong>in</strong>ternational review <strong>of</strong> alcohol-<strong>related</strong>research and public policy[13]a recent <strong>Australia</strong>n research monographon the prevention <strong>of</strong> substance use, riskand harm[7]a recent update <strong>of</strong> the latter, witha focus on prevention <strong>in</strong>terventionstarget<strong>in</strong>g adolescents.[41]Other recent reviews have also been drawn upon,to a lesser extent, <strong>in</strong>clud<strong>in</strong>g Stockwell 2004,[42]Loxley et al. 2005[7, 43] and NDRI 2007.[36]The conclusions reached <strong>in</strong> the WHO report[13]with regard to the respective strengths andweaknesses <strong>of</strong> different types <strong>of</strong> <strong>in</strong>terventions,accord<strong>in</strong>g to the available <strong>in</strong>ternational researchevidence, are summarised <strong>in</strong> Table 6. Included <strong>in</strong>this table are <strong>Australia</strong>n-authored evaluations <strong>of</strong>the equivalent <strong>in</strong>terventions provided by Loxleyet al.[7] and Toumbourou et al.[41] The scalesused to rate the <strong>in</strong>terventions by the respectiveauthors are summarised <strong>in</strong> Table 5 below.17
Table 5: Key to the rat<strong>in</strong>g scales shown <strong>in</strong> Table 6Rat<strong>in</strong>gEvidence <strong>of</strong>effectivenessBreadth <strong>of</strong>research supportTest across cultures<strong>Australia</strong>nevaluation0 Lack <strong>of</strong> effectiveness No studies undertaken Not tested Limited <strong>in</strong>vestigation★ Limited effectiveness 1 well-designed studycompletedTested <strong>in</strong> 1 countryEvidence forimplementation★ ★ Moderate effectiveness 2–4 studies completed Tested <strong>in</strong> 2–4 countries Evidence for outcomeeffectiveness★ ★ ★High degree <strong>of</strong>effectiveness5+ studies completed Tested <strong>in</strong> 5+ countries Evidence for effectivedissem<strong>in</strong>ation? No evidence available N/A●✖Warrants furtherresearchEvidence iscontra-<strong>in</strong>dicativeThis rat<strong>in</strong>g scale applies to the WHO’s<strong>in</strong>ternational review [13] and <strong>Australia</strong>nreviews.[14].Of the 39 <strong>in</strong>terventions listed <strong>in</strong> Table 6, at leasthalf <strong>of</strong> these are universal (targeted at the wholepopulation) and approximately half are targetedat high-risk groups. The <strong>in</strong>ternational reviewby Babor et al. concludes that <strong>in</strong>terventionstarget<strong>in</strong>g the whole population generally havehigher effectiveness rat<strong>in</strong>gs and are less costlyto implement and ma<strong>in</strong>ta<strong>in</strong>, on average, thanthose target<strong>in</strong>g high-risk groups.[13] In general,the types <strong>of</strong> <strong>in</strong>terventions that are consideredmost effective accord<strong>in</strong>g to the rat<strong>in</strong>gs are,<strong>in</strong> order:1. Regulat<strong>in</strong>g physical availability.2. Taxation and pric<strong>in</strong>g.3. Dr<strong>in</strong>k-driv<strong>in</strong>g countermeasures.4. Treatment and early <strong>in</strong>tervention.The types <strong>of</strong> <strong>in</strong>terventions for which there issomewhat less evidence <strong>of</strong> effectivenessare, <strong>in</strong> order:5. Alter<strong>in</strong>g the dr<strong>in</strong>k<strong>in</strong>g context6. Regulat<strong>in</strong>g promotion7. Education and persuasionThere are differences <strong>in</strong> the rat<strong>in</strong>gs <strong>of</strong> some<strong>in</strong>terventions between the <strong>in</strong>ternationalreview[13] and the <strong>Australia</strong>n review.[7](for example, the treatment <strong>of</strong> alcoholproblems and mass media campaigns).Also, importantly, it should be recognisedthat although the effectiveness <strong>of</strong> some<strong>in</strong>terventions do not rate highly, <strong>in</strong> somecases this may be due to the limitedresearch evidence that is available to<strong>in</strong>form the rat<strong>in</strong>g (for example, advertis<strong>in</strong>gcontent controls).18
Table 6: Rat<strong>in</strong>gs <strong>of</strong> policy-relevant strategies and <strong>in</strong>terventionsStrategy or <strong>in</strong>tervention EffectivenessBreadth <strong>of</strong>researchCrossculturaltest<strong>in</strong>gCost toimplementRegulat<strong>in</strong>g physical availability Total ban on sales ★ ★ ★ ★ ★ ★ ★ ★ High ★ ★<strong>Australia</strong>nevaluationM<strong>in</strong>imum legal purchase age ★ ★ ★ ★ ★ ★ ★ ★ LowHours and days <strong>of</strong> sale restrictions ★ ★ ★ ★ ★ ★ Low ★ ★Restrictions on density <strong>of</strong> outlets ★ ★ ★ ★ ★ ★ ★ Low ●Staggered clos<strong>in</strong>g times for bars and clubs ✖Server liability ★ ★ ★ ★ ★ Low ★Different availability by alcohol strength ★ ★ ★ ★ ★ LowTaxation and pric<strong>in</strong>g <strong>Alcohol</strong> taxes ★ ★ ★ ★ ★ ★ ★ ★ ★ Low ★ ★Hypothecated tax to pay for treatment / prevention ★ ★ ★Sett<strong>in</strong>g floor prices / bann<strong>in</strong>g discount<strong>in</strong>g ★ ★Dr<strong>in</strong>k-driv<strong>in</strong>g countermeasures Sobriety checkpo<strong>in</strong>ts ★ ★ ★ ★ ★ ★ ★ ★ ModerateRandom breath test<strong>in</strong>g ★ ★ ★ ★ ★ ★ Moderate ★ ★ ★Lowered BAC limits ★ ★ ★ ★ ★ ★ ★ ★ LowAdm<strong>in</strong>istrative licence suspension ★ ★ ★ ★ ★ ★ ModerateLow BAC for young drivers ★ ★ ★ ★ ★ ★ Low ★Graduated licens<strong>in</strong>g for novice drivers ★ ★ ★ ★ ★ ★ LowDesignated drivers and ride services 0 ★ ★ Moderate ★Ignition <strong>in</strong>terlocks ★Treatment and early <strong>in</strong>tervention Brief <strong>in</strong>tervention <strong>in</strong> primary health sett<strong>in</strong>gs ★ ★ ★ ★ ★ ★ ★ ★ Moderate ★ ★ ★<strong>Alcohol</strong> problems treatment ★ ★ ★ ★ ★ ★ ★ High ★ ★ ★Thiam<strong>in</strong>e supplementation ★ ★Workplace <strong>in</strong>terventions ●Mutual help/self-help attendance ★ ★ ★ ★ LowMandatory treatment <strong>of</strong> repeat dr<strong>in</strong>k drivers ★ ★ ★ ★ ModerateAlter<strong>in</strong>g the dr<strong>in</strong>k<strong>in</strong>g context Bans on serv<strong>in</strong>g <strong>in</strong>toxicated persons ★ ★ ★ ★ ★ ★ ModerateTra<strong>in</strong><strong>in</strong>g staff to prevent <strong>in</strong>toxication / aggression ★ ★ ★ Moderate ★ ★ (✖ if not enforced)Voluntary codes <strong>of</strong> bar practice 0 ★ ★ Low ★ ★ (✖ if not enforced)Enforcement <strong>of</strong> on-premises regulations and laws ★ ★ ★ ★ ★ HighPromot<strong>in</strong>g alcohol-free events 0 ★ ★ ★ HighCommunity mobilisation ★ ★ ★ ★ ★ High ★ ★Plastic or tempered-glass serv<strong>in</strong>g conta<strong>in</strong>ers ★Food service ★Regulat<strong>in</strong>g promotion Advertis<strong>in</strong>g bans ? ● ● LowAdvertis<strong>in</strong>g content controls ? ● ● Low ●Education and persuasion <strong>Alcohol</strong> education <strong>in</strong> schools 0 ★ ★ ★ ★ ★ High ★College student education 0 ★ ★ HighParent education ? ● ● Moderate ●Public service messages / Mass media campaigns ● ● ● Moderate ★Warn<strong>in</strong>g labels / National dr<strong>in</strong>k<strong>in</strong>g guidel<strong>in</strong>es 0 ★ ★ Low ★Source: Adapted from Babor et al. (2003),[13] Loxley et al. (2004),[7] Toumbourou et al. (2007)[41]19
4.2 Regulat<strong>in</strong>g the physicalavailability <strong>of</strong> alcoholRegulat<strong>in</strong>g physical availability refers to theaccessibility or convenience <strong>of</strong> the alcoholproducts, and relates to policies that aim toprevent alcohol-<strong>related</strong> harm through controlson the condition <strong>of</strong> sale to the dr<strong>in</strong>ker as aretail customer.[13] In <strong>Australia</strong>, there has beena recent review <strong>of</strong> the evidence for restrict<strong>in</strong>gthe sale and supply <strong>of</strong> alcohol by the NationalDrug Research Institute.[36] While regulation<strong>of</strong> the ‘economic’ availability <strong>of</strong> alcohol (i.e.the price <strong>of</strong> alcohol) is, currently, exclusively afederal responsibility <strong>in</strong> <strong>Australia</strong>, via measuressuch as taxation, the physical availability <strong>of</strong>alcohol is generally regulated by state andterritory governments, and to a limited extentby local governments.Restrict<strong>in</strong>g the hours and days <strong>of</strong> sale <strong>of</strong> alcoholis a standard component <strong>of</strong> alcohol policyand regulation, and there is a substantial body<strong>of</strong> <strong>in</strong>ternational and <strong>Australia</strong>n work that hasexam<strong>in</strong>ed the impact <strong>of</strong> changes to trad<strong>in</strong>ghours for licensed premises on levels <strong>of</strong> alcoholconsumption and rates <strong>of</strong> <strong>related</strong> harms. Most<strong>Australia</strong>n studies have shown that <strong>in</strong>creasedtrad<strong>in</strong>g hours have been accompaniedby significantly <strong>in</strong>creased levels <strong>of</strong> alcoholconsumption and/or harms.[36] A recent<strong>Australia</strong>n study by Chikritzhs and Stockwell[44]found that small extensions <strong>of</strong> trad<strong>in</strong>g hoursfor licensed hotels <strong>in</strong> Perth, Western <strong>Australia</strong>,significantly <strong>in</strong>creased the numbers <strong>of</strong> dr<strong>in</strong>kdriverroad crashes. More specifically, this studydemonstrated that the relationship betweentrad<strong>in</strong>g hours and <strong>in</strong>creased dr<strong>in</strong>k-driver roadcrashes was mediated by the quantity <strong>of</strong>alcohol purchases. The National Drug ResearchInstitute (NDRI) reports that several studies have<strong>in</strong>dicated that young males and regular heavydr<strong>in</strong>kers are especially likely to take advantage<strong>of</strong> longer trad<strong>in</strong>g hours.[36]Restrictions on density <strong>of</strong> outlets can beachieved by requir<strong>in</strong>g m<strong>in</strong>imum distancesbetween outlets or limit<strong>in</strong>g the number <strong>of</strong>outlets <strong>in</strong> a particular location.Liquor licens<strong>in</strong>g systems or plann<strong>in</strong>g controlscan potentially be used to limit the number<strong>of</strong> places where alcohol can be sold. Inrecent years <strong>in</strong> <strong>Australia</strong> there has been asignificant liberalisation <strong>of</strong> licens<strong>in</strong>g laws anda correspond<strong>in</strong>g growth <strong>in</strong> outlets, both onand<strong>of</strong>f-premises. Recent research from threestates,[45-49] has demonstrated consistent l<strong>in</strong>ksbetween the availability <strong>of</strong> alcohol <strong>in</strong> a regionand the alcohol-<strong>related</strong> problems experiencedthere. In particular, these studies have l<strong>in</strong>kedrates <strong>of</strong> violence to density <strong>of</strong> alcohol outlets. Alongitud<strong>in</strong>al study <strong>in</strong> Melbourne has highlightedthat changes <strong>in</strong> the number <strong>of</strong> outlets <strong>in</strong> anarea are directly <strong>related</strong> to changes <strong>in</strong> therates <strong>of</strong> night-time assaults occurr<strong>in</strong>g there.The l<strong>in</strong>ks between outlet density and otheroutcomes are less clear cut, although some<strong>in</strong>ternational evidence suggests higher outletdensity is <strong>related</strong> to higher rates <strong>of</strong>: risky alcoholconsumption,[50] motor vehicle accidents,[51]risky sexual behaviour,[52] pedestrian <strong>in</strong>jury,[53]child maltreatment[54] and neighbourhoodamenity problems.[55] The results <strong>of</strong> thisresearch are clear: liberalis<strong>in</strong>g alcoholavailability is likely to <strong>in</strong>crease alcohol-<strong>related</strong>problems. The results certa<strong>in</strong>ly call <strong>in</strong>to questionthe general assumption beh<strong>in</strong>d actions <strong>in</strong>recent decades that have been made <strong>in</strong>accordance with National Competition Policysuch as the state-led liberalisation <strong>of</strong> liquorlicens<strong>in</strong>g regimes – that the number <strong>of</strong> a type<strong>of</strong> outlet should be determ<strong>in</strong>ed by marketdemand for the product, without consideration<strong>of</strong> community amenity or impacts.Apart from issues <strong>of</strong> outlet density, there is thequestion <strong>of</strong> whether particular types <strong>of</strong> outletsor their design and location are particularlylikely to cause problems. There is goodevidence that certa<strong>in</strong> premises contributedisproportionately to problems,[32] highlight<strong>in</strong>gthe need to further exam<strong>in</strong>e the types <strong>of</strong> outletsthat are <strong>related</strong> to assaults. Further data, suchas alcohol sales, open<strong>in</strong>g hours, capacity andvenue style, could provide substantial <strong>in</strong>sights<strong>in</strong>to how different outlets contribute to theeffect <strong>of</strong> outlet density on assault.20
Growth <strong>in</strong> alcohol outletsWhile not completely deregulated, liquorlicens<strong>in</strong>g laws and regulations <strong>in</strong> mostjurisdictions have been significantly relaxedover the past decade, generally co<strong>in</strong>cid<strong>in</strong>gwith the required reviews under the NationalCompetition Policy. One <strong>of</strong> the effects <strong>of</strong> thishas been a proliferation <strong>in</strong> the number <strong>of</strong>new licensed premises <strong>in</strong> some jurisdictions(see Fig. 8).Along with an <strong>in</strong>crease <strong>in</strong> the total number<strong>of</strong> licensed premises, there has beenan <strong>in</strong>crease <strong>in</strong> the numbers <strong>of</strong> premiseswith extended trad<strong>in</strong>g hours, the numbers<strong>of</strong> licences to sell packaged liquor(i.e. take away) and over time, an <strong>in</strong>creasedconcentration <strong>of</strong> licences held by just afew bus<strong>in</strong>esses.Figure 8: Number <strong>of</strong> liquor licences by year,Victoria, 1986 to 2006Source: Consumer Affairs Victoria, unpublished dataRestrict<strong>in</strong>g availability by alcohol strength isknown to be an effective <strong>in</strong>tervention, both<strong>in</strong>ternationally and <strong>in</strong> <strong>Australia</strong>. In <strong>Australia</strong>,it has been estimated that full-strength beermakes the largest s<strong>in</strong>gle contribution to all riskyand high-risk alcohol consumption (39%).[21]The National Drug Research Institute (NDRI)reports that studies that have exam<strong>in</strong>ed therelationship between alcoholic beverage typeand levels <strong>of</strong> alcohol-<strong>related</strong> harm have found<strong>in</strong>creas<strong>in</strong>g evidence that beer consumption ismore commonly associated with dr<strong>in</strong>k-driv<strong>in</strong>g.[36] The NDRI also observes that while moststudies identify w<strong>in</strong>e as a comparatively low-riskbeverage, a study by Stockwell et al. (1998)[56] found that certa<strong>in</strong> types <strong>of</strong> w<strong>in</strong>e that <strong>of</strong>ferhigh alcohol content at a relatively low pricewere strongly associated with hospitalisationsfor alcohol-<strong>related</strong> road <strong>in</strong>juries, falls, assaultsand suicides. Some small regional or remotecommunities <strong>in</strong> <strong>Australia</strong>, with relatively largeIndigenous populations, have <strong>in</strong>troduced salesbans on cask w<strong>in</strong>e and cask fortified w<strong>in</strong>e.Accord<strong>in</strong>g to the NDRI,[36] evaluations <strong>of</strong> some<strong>of</strong> these bans show that such restrictions canresult <strong>in</strong> reduced alcohol-<strong>related</strong> harm <strong>in</strong> thecommunities where the bans exist.The issue <strong>of</strong> the server liability for <strong>in</strong>juries to<strong>in</strong>toxicated people or third parties affected bythe actions <strong>of</strong> a person affected by alcohol isa complex and controversial area <strong>of</strong> the law.[57] In the US, ‘Dram Shop’ laws and courtdecisions under common law <strong>in</strong> many statesallow people <strong>in</strong>jured through the actions <strong>of</strong> an<strong>in</strong>toxicated person to recover damages froma licensee or licensed premises owner. Suchlicensees are, <strong>in</strong> most Dram Shop legislation,also vicariously liable for their employees’actions <strong>in</strong> serv<strong>in</strong>g an (<strong>in</strong>toxicated) patron.[57]Loxley et al. report[7] that studies show DramShop laws have a modest deterrent effect, andthat the underly<strong>in</strong>g rationale for discourag<strong>in</strong>gservice <strong>of</strong> <strong>in</strong>toxicated persons is sound andthere is no likelihood <strong>of</strong> adverse consequences.A recent <strong>Australia</strong>n review <strong>of</strong> the key aspects<strong>of</strong> law and the implications <strong>of</strong> recent courtdecisions has reported that there is now a lessonerous duty <strong>of</strong> care imposed on licensees andtheir staff with regard to the consequences <strong>of</strong>serv<strong>in</strong>g alcohol.[58] (See also the discussion <strong>of</strong>responsible service <strong>of</strong> alcohol (RSA) <strong>in</strong>terventions<strong>in</strong> Section 4.6 <strong>of</strong> this paper).M<strong>in</strong>imum legal purchase age refers to the ageat which alcohol can actually be purchasedby a person. This is dist<strong>in</strong>ct from the age atwhich alcohol can be consumed, sometimesreferred to as the legal dr<strong>in</strong>k<strong>in</strong>g age.21
The dist<strong>in</strong>ction is important because while allstate and territory laws <strong>in</strong> <strong>Australia</strong>n prohibita m<strong>in</strong>or from purchas<strong>in</strong>g alcohol, they do notnecessarily prohibit consumption <strong>in</strong> certa<strong>in</strong>circumstances. Babor et al. emphasise thatconsistent enforcement <strong>of</strong> laws regard<strong>in</strong>gpurchase age is critical if reduced alcoholconsumption and <strong>related</strong> harm among youngpeople is to be achieved.[13] Although them<strong>in</strong>imum legal purchase age for alcohol <strong>in</strong> all<strong>Australia</strong>n jurisdictions is 18 years, the averageage at which <strong>Australia</strong>ns have their first fullserve <strong>of</strong> alcohol is 17 years, and as detailedearlier <strong>in</strong> this paper, there is a high prevalence<strong>of</strong> underage dr<strong>in</strong>k<strong>in</strong>g that has not changedsignificantly <strong>in</strong> the past 20 years. In the US,where the m<strong>in</strong>imum legal purchase age forsome time ranged between 18 and 21 years,several studies have found that <strong>in</strong>creas<strong>in</strong>g theage limit is an effective means <strong>of</strong> reduc<strong>in</strong>groad crash death and <strong>in</strong>jury among teenagersand young adults. The NDRI reports[36] thatsome studies have also found that the higherlegal m<strong>in</strong>imum dr<strong>in</strong>k<strong>in</strong>g age is associated withreductions <strong>in</strong> alcohol consumption amongyoung people. There is, therefore, someevidence that rais<strong>in</strong>g the purchase age to21 can reduce teenage dr<strong>in</strong>k<strong>in</strong>g, as well asharms. Kypri’s account[59] <strong>of</strong> recent attemptsto <strong>in</strong>crease the m<strong>in</strong>imum purchase age <strong>in</strong>New Zealand to 20 demonstrated that populardebate conv<strong>in</strong>ced a majority <strong>of</strong> the public thatrais<strong>in</strong>g the age would be an appropriate wayto reduce young people’s harm from dr<strong>in</strong>k<strong>in</strong>g.Toumbourou et al. here <strong>in</strong> <strong>Australia</strong> haverecommended that a first step <strong>in</strong> this directionwould be better monitor<strong>in</strong>g <strong>of</strong> alcohol-<strong>related</strong>developmental harms us<strong>in</strong>g longitud<strong>in</strong>al andother developmental research.[41]It must be acknowledged that consumption<strong>of</strong> alcohol by children and adolescents <strong>in</strong> thehome and <strong>in</strong> certa<strong>in</strong> social sett<strong>in</strong>gs is <strong>of</strong>tensanctioned by parents, <strong>of</strong>ten <strong>in</strong> the belief thatit is relatively harmless or might be helpful <strong>in</strong>educat<strong>in</strong>g young people about alcohol.[60]The majority <strong>of</strong> young <strong>Australia</strong>ns who reportdr<strong>in</strong>k<strong>in</strong>g at home also report parents as be<strong>in</strong>gthe primary suppliers <strong>of</strong> their alcohol.[61]In New South Wales, it is now an <strong>of</strong>fence tosupply alcohol to m<strong>in</strong>ors <strong>in</strong> a private homewithout the direct approval <strong>of</strong> a parent orguardian. This has <strong>of</strong>ten been referred to as theNSW secondary supply law. While the impact<strong>of</strong> this law on youth dr<strong>in</strong>k<strong>in</strong>g is not yet known,legislation <strong>of</strong> this k<strong>in</strong>d has been welcomedby advocates aga<strong>in</strong>st alcohol-<strong>related</strong> harmand there is currently considerable lobby<strong>in</strong>g<strong>of</strong> government to support the <strong>in</strong>troduction <strong>of</strong>similar laws <strong>in</strong> other <strong>Australia</strong>n jurisdictions.[60]Another example <strong>of</strong> restrictions on the physicalavailability <strong>of</strong> alcohol, which is known to beeffective <strong>in</strong> reduc<strong>in</strong>g alcohol-<strong>related</strong> harm<strong>in</strong> some <strong>Australia</strong>n Indigenous communities,is referred to as dry community declarations.[36] Some remote Indigenous communities <strong>in</strong>Western <strong>Australia</strong>, the Northern Territory andSouth <strong>Australia</strong> have declared themselves ‘dry’,us<strong>in</strong>g provisions <strong>of</strong> state/territory legislation.The key element <strong>of</strong> such dry area declarationsis a comb<strong>in</strong>ation <strong>of</strong> Indigenous communitycontrol and statutory authority, along withpolice enforcement for ensur<strong>in</strong>g that drycommunity declarations reach their potential.Evidence suggests that although there areshortcom<strong>in</strong>gs (for example, sly grogg<strong>in</strong>g) andassociated costs to this approach, overallthere are reductions <strong>in</strong> consumption andalcohol-<strong>related</strong> harm. It should be notedthat dry community declarations are dist<strong>in</strong>ctfrom local dry area alcohol bans, as the latterrelate to restrictions on dr<strong>in</strong>k<strong>in</strong>g <strong>in</strong> designatedpublic places and are usually imposedwhere there are high rates <strong>of</strong> alcohol-<strong>related</strong>public disorder.[36] While local dry area banshave been found to decrease public orderproblems <strong>in</strong> designated areas, overall it is notyet fully known if they reduce public order<strong>of</strong>fences, alcohol-<strong>related</strong> hospitalisations orpolice detentions <strong>of</strong> <strong>in</strong>toxicated persons. Oftendry area restrictions simply displace dr<strong>in</strong>kersto other areas where there are no, or fewer,restrictions, and dry area declarations are <strong>of</strong>tenseen as <strong>in</strong>herently discrim<strong>in</strong>atory because <strong>of</strong>the negative impacts on Indigenous peoplealready at risk <strong>of</strong> alcohol problems.[36]22
Currently receiv<strong>in</strong>g considerable attention<strong>in</strong> some <strong>Australia</strong>n jurisdictions are measures<strong>related</strong> to restrict<strong>in</strong>g the hours <strong>of</strong> sale <strong>of</strong> alcohol,known as lockouts. These do not restrict trad<strong>in</strong>ghours per se, however, because outlets arepermitted to cont<strong>in</strong>ue trad<strong>in</strong>g until their usualclos<strong>in</strong>g times. However, after a certa<strong>in</strong> time,such as 2:00am or 3:00am, new patrons andthose wish<strong>in</strong>g to re-enter the premises are notpermitted to do so. Lockouts aim to reduce themovement <strong>of</strong> people between clubs after acerta<strong>in</strong> time, s<strong>in</strong>ce it is this movement <strong>of</strong> peoplebetween venues that police have reportedas be<strong>in</strong>g a major cause <strong>of</strong> alcohol-<strong>related</strong><strong>in</strong>cidents late at night. There are examples<strong>of</strong> lockout programs <strong>in</strong> operation <strong>in</strong> locationsthroughout <strong>Australia</strong>, such as <strong>in</strong> Ballarat andBendigo <strong>in</strong> Victoria, and across Queensland,where a 3.00am lockout now applies to alllate-night licensed premises. The Victoriangovernment has also trialled a 2.00am lockoutthroughout four <strong>in</strong>ner-city municipalities <strong>of</strong>Melbourne. The NDRI reports[36] that, asyet, there is limited formal evidence <strong>of</strong> theeffectiveness <strong>of</strong> lockout programs, <strong>in</strong> partbecause they <strong>of</strong>ten occur as one elementwith<strong>in</strong> a range <strong>of</strong> programs aimed at reduc<strong>in</strong>glate-night alcohol-<strong>related</strong> problems (forexample, CCTV cameras, street light<strong>in</strong>g, publictransport, police presence).While they are not usually focused solely onissues that relate to the physical availability<strong>of</strong> alcohol, community-based preventionprograms have become <strong>in</strong>creas<strong>in</strong>glypopular <strong>in</strong> recent years because <strong>of</strong> emerg<strong>in</strong>gunderstand<strong>in</strong>gs <strong>of</strong> how environmental andsocial conditions contribute to alcoholproblems.[7] A detailed discussion on therange and scope effects <strong>of</strong> community basedprograms is not provided here, but can beobta<strong>in</strong>ed elsewhere (see Loxley et al. 2007:[7]pp166–167).4.3 Taxation and pric<strong>in</strong>gThe price <strong>of</strong> alcohol clearly impacts onconsumption patterns. There are more than50 studies from around the world show<strong>in</strong>gthat when alcohol <strong>in</strong>creases <strong>in</strong> price,consumption is reduced.[12, 39-42] The World<strong>Health</strong> Organization (WHO) is one <strong>of</strong> many<strong>in</strong>ternational and national health organisationsthat strongly endorse the use <strong>of</strong> <strong>in</strong>creasedalcohol taxation (higher prices for alcoholproducts) as an effective preventative strategyto reduce alcohol-<strong>related</strong> harm.[62] At thesame time, it is important to recognise thatthere is a complex relationship between priceand consumption.[63, 64] Patterns <strong>of</strong> alcoholconsumption can vary considerably accord<strong>in</strong>gto <strong>in</strong>dividual factors such as the age, sex and<strong>in</strong>come levels <strong>of</strong> the dr<strong>in</strong>ker. Other factors suchas availability, the cultural sett<strong>in</strong>g, the market<strong>in</strong>gand image <strong>of</strong> the product are also important.Studies consistently show that lower socioeconomicgroups and people with limiteddisposable <strong>in</strong>come (young people, Indigenousgroups and heavy dr<strong>in</strong>kers) are more directlyimpacted by the price <strong>of</strong> alcohol products.Higher <strong>in</strong>come dr<strong>in</strong>kers tend to dr<strong>in</strong>k moreexpensive alcohol, and while price may leadthem to reduce their consumption marg<strong>in</strong>ally,they are also able to alter dr<strong>in</strong>k<strong>in</strong>g preferencesto cheaper alternatives.[65, 66] The nature<strong>of</strong> the alcohol product is also a key variable.An <strong>Australia</strong>n study identified considerablevariations <strong>in</strong> price elasticity (the amount thatprice needs to change before it impacts onconsumption) for different alcohol products.It concluded that spirits are twice as pricesensitive as w<strong>in</strong>e and beer.[67]Given the complexity <strong>of</strong> the relationshipbetween alcohol price and consumption,<strong>in</strong>creas<strong>in</strong>g alcohol taxation does not necessarilylead to a l<strong>in</strong>ear reduction <strong>in</strong> the levels <strong>of</strong>alcohol-<strong>related</strong> harm. It is important that therelationship between the price <strong>of</strong> <strong>in</strong>dividualalcohol products and consumption amongstparticular groups <strong>of</strong> dr<strong>in</strong>kers is carefullymodelled aga<strong>in</strong>st known price elasticity andexist<strong>in</strong>g consumption patterns.23
While <strong>in</strong>creas<strong>in</strong>g the price through taxationis likely to lead to a reduction <strong>in</strong> per capitaconsumption, <strong>in</strong>creas<strong>in</strong>g the price <strong>of</strong> <strong>in</strong>dividualproducts may not necessarily achieve this goal.In some cases, product-based changes cancreate opportunities for new products anddr<strong>in</strong>k<strong>in</strong>g patterns that <strong>in</strong>crease levels <strong>of</strong> harm.[68] In this context, it is important to recognisethat the production costs <strong>of</strong> alcohol productsvary considerably between product types(eg spirits are relatively <strong>in</strong>expensive tomanufacture compared to beer and w<strong>in</strong>eproducts) which <strong>in</strong> turn has a bear<strong>in</strong>g on thecost price to consumers.<strong>Australia</strong>’s alcohol tax system can best beunderstood as a constantly chang<strong>in</strong>g reflection<strong>of</strong> the history <strong>of</strong> alcohol consumption <strong>in</strong> <strong>Australia</strong>,and the status <strong>of</strong> various alcohol products.It also reflects chang<strong>in</strong>g powers <strong>of</strong> taxationbetween state and territory governments andthe <strong>Australia</strong>n Government. As a consequence,different products – w<strong>in</strong>e, spirits, beer, ciders,fortified w<strong>in</strong>es – are all taxed differently. Theexcise duties arrangements can generally bedescribed as a volumetric tax system, becausethe amount <strong>of</strong> excise duty depends on thevolume <strong>of</strong> alcohol conta<strong>in</strong>ed <strong>in</strong> the particularproduct. W<strong>in</strong>e equalisation tax can be describedas an ad valorem tax system, because the rate<strong>of</strong> tax depends on the value <strong>of</strong> the retail sell<strong>in</strong>gprice <strong>of</strong> the particular product. Customs dutiesare a comb<strong>in</strong>ation <strong>of</strong> both volumetric and advalorem systems. GST is set at a fixed rate <strong>of</strong> 10%<strong>of</strong> the product price, on top <strong>of</strong> all other taxes(see Table 7).With<strong>in</strong> some categories there are variousconcessions and exceptions. Smaller w<strong>in</strong>eries,for <strong>in</strong>stance, are largely exempt from their valueadded tax (the W<strong>in</strong>e Equalisation Tax) for allcellar door sales.Recent estimates show that the <strong>Australia</strong>nGovernment will collect over $6 billion as aresult <strong>of</strong> the production and consumption <strong>of</strong>alcohol dur<strong>in</strong>g the 2008/09 f<strong>in</strong>ancial year.[68, 4]However, a substantial disparity exists betweenthe amount <strong>of</strong> tax revenue received by the<strong>Australia</strong>n Government from risky dr<strong>in</strong>k<strong>in</strong>gcompared with the overall amount spent <strong>in</strong>attempt<strong>in</strong>g to prevent harmful consumption<strong>of</strong> alcohol. For example, it has been estimatedthat <strong>Australia</strong>n adolescents (aged 12–17 years)spent approximately $217 million on alcoholicbeverages <strong>in</strong> 2002, nett<strong>in</strong>g the <strong>Australia</strong>nGovernment approximately $112 million <strong>in</strong> taxrevenue.[69] This means that for every dollarspent on alcohol <strong>in</strong>terventions aimed atadolescents, the government receives around$7 <strong>in</strong> alcohol tax revenue.[69]The current taxation rates translate <strong>in</strong>to a widevariety <strong>of</strong> taxation per standard dr<strong>in</strong>k <strong>of</strong> alcohol(see Fig. 13). For those who argue that alcoholshould be taxed accord<strong>in</strong>g to the amount <strong>of</strong>alcohol <strong>in</strong> each product and conta<strong>in</strong>er, thecurrent system represents a massive distortion<strong>of</strong> this pr<strong>in</strong>ciple.Table 7: Summary <strong>of</strong> the types <strong>of</strong> alcohol taxesapplied by category <strong>of</strong> alcohol productBeer Spirits & RTDs W<strong>in</strong>e CiderGST Yes Yes Yes YesExcise duty Yes Yes No NoWET No No Yes YesCustoms duty (ad valorem) No Yes (imported) Yes (imported) NoCustoms duty (volumetric) Yes (imported) Yes (imported) No No24
$1.00$0.90$0.81$0.87$0.87Excise or WET payable per standard dr<strong>in</strong>k:$0.80$0.70$0.60$0.50$0.40$0.30$0.20$0.10$0.04$0.05$0.16$0.17$0.19$0.26$0.28$0.32$0.39$0.52$-Light beeron tapCask W<strong>in</strong>e Port, Sherry Mid strengthbeer on tapPackagedlight beerBottled W<strong>in</strong>e1Full strengthbeer on tapPackagedmid strengthbeerPackagedfull strengthbeerBottled W<strong>in</strong>e2BrandyPre-mixedspirits /RTDsWhistky,Rum,Vodka,LiqueursTypical ABV:2 12.5 20 3 2 14 5 3 5 14 37 3.0 - 9.0 22 - 43Figure 13: Tax payable per standard dr<strong>in</strong>k*<strong>of</strong> alcohol, various products, <strong>Australia</strong>, as at1 August 2008*Note: *Includes a 1.15% ABV excise-free concession for beer. WET payableper standard dr<strong>in</strong>k <strong>of</strong> w<strong>in</strong>e is based on a four-litre cask <strong>of</strong> w<strong>in</strong>e sell<strong>in</strong>gfor $13 (<strong>in</strong>cl. GST) [‘Cask W<strong>in</strong>e’], a 750ml bottle <strong>of</strong> w<strong>in</strong>e sell<strong>in</strong>g for $15(<strong>in</strong>cl. GST) [‘Bottled W<strong>in</strong>e 1’], a 750ml bottle <strong>of</strong> w<strong>in</strong>e sell<strong>in</strong>g for $30(<strong>in</strong>cl. GST) [‘Bottled W<strong>in</strong>e 2’] and a 750ml bottle <strong>of</strong> port sell<strong>in</strong>g for $13(<strong>in</strong>cl. GST) [‘Port, Sherry’]. A standard dr<strong>in</strong>k is equal to 0.001267 litres or10 grams <strong>of</strong> pure alcohol.As noted above, <strong>Australia</strong> has been througha cont<strong>in</strong>uous process <strong>of</strong> change <strong>in</strong> relationto the taxation and pric<strong>in</strong>g <strong>of</strong> various alcoholproducts. There are three changes that areparticularly <strong>in</strong>terest<strong>in</strong>g to note. In the late 1980s,states and territories adopted various forms<strong>of</strong> licens<strong>in</strong>g for all alcohol sales. As part <strong>of</strong> thissystem, most jurisdictions <strong>of</strong>fered low-alcoholbeer (less than 3.5% alcohol by volume) fora significant concession <strong>in</strong> fees. The licensefee concession translated <strong>in</strong>to cheaper lowalcoholbeer and, <strong>in</strong> comb<strong>in</strong>ation with <strong>in</strong>tensemarket competition <strong>in</strong> the beer market andthe <strong>in</strong>troduction <strong>of</strong> harm-reduction measuressuch as random breath test<strong>in</strong>g, createdan ideal environment for low-alcohol beer.Producers recognised the benefit <strong>of</strong> <strong>in</strong>vest<strong>in</strong>gconsiderable developmental and market<strong>in</strong>g<strong>in</strong>vestment <strong>in</strong>to low-alcohol beer.As a consequence, low-alcohol beer <strong>in</strong>creasedits sales very significantly and capturedapproximately 20% <strong>of</strong> the total <strong>Australia</strong>nbeer market.[70]The Northern Territory’s ‘Liv<strong>in</strong>g with <strong>Alcohol</strong>’program provides another example <strong>of</strong> howchanges <strong>in</strong> price through government taxation<strong>in</strong>creases contributed to a reduction <strong>in</strong> percapita consumption. In 1992, the NorthernTerritory government used a hypothecationapproach by plac<strong>in</strong>g a levy <strong>of</strong> 5 cents perstandard dr<strong>in</strong>k on the sale <strong>of</strong> alcohol productswith more than 3% alcohol by volumeand used the revenue to fund a range <strong>of</strong>alcohol-prevention measures <strong>in</strong> the territory.[71] Evaluations <strong>of</strong> the ‘Liv<strong>in</strong>g with <strong>Alcohol</strong>’program found that the <strong>in</strong>crease <strong>in</strong> price hadcontributed to a major reduction <strong>in</strong> the level<strong>of</strong> alcohol-<strong>related</strong> harm with<strong>in</strong> the NorthernTerritory.[72, 73]Over the last 15 years, there have been a series<strong>of</strong> changes <strong>in</strong> the level <strong>of</strong> excise and taxationapplied to various forms <strong>of</strong> the ready to dr<strong>in</strong>k(RTD) product segment <strong>of</strong> the <strong>Australia</strong>nalcohol market.25
These changes have resulted <strong>in</strong> major shifts <strong>in</strong>dr<strong>in</strong>k<strong>in</strong>g patterns across <strong>Australia</strong>, particularly <strong>in</strong>relation to brown spirit pre-mixed dr<strong>in</strong>ks (mostlyaround 5% alcohol by volume <strong>in</strong> 375ml cans)and white spirit pre-mixed bottled dr<strong>in</strong>ks (mostlyaround 5% alcohol by volume <strong>in</strong> 375ml bottles).With each price change, sales <strong>of</strong> these RTDshave <strong>in</strong>creased or decreased quite significantly.While there is considerable evidence that these<strong>in</strong>creases and decreases <strong>in</strong> sales representshifts <strong>in</strong> product preferences (market share)rather than shifts <strong>in</strong> per capita dr<strong>in</strong>k<strong>in</strong>g, thepatterns <strong>of</strong> consumption have clearly beendirectly <strong>in</strong>fluenced by taxation and pric<strong>in</strong>g.There is substantive evidence that the higherthe price, the lower the consumption <strong>of</strong> theseproducts, and the lower the price, the higherthe consumption <strong>of</strong> these products. Perhapsjust as importantly, the shifts <strong>in</strong> consumptionpatterns are more marked amongst the youngand lower social-economic groups.[2, 68, 74]The pr<strong>in</strong>ciple <strong>of</strong> alcohol taxation reform most<strong>of</strong>ten discussed by public health advocatesis usually that <strong>of</strong> apply<strong>in</strong>g excise taxes to allcategories <strong>of</strong> alcoholic beverages. That is,tax<strong>in</strong>g the beverages on their alcohol content,as a mild discouragement <strong>of</strong> consumption.Along with taxation reform <strong>of</strong> this k<strong>in</strong>d, therehave been calls to raise the price <strong>of</strong> thecheapest forms <strong>of</strong> alcohol. This is referred toas the floor price <strong>of</strong> alcohol. Given that priceis be<strong>in</strong>g used as the lever, it is the floor pricethat should be given more attention <strong>in</strong> order toachieve a real shift <strong>in</strong> per capita consumption,rather than just product preference. With<strong>in</strong> thiscontext, it is important to acknowledge thatthe impact <strong>of</strong> any <strong>in</strong>crease <strong>in</strong> the floor pricefor alcohol will impact more on young people,Indigenous communities, heavy dr<strong>in</strong>kers andlower socio-economic groups.It appears that the most likely model thatcan effectively reduce alcohol-<strong>related</strong> harmwould be based on an across-the-boardexcise model that also <strong>in</strong>cludes regulat<strong>in</strong>g thefloor (m<strong>in</strong>imum) price, especially with regardto small conta<strong>in</strong>ers. The excise tax couldbe scaled with<strong>in</strong> different product types toensure there were strong f<strong>in</strong>ancial <strong>in</strong>centivesfor the production <strong>of</strong> lower alcohol products(for example, low-strength beer, w<strong>in</strong>e andRTDs), and so that the highest-risk alcoholproducts (i.e. spirits, which can more easilycause overdose) are taxed at an appropriatelyhigher rate. In comb<strong>in</strong>ation with a volumetrictaxation system, <strong>in</strong> which all products are taxedaccord<strong>in</strong>g to alcohol content, all productscould effectively have a floor price based ontheir alcohol content <strong>in</strong> a 300ml conta<strong>in</strong>er.Modell<strong>in</strong>g this alcohol taxation system would bea very challeng<strong>in</strong>g exercise, particularly whenhealth advocates have very limited access toactual sales data. As noted above, compet<strong>in</strong>g<strong>in</strong> the alcohol market requires extensive markettest<strong>in</strong>g and monitor<strong>in</strong>g. This generates a level<strong>of</strong> detailed <strong>in</strong>formation that is not availableto health researchers and policy makers.Perhaps just as importantly, this model wouldhave a negative impact on some segments– particularly cask w<strong>in</strong>e and cider – whileadvantag<strong>in</strong>g other market segments – spiritsand spirit-based RTD products. It would be verydifficult to ga<strong>in</strong> broad political support for sucha model, given the level <strong>of</strong> public and politicalopposition from powerful alcohol producers.There has been some modell<strong>in</strong>g undertakenthat considered a range <strong>of</strong> alcohol taxationscenarios that would move the alcohol exciseand taxation system closer to a true volumetricbase, while rema<strong>in</strong><strong>in</strong>g revenue neutral with<strong>in</strong>each market segment. These models are publiclyavailable, but have attracted limited supportas they <strong>in</strong>crease the price <strong>of</strong> cask w<strong>in</strong>e andciders while more expensive w<strong>in</strong>es are reduced<strong>in</strong> price.[36] Until public health researchers andadvocates have access to accurate sales data,and economic modell<strong>in</strong>g can be implementedon the comb<strong>in</strong>ation <strong>of</strong> floor price and a morevolumetric approach to alcohol taxation, itis difficult to strongly put forward a particularmodel. At the same time, there is a substantivehistory <strong>in</strong> <strong>Australia</strong> that illustrates the danger <strong>of</strong>chang<strong>in</strong>g taxation levels <strong>of</strong> particular productswithout consider<strong>in</strong>g the implications both onconsumption patterns and the developmentand market<strong>in</strong>g <strong>of</strong> alternative alcohol products.26
4.4 Dr<strong>in</strong>k-driv<strong>in</strong>g countermeasuresDr<strong>in</strong>k-driv<strong>in</strong>g laws and the associated programs<strong>of</strong> enforcement and social market<strong>in</strong>g areconsidered to be one <strong>of</strong> the great publichealth success stories <strong>of</strong> the late 20th century. In<strong>Australia</strong>, state and territory laws allow a Blood<strong>Alcohol</strong> Content (BAC) <strong>of</strong> up to 0.05% whiledriv<strong>in</strong>g for full licence holders, 0.00% for learnerdrivers and 0.00 per to 0.02% for provisionaldrivers, depend<strong>in</strong>g on the state or territory. Thosewho operate commercial aircraft, public orheavy vehicles, commercial vessels, mach<strong>in</strong>eryand mobile plant or farm equipment mustobserve the BAC restrictions required by theiremployer, as well as those required by law. Formost adults, dr<strong>in</strong>k<strong>in</strong>g no more than two standarddr<strong>in</strong>ks on an occasion will ma<strong>in</strong>ta<strong>in</strong> their BACbelow 0.05%. The evidence for the deterrenteffect <strong>of</strong> such laws is strong, although the effectscan erode over time and hence some countrieshave cont<strong>in</strong>ued to lower BAC limits.[13] From the1970s, <strong>Australia</strong>n states world leaders <strong>in</strong> driv<strong>in</strong>gdown rates <strong>of</strong> dr<strong>in</strong>k-driv<strong>in</strong>g through randombreath tests and other means.There is some evidence, albeit tentative, thathav<strong>in</strong>g lower BAC limits for young driversreduces the risk <strong>of</strong> road fatalities, especially ifthe BAC limit is 0.00%.[7] More broadly, there isgood evidence that lower BAC limits, delayedaccess to full licence and curfews for youngdrivers can be effective <strong>in</strong> reduc<strong>in</strong>g dr<strong>in</strong>k driv<strong>in</strong>gamong young people; graduated licens<strong>in</strong>gschemes can potentially <strong>in</strong>corporate all <strong>of</strong> thesemeasures with<strong>in</strong> a s<strong>in</strong>gle system.[13]Random breath test<strong>in</strong>g (RBT) has been shownto be effective <strong>in</strong> several countries, <strong>in</strong>clud<strong>in</strong>g<strong>Australia</strong>, <strong>in</strong> reduc<strong>in</strong>g road crashes, <strong>in</strong>juries andfatalities.[7] The def<strong>in</strong><strong>in</strong>g feature <strong>of</strong> RBT is thatany motorist at any time may be required totake a breast test, and there is noth<strong>in</strong>g theycan do to <strong>in</strong>fluence their chances <strong>of</strong> be<strong>in</strong>gtested.[13] Research suggests that there is astrong tendency for motorists to comply withdr<strong>in</strong>k-driv<strong>in</strong>g laws <strong>in</strong> jurisdictions that use RBTprograms because <strong>of</strong> the uncerta<strong>in</strong>ty aboutthe real risk <strong>of</strong> detection.[13] Here<strong>in</strong> lies part <strong>of</strong>the impressive cost effectiveness <strong>of</strong> randombreath test<strong>in</strong>g. RBT is considered a superiormethod <strong>of</strong> enforc<strong>in</strong>g dr<strong>in</strong>k-driv<strong>in</strong>g laws thansobriety checkpo<strong>in</strong>ts, which only check driverswho are judged to have been dr<strong>in</strong>k<strong>in</strong>g.[13] In<strong>Australia</strong>, creat<strong>in</strong>g the public perception thatthere is a high chance <strong>of</strong> be<strong>in</strong>g caught dr<strong>in</strong>kdriv<strong>in</strong>g through RBT has been achieved by acomb<strong>in</strong>ation <strong>of</strong> high-visibility polic<strong>in</strong>g (roadblocks, ‘booze buses’) and frequent socialmarket<strong>in</strong>g campaigns that emphasise thelikelihood <strong>of</strong> dr<strong>in</strong>k drivers be<strong>in</strong>g detected.[7]Among the range <strong>of</strong> punishments for dr<strong>in</strong>kdriv<strong>in</strong>g, the penalty that appears to havehad the most consistent impact is licencesuspension.[13] Increas<strong>in</strong>g the severity <strong>of</strong> f<strong>in</strong>esand impos<strong>in</strong>g penalties such as imprisonmentfor dr<strong>in</strong>k driv<strong>in</strong>g have not been shown to result <strong>in</strong>reduced rates <strong>of</strong> dr<strong>in</strong>k driv<strong>in</strong>g or car accidents.[13] However, it is estimated that up to 70% <strong>of</strong>people who lose their licence cont<strong>in</strong>ue to drivewhile unlicensed, as the risk <strong>of</strong> apprehensionis relatively low.[43] The major concerns withdisqualified drivers cont<strong>in</strong>u<strong>in</strong>g to drive arethat it underm<strong>in</strong>es the effectiveness <strong>of</strong> licencesuspension and is also l<strong>in</strong>ked to a range <strong>of</strong>other high-risk behaviour such as repeateddr<strong>in</strong>k driv<strong>in</strong>g and speed<strong>in</strong>g.[43] Court diversion<strong>of</strong> dr<strong>in</strong>k drivers to educative and mandatorytreatment <strong>in</strong>terventions and the <strong>in</strong>capacitation<strong>of</strong> vehicles us<strong>in</strong>g ignition <strong>in</strong>terlock devices areregarded as effective means <strong>of</strong> <strong>in</strong>creas<strong>in</strong>gcompliance with licence suspension andreduc<strong>in</strong>g recidivism.[7, 13]While there is no evidence that on-premisedesignated driver programs produce negativeeffects, the impact <strong>of</strong> such programs is verymodest and even with concerted promotionsthey only produce a small positive effect.[13]An <strong>Australia</strong>n review <strong>of</strong> these schemes wassomewhat more supportive, po<strong>in</strong>t<strong>in</strong>g to researchf<strong>in</strong>d<strong>in</strong>gs that the programs do have somepositive <strong>in</strong>fluence on the behaviour <strong>of</strong> youngpeople <strong>in</strong> select<strong>in</strong>g a sober driver, and thatgiven the cost <strong>of</strong> such programs is usually borneby licensed premises, there is no opportunitycost <strong>in</strong> recommend<strong>in</strong>g such schemes.[7]27
4.5 Treatment and early <strong>in</strong>terventionThis paper considers treatment and early<strong>in</strong>tervention as essential components <strong>of</strong>a preventative approach to the harmfulconsumption <strong>of</strong> alcohol. While treatment andprevention are traditionally viewed as separateand sometimes un<strong>related</strong> activities, it is criticalthat they be embraced as part <strong>of</strong> a holisticapproach to tackl<strong>in</strong>g alcohol problems froma public health perspective. While treatmentsare primarily designed to serve the needs <strong>of</strong><strong>in</strong>dividuals, there are a number <strong>of</strong> ways thattreatment can also have a positive impactat a whole-<strong>of</strong>-population level:nnnnBy rais<strong>in</strong>g public awareness<strong>of</strong> alcohol problemsInfluenc<strong>in</strong>g national andcommunity agendasInvolv<strong>in</strong>g health pr<strong>of</strong>essionals <strong>in</strong>advocacy for preventionProvid<strong>in</strong>g secondary benefits for families,employers and road users.[13]Brief <strong>in</strong>terventions <strong>in</strong> primary health sett<strong>in</strong>gs. Forearly-stage alcohol problems, brief <strong>in</strong>terventionsare consistently identified as a key <strong>in</strong>gredient <strong>in</strong>a comprehensive alcohol-prevention strategybecause they are regarded as relatively<strong>in</strong>expensive, they take very little time andthey can be implemented by a wide range<strong>of</strong> health and welfare pr<strong>of</strong>essionals.[7] Theirbenefit as preventative measures arises fromthe relative effectiveness <strong>in</strong> treat<strong>in</strong>g early-stageproblem dr<strong>in</strong>k<strong>in</strong>g, obviat<strong>in</strong>g the need for latermore <strong>in</strong>tense and costly treatment.[43] Brief<strong>in</strong>terventions are designed to motivate high-riskdr<strong>in</strong>kers to moderate their alcohol consumption,and typically <strong>in</strong>volve one to three sessions beforeor soon after the onset <strong>of</strong> problem dr<strong>in</strong>k<strong>in</strong>g.[13]In <strong>Australia</strong>, brief <strong>in</strong>terventions, as yet, are arelatively untapped opportunity, due <strong>in</strong> partto the need for greater recognition <strong>of</strong> the rolethat the primary health workforce can play.[43] Efforts dur<strong>in</strong>g the 1980s and early 1990s to<strong>in</strong>troduce more systematic screen<strong>in</strong>g, earlyidentification and potentially brief or extendedresponses were variously tried.These <strong>in</strong>cluded the Coord<strong>in</strong>ator <strong>of</strong> <strong>Alcohol</strong> andDrug Education <strong>in</strong> Medical Schools (CADEMS)that supported curriculum development forundergraduate medical students, a range<strong>of</strong> General Practice trials (especially <strong>in</strong> NewSouth Wales, sometimes <strong>in</strong> association withother specific <strong>in</strong>terventions <strong>in</strong>clud<strong>in</strong>g tobaccoand even efforts to develop a comb<strong>in</strong>ed riskscreen<strong>in</strong>g<strong>in</strong>strument for a number <strong>of</strong> conditions)and studies <strong>of</strong> the use <strong>of</strong> screen<strong>in</strong>g <strong>in</strong>struments(especially AUDIT) <strong>in</strong> hospital sett<strong>in</strong>gs. Follow-uphas been patchy, and even where the uptakeand utility under experimental conditions waspromis<strong>in</strong>g, the longer term effort and costrequired to achieve widespread <strong>in</strong>volvement hasnot been susta<strong>in</strong>ed. With a sense <strong>of</strong> déjà vu, theauthors note a recent study <strong>of</strong> the effectiveness<strong>of</strong> brief <strong>in</strong>terventions <strong>in</strong> hospital emergencydepartments, which suggests that these canpotentially reduce subsequent alcohol-<strong>related</strong><strong>in</strong>juries significantly.[75] For assessments andbrief <strong>in</strong>terventions to become part <strong>of</strong> rout<strong>in</strong>epractice <strong>of</strong> doctors, nurses and other healthpr<strong>of</strong>essionals, an approach at the healthsystem level accompanied by fund<strong>in</strong>gand promotion is needed. It is unrealisticto expect overstretched health serviceproviders to implement brief <strong>in</strong>terventionswithout reimbursement or other recognition.While this paper especially addresses primaryprevention, it is worth not<strong>in</strong>g that there rema<strong>in</strong>sa serious lack <strong>of</strong> accessible and availableevidence-based treatment services for laterstage alcohol dependence and other alcohol<strong>related</strong>disorders across <strong>Australia</strong> (<strong>in</strong> private andpublic as well as <strong>in</strong> city and remote locations).With a still evolv<strong>in</strong>g specialist cl<strong>in</strong>ical workforce,there rema<strong>in</strong>s a relative vacuum for tra<strong>in</strong><strong>in</strong>gand pr<strong>of</strong>essional development at senior cl<strong>in</strong>icallevels, and it is this group that ultimately set thestandard and nature <strong>of</strong> practice <strong>in</strong> any field.A comment from a senior cl<strong>in</strong>ician on the morerecent development <strong>of</strong> Medicare support forprivate practice GPs and cl<strong>in</strong>ical psychologistsis pert<strong>in</strong>ent: ‘it means that I get all these patientstreated under the mental health items withfundamental alcohol-<strong>related</strong> problemswhere alcohol was not properly managed’.28
Workplace <strong>in</strong>terventions. <strong>Australia</strong>n workplacesare another sett<strong>in</strong>g with great potential for brief<strong>in</strong>terventions with at risk dr<strong>in</strong>kers. There are twoma<strong>in</strong> rationales for workplace <strong>in</strong>terventionswith regard to the harmful consumption<strong>of</strong> alcohol: to improve productivity; and toimprove workplace safety.[7] In the <strong>Australia</strong>ncontext, approaches to workplace alcoholissues are <strong>in</strong>fluenced by occupational healthand safety laws and polices, and devis<strong>in</strong>gprevention strategies must be considered <strong>in</strong>this context. Historically, alcohol problems <strong>in</strong>the workplace have been dealt with throughemployee assistance programs (EAPs) andemployers’ policies on alcohol and drug use;however, there has been <strong>in</strong>sufficient researchto determ<strong>in</strong>e the effectiveness <strong>of</strong> EAPs <strong>in</strong>respond<strong>in</strong>g to and/or prevent<strong>in</strong>g alcoholissues <strong>in</strong> the workplace.[7] Nonetheless, EAPsdo provide the potential opportunity for<strong>in</strong>terventions that are known to be effective,such as brief <strong>in</strong>terventions for high-risk dr<strong>in</strong>kers.A recent study <strong>of</strong> alcohol consumptionby <strong>Australia</strong>n workers and the impact onabsenteeism has po<strong>in</strong>ted to the need forworkplace education to <strong>in</strong>fluence youngemployees’ attitudes and behaviours regard<strong>in</strong>galcohol use.[76] The study also suggests thatthere is a need to take a whole-<strong>of</strong>-workplaceapproach when design<strong>in</strong>g and implement<strong>in</strong>gprevention strategies that target both ‘problemdr<strong>in</strong>kers’ and workers who dr<strong>in</strong>k at short-termrisk levels, even <strong>in</strong>frequently, because thelatter have an elevated risk <strong>of</strong> alcohol-<strong>related</strong>workplace absenteeism.[76] Others havepo<strong>in</strong>ted to the need for address<strong>in</strong>g structuralfactors <strong>in</strong> the workplace as a more susta<strong>in</strong>ableprevention measure, such as reduc<strong>in</strong>g stressfulwork<strong>in</strong>g conditions that may lead to healthdamag<strong>in</strong>gbehaviour such as the harmfulconsumption <strong>of</strong> alcohol.[77]<strong>Alcohol</strong> problem treatment. Internationally, andparticularly <strong>in</strong> <strong>Australia</strong>, the evidence base withregard to the treatment <strong>of</strong> alcohol problems isvery well developed and is now at the stage<strong>of</strong> determ<strong>in</strong><strong>in</strong>g what is best practice ratherthan attempt<strong>in</strong>g to determ<strong>in</strong>e if treatmentcan work.[7] Effective alcohol treatmentoptions <strong>in</strong>clude motivational <strong>in</strong>terview<strong>in</strong>g, brief<strong>in</strong>terventions, social skills tra<strong>in</strong><strong>in</strong>g, communityre<strong>in</strong>forcement approach, relapse preventionand some aversion therapies.[7] There isevidence that mutual help programs such as12-Step Facilitation Therapy, which encouragesattendance at <strong>Alcohol</strong>ics Anonymous (AA)meet<strong>in</strong>gs, are particularly effective for severelydependent dr<strong>in</strong>kers with low levels <strong>of</strong> socialsupport.[7] Although popular and widelyused, there are also treatments that have littleevidence <strong>of</strong> efficacy, <strong>in</strong>clud<strong>in</strong>g <strong>in</strong>sight-orientatedpsychotherapy, confrontation counsell<strong>in</strong>g,relaxation tra<strong>in</strong><strong>in</strong>g, general ‘alcoholismcounsell<strong>in</strong>g’, education and milieu therapy.[7]Pharmacotherapies for alcohol dependence<strong>in</strong>clude disulfiram, naltrexone and acamprosate.Reviews have found that naltrexone andacamprosate are the safest and most effective<strong>of</strong> the three pharmacotherapies <strong>in</strong> the longand <strong>in</strong>termediate terms, respectively.[7]Thiam<strong>in</strong>e supplementation. A uniquepreventative measure to address the risk <strong>of</strong>serious bra<strong>in</strong> damage from thiam<strong>in</strong>e deficiency(known as Wernicke-Korsak<strong>of</strong>f’s syndrome)that can result from heavy consumption <strong>of</strong>alcohol over many years, along with poornutrition, is thiam<strong>in</strong>e supplementation. S<strong>in</strong>ce1991, all bak<strong>in</strong>g flour <strong>in</strong> <strong>Australia</strong> has beensupplemented with thiam<strong>in</strong>e as a universalmethod to <strong>in</strong>crease thiam<strong>in</strong>e levels <strong>in</strong> the diet<strong>of</strong> at risk populations.[7] This is <strong>in</strong>cluded hereas an example <strong>of</strong> a preventative measurethat requires ongo<strong>in</strong>g consideration, as therehas s<strong>in</strong>ce been advocacy for the removal <strong>of</strong>supplements (<strong>in</strong>clud<strong>in</strong>g thiam<strong>in</strong>e) by the purefood advocates and there is concern that thereach <strong>of</strong> thiam<strong>in</strong>e <strong>in</strong> bakers flour might not bethe most cost-effective population measure <strong>in</strong>prevent<strong>in</strong>g this condition.[78]S<strong>in</strong>ce the 1980s, sober<strong>in</strong>g-up centres havebeen established <strong>in</strong> many parts <strong>of</strong> <strong>Australia</strong>,particularly Indigenous communities, ashumane forms <strong>of</strong> care for publicly <strong>in</strong>toxicated<strong>in</strong>dividuals, and as an alternative to <strong>in</strong>dividualsbe<strong>in</strong>g arrested and held <strong>in</strong> police cells andwatch houses.[34]29
number <strong>of</strong> RSA tra<strong>in</strong><strong>in</strong>g programs have beenevaluated <strong>in</strong> <strong>Australia</strong>.[36] In addition to tra<strong>in</strong><strong>in</strong>gbar staff <strong>in</strong> the responsible service <strong>of</strong> alcohol,there have also been programs designed totra<strong>in</strong> staff <strong>in</strong> manag<strong>in</strong>g aggressive behaviour,given the reality that some patrons may havebecome already <strong>in</strong>toxicated elsewhere andthat some aggressive behaviour may not benecessarily alcohol-<strong>related</strong> at all.[13] There havebeen very few evaluations <strong>of</strong> such programs,although there is evidence that they canimprove staff and patron <strong>in</strong>teractions generally,but the long-term susta<strong>in</strong>ability <strong>of</strong> theseimprovements relies on ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g tra<strong>in</strong><strong>in</strong>gand standards <strong>of</strong> practice.[13]Proactive polic<strong>in</strong>g or <strong>in</strong>telligence-led polic<strong>in</strong>ghas been successful <strong>in</strong> some parts <strong>of</strong> theworld and has been partially adopted <strong>in</strong>some <strong>Australia</strong>n jurisdictions.[13] It <strong>in</strong>volvesmonitor<strong>in</strong>g alcohol-<strong>related</strong> <strong>in</strong>cidents <strong>in</strong> andaround licensed premises, comb<strong>in</strong>ed withregular police visits to the licensed premisesthat are most <strong>of</strong>ten l<strong>in</strong>ked to alcohol problems.For example, the New South Wales policehave adopted a system <strong>of</strong> enforc<strong>in</strong>g liquorlaws through the collection <strong>of</strong> data such asfeedback to police about alcohol-<strong>related</strong>crimes that have followed dr<strong>in</strong>k<strong>in</strong>g at aspecific licensed premises.[83] Known as the‘<strong>Alcohol</strong> L<strong>in</strong>k<strong>in</strong>g Program’, the <strong>in</strong>telligence-ledenforcement system has been shown to reducealcohol-<strong>related</strong> crime, and similar approachesare now be<strong>in</strong>g trialled and implemented <strong>in</strong>other jurisdictions.Voluntary codes <strong>of</strong> bar practice typically takethe form <strong>of</strong> ‘liquor accords’ <strong>in</strong> <strong>Australia</strong>. Theemergence <strong>of</strong> liquor accords as a means <strong>of</strong>reduc<strong>in</strong>g alcohol-<strong>related</strong> problems <strong>in</strong> late-nightenterta<strong>in</strong>ment centres began <strong>in</strong> Victoria <strong>in</strong> theearly 1990s, and s<strong>in</strong>ce then there has been arapid proliferation throughout several states.[36]Accords are local, community-based<strong>in</strong>itiatives to <strong>in</strong>volve licensees, other bus<strong>in</strong>esses,local government authorities, communityrepresentatives and police, but which areimplemented and largely coord<strong>in</strong>ated bythe latter to reduce alcohol-<strong>related</strong> harm<strong>in</strong> the late-night dr<strong>in</strong>k<strong>in</strong>g environment.[36]There are many possible components <strong>of</strong>accords, such as RSA, dr<strong>in</strong>k discount<strong>in</strong>g bans,tra<strong>in</strong>ed security personnel, provisions <strong>of</strong> food,use <strong>of</strong> safe glassware and alcohol conta<strong>in</strong>ers,and environmental modifications to reduceconflict and thereby reduce the risk <strong>of</strong> violence.[7] Few accords have been formally evaluated,and among those that have, most havebeen unable to demonstrate effectiveness<strong>in</strong> either the short- or (particularly) long-termreduction <strong>of</strong> alcohol-<strong>related</strong> harms.[36] Theappeal <strong>of</strong> accords probably rests more on thedevelopment <strong>of</strong> local communication networks,the facilitation <strong>of</strong> local <strong>in</strong>put, a sense <strong>of</strong> local‘control’ and improv<strong>in</strong>g public relations throughopen negotiations than <strong>in</strong> the actual reduction<strong>of</strong> harm. Even so, improved communicationand participation may also be perceived asdesirable and worthwhile outcomes <strong>in</strong> somecircumstances. Loxley et al. acknowledgethat there is no doubt that accords can bean effective vehicle for <strong>in</strong>troduc<strong>in</strong>g someharm-reduc<strong>in</strong>g practices <strong>in</strong>to licenseddr<strong>in</strong>k<strong>in</strong>g venues; however, it is recommendedthat voluntary regulation such as this isaccompanied by effective law enforcement.[7]The promotion <strong>of</strong> alcohol-free events, whilepopular <strong>in</strong> many countries, <strong>in</strong>clud<strong>in</strong>g <strong>Australia</strong>,has not been found on its own to be effective<strong>in</strong> reduc<strong>in</strong>g alcohol problems.[36] <strong>Alcohol</strong>restrictions for large sport<strong>in</strong>g and leisure eventshave usually been implemented as part <strong>of</strong>a range <strong>of</strong> <strong>in</strong>itiatives, mak<strong>in</strong>g it difficult todeterm<strong>in</strong>e their specific impact.[36] Based onevidence that some <strong>in</strong>juries from alcohol-<strong>related</strong>violence were l<strong>in</strong>ked to the use <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>gglasses and bottles as weapons, a number <strong>of</strong>licensed premises around the world now servealcohol only <strong>in</strong> toughened glass or plasticconta<strong>in</strong>ers.[13] However, the soundness <strong>of</strong> thisapproach has been called <strong>in</strong>to question by astudy that found that <strong>in</strong>juries to bar staff actually<strong>in</strong>creased when toughened glass was used.[13]Provid<strong>in</strong>g food service on premises that servealcohol, as a way <strong>of</strong> encourag<strong>in</strong>g eat<strong>in</strong>gwhile dr<strong>in</strong>k<strong>in</strong>g and hence reduc<strong>in</strong>g the effects<strong>of</strong> alcohol, is a popular element <strong>in</strong> liquoraccords.[7]31
However, the specific contribution <strong>of</strong> mak<strong>in</strong>gfood available on licensed premises as away <strong>of</strong> prevent<strong>in</strong>g <strong>in</strong>toxication has not beendeterm<strong>in</strong>ed, and <strong>in</strong> the case <strong>of</strong> certa<strong>in</strong> foods(for example, salty snacks) there may actuallybe a risk <strong>of</strong> the opposite effect on alcoholconsumption.[7]Community mobilisation has been used toraise awareness <strong>of</strong> problems associated withon-premises dr<strong>in</strong>k<strong>in</strong>g, develop specific solutionsto problems and pressure licensees to takeresponsibility for some <strong>of</strong> the impacts on thelocal community, such as noise, litter and antisocialbehaviour.[13] There is no set formula bywhich community action projects operate, aseach project has differ<strong>in</strong>g aims and objectives,<strong>of</strong>ten <strong>in</strong> response to localised problems.[36]Studies overseas support the view that whencommunity mobilisations are implemented ascomprehensive, evidence-based strategiesand are well funded, they can <strong>in</strong>fluence serverbehaviour, dr<strong>in</strong>k<strong>in</strong>g behaviour and levels <strong>of</strong>alcohol-<strong>related</strong> harms associated with licensedpremises.[36] Although some relatively smallcommunity mobilisation projects are currentlyunder way <strong>in</strong> <strong>Australia</strong>, results from evaluativestudies are yet to be published.[36] In general,community mobilisation approaches have atleast a temporary effect on licensed premises <strong>in</strong>terms <strong>of</strong> serv<strong>in</strong>g practices and patron behaviourbut <strong>in</strong> the longer term they <strong>of</strong>ten tend not to beimplemented <strong>in</strong> a systematic way, and prove tobe expensive and difficult to susta<strong>in</strong>.[13]4.7 Regulat<strong>in</strong>g promotion<strong>Alcohol</strong> market<strong>in</strong>g and promotion is aglobal activity, with the largest corporationspromot<strong>in</strong>g their products across the world.[13]Market<strong>in</strong>g strategies <strong>in</strong>clude an <strong>in</strong>tegratedmix <strong>of</strong> advertis<strong>in</strong>g on television, radio, pr<strong>in</strong>tmedia, po<strong>in</strong>t <strong>of</strong> sale promotions, productdesign (<strong>in</strong>clud<strong>in</strong>g the packag<strong>in</strong>g and nam<strong>in</strong>g<strong>of</strong> alcohol beverages) and the <strong>in</strong>ternet.Sponsorship <strong>of</strong> sports and cultural events is alsoa common market<strong>in</strong>g strategy used by alcoholcompanies, particularly <strong>in</strong> <strong>Australia</strong>. The keyquestions from a public perspective are:nnwhat is the impact <strong>of</strong> market<strong>in</strong>g andpromotion on overall consumptionand particularly the misuse <strong>of</strong> alcohol<strong>in</strong> the community?what are the most effective measures forprevent<strong>in</strong>g the adverse impacts <strong>of</strong> alcoholmarket<strong>in</strong>g and promotion?Total alcohol advertis<strong>in</strong>g expenditure <strong>in</strong><strong>Australia</strong> <strong>in</strong> 2007 was reported to be $128 million(see Table 8). However, this figure is highlyconservative, given that it generally relatesto the advertis<strong>in</strong>g <strong>of</strong> products rather than <strong>of</strong>alcohol outlets, for which alcohol advertis<strong>in</strong>gexpenditure is now very significant. Nordoes it <strong>in</strong>clude sponsorship, ‘below the l<strong>in</strong>e’advertis<strong>in</strong>g or <strong>in</strong>ternet advertis<strong>in</strong>g, the latterbe<strong>in</strong>g a significant growth area <strong>in</strong> recent years.In <strong>Australia</strong>, the ma<strong>in</strong> sectors <strong>in</strong> which alcoholadvert<strong>in</strong>g expenditure occurs, and throughwhich the greatest exposure is achieved, arethrough commercial television advertis<strong>in</strong>g (38%)and outdoor advertis<strong>in</strong>g (32%). Globalisedalcohol manufacturers (for example, Diageo;Pernod Ricard Pacific) are among the biggestspend<strong>in</strong>g advertisers <strong>in</strong> <strong>Australia</strong>. The amountspent on advertis<strong>in</strong>g by spirits and w<strong>in</strong>eproducers comb<strong>in</strong>ed, now equals that <strong>of</strong> thetraditionally dom<strong>in</strong>ant beer market <strong>in</strong> <strong>Australia</strong>,reflect<strong>in</strong>g an <strong>in</strong>creas<strong>in</strong>gly competitive alcoholbeverage market.32
Table 8: <strong>Alcohol</strong> advertis<strong>in</strong>g <strong>in</strong> <strong>Australia</strong> by sector, advertiser and beverage category, 2007SectorPercentageshareRank Advertiser$millionsAnnualchangeBeveragecategoryPercentageshareMetro TV 33% 1 Diageo 19.1 29% Beer 47%Regional TV 5% 2 Carlton & United14.4 -24% Spirits 26%BeveragesMetro press 5% 3 Tooheys Brewery 14.0 10% W<strong>in</strong>e 21%Regional1% 4 Boag J & Son 9.9 13% Premix /6%pressciderMagaz<strong>in</strong>es 14% 5 Pernod Ricard6.9 60%PacificRadio 5% 6 Ber<strong>in</strong>ger Blass W<strong>in</strong>e 5.3 93%EstatesC<strong>in</strong>ema 5% 7 Southcorp W<strong>in</strong>es 4.8 191%Outdoor 32% 8 Suntory 4.8 421%Direct mail 1% 9 Carlton Special4.7 238%Beverages10 He<strong>in</strong>eken 3.9 36%Others not <strong>in</strong> top 10 39.9 -5%Source: Nielsen Media Research AdEx 2008The impact <strong>of</strong> advertis<strong>in</strong>g on <strong>in</strong>dividuals can beseen as hav<strong>in</strong>g both immediate effects, suchas <strong>in</strong>fluenc<strong>in</strong>g decision mak<strong>in</strong>g with regard tobrand preference, as well as longer term effectssuch as re<strong>in</strong>forc<strong>in</strong>g pro-dr<strong>in</strong>k<strong>in</strong>g messages.[13] Inthis way, it is both the content and frequency <strong>of</strong>exposure to advertis<strong>in</strong>g that can have an impacton <strong>in</strong>dividuals’ attitudes and behaviours. Theimpact <strong>of</strong> alcohol advertis<strong>in</strong>g on young peopleis an area where there has been considerableresearch, but <strong>of</strong> somewhat poor quality, yield<strong>in</strong>gconflict<strong>in</strong>g results that range from positiveassociations between young people whohave been exposed to and/or enjoy alcoholadvertis<strong>in</strong>g and an <strong>in</strong>creased risk <strong>of</strong> harmfulconsumption <strong>of</strong> alcohol, to negative associationsor <strong>in</strong>conclusive results.[7] Numerous studieshave found a l<strong>in</strong>k between alcohol advertis<strong>in</strong>gand alcohol-<strong>related</strong> knowledge, beliefs and<strong>in</strong>tentions <strong>of</strong> young people.[84]Unlike tobacco advertis<strong>in</strong>g, which was banned<strong>in</strong> <strong>Australia</strong> <strong>in</strong> 1995, there are no alcoholadvertis<strong>in</strong>g bans <strong>in</strong> <strong>Australia</strong>, although somerestrictions, <strong>in</strong>clud<strong>in</strong>g advertis<strong>in</strong>g contentcontrols, do apply (see further below). In<strong>Australia</strong>, alcohol advertis<strong>in</strong>g is subject to anumber <strong>of</strong> different laws and codes <strong>of</strong> practice.The <strong>Australia</strong>n Association <strong>of</strong> NationalAdvertisers Code <strong>of</strong> Ethics covers generaladvertis<strong>in</strong>g issues. Other applicable laws andcodes <strong>in</strong>clude:nnnnnThe Trade Practices ActState and territory fair trad<strong>in</strong>g legislationThe Commercial Television IndustryCode <strong>of</strong> PracticeThe Commercial Radio Code <strong>of</strong> PracticeThe Outdoor Advertis<strong>in</strong>g Code <strong>of</strong> Ethics.The Commercial Television Industry Code <strong>of</strong>Practice states that advertisements can onlybe shown dur<strong>in</strong>g M, MA or AV classificationperiods. However, on weekends and publicholidays, alcohol advertisements can be shownas an accompaniment to the live broadcast<strong>of</strong> a sport<strong>in</strong>g event. <strong>Alcohol</strong> advertis<strong>in</strong>g iscovered <strong>in</strong> detail by the <strong>Alcohol</strong> BeveragesAdvertis<strong>in</strong>g Code (ABAC) Scheme. The ma<strong>in</strong>aims <strong>of</strong> the scheme are to ensure that alcoholadvertis<strong>in</strong>g presents a responsible approachto dr<strong>in</strong>k<strong>in</strong>g, and does not have appeal tochildren or adolescents. Among other rules <strong>in</strong>the code, the adm<strong>in</strong>istration <strong>of</strong> the follow<strong>in</strong>gis <strong>of</strong>ten questioned by community members:‘Advertisements for alcohol beverages must notdepict the consumption or presence <strong>of</strong> alcohol33
everages as a cause <strong>of</strong> or contribut<strong>in</strong>g tothe achievement <strong>of</strong> personal, bus<strong>in</strong>ess, social,sport<strong>in</strong>g, sexual or other success’ (ABAC 2008,Clause C (i)).[85]The ABAC Scheme is funded and adm<strong>in</strong>isteredentirely by the alcohol <strong>in</strong>dustry. Commonwealthand state and territory governments are <strong>in</strong>volvedthrough one government representative on theABAC Management Committee.Despite the ABAC Scheme’s rules, whichdiscourage advertis<strong>in</strong>g that has ‘strong orevident appeal to children or adolescents’,research shows that a substantial amount <strong>of</strong>alcohol advertis<strong>in</strong>g is communicated to youngpeople. For example, several advertisements foralcoholic beverages screened on television <strong>in</strong>metropolitan Melbourne were found to be morelikely to reach 13- to 17-year-olds than adults(see Table 9).Table 9: Advertis<strong>in</strong>g on metro Melbournetelevision, year to March 2005said or shown. It is estimated that only 3% <strong>of</strong> thetotal adult population are aware <strong>of</strong> the exist<strong>in</strong>gABAC scheme and know what it relates to.[87]Among the 30% <strong>of</strong> people who reported be<strong>in</strong>gconcerned about any alcohol advertis<strong>in</strong>g,only 2% had made a formal compla<strong>in</strong>t. Some<strong>of</strong> the reasons why those who were concerneddid not make a compla<strong>in</strong>t <strong>in</strong>cluded the beliefthat it would not achieve anyth<strong>in</strong>g (30%), nothav<strong>in</strong>g time (25%) and not know<strong>in</strong>g who/how/where to compla<strong>in</strong> (15%). ABAC currently hasno powers to sanction advertisers who breachthe code rules; however, a Senate Committee<strong>in</strong>quiry currently under way is consider<strong>in</strong>gproposed federal legislation that would<strong>in</strong>troduce sanctions on advertisers who breachthe code, which would be determ<strong>in</strong>ed by an<strong>in</strong>dependent adjudicat<strong>in</strong>g panel.[88]In 2003, the M<strong>in</strong>isterial Council on Drug Strategyconsidered a report on the effectiveness <strong>of</strong>the ABAC Scheme that identified the follow<strong>in</strong>gissues <strong>of</strong> concern:ProductHe<strong>in</strong>ekenLagerCougarBourbonArchersSpriSchnappsBundabergRum Dry &Lime MixOrlandoJacobsCreekSparkl<strong>in</strong>gRoseTotalannualspendSource: K<strong>in</strong>g, Taylor and Carroll (2005)[86]Frequency<strong>of</strong> adsRelativeexposure(<strong>of</strong> 13–17-years-oldsVs 18–29-year-olds)$ 94,000 110 1.12$ 45,000 103 1.04$ 57,000 110 1.04$ 36,000 88 1.06$ 89,000 34 1.11As a self-regulatory scheme, ABAC’seffectiveness largely depends on the<strong>in</strong>dependence <strong>of</strong> its compla<strong>in</strong>ts body withthe powers to sanction.[43] Recent researchhas revealed that less than three <strong>in</strong> 10 (28%)people surveyed reported an awareness<strong>of</strong> restrictions or regulations cover<strong>in</strong>g theadvertis<strong>in</strong>g <strong>of</strong> alcohol, <strong>in</strong> terms <strong>of</strong> what can bennnnnThe current system does not address publichealth concerns about alcohol advertis<strong>in</strong>gand use. In particular, most compla<strong>in</strong>tsabout alcohol advertis<strong>in</strong>g are dealt withunder the general advertis<strong>in</strong>g compla<strong>in</strong>tsresolution system rather than the alcoholspecificsystem.The high dismissal rate for compla<strong>in</strong>ts aboutalcohol advertisements heard by the ASBdoes not engender community confidence<strong>in</strong> the compla<strong>in</strong>t system and maydiscourage people from mak<strong>in</strong>g compla<strong>in</strong>tsabout alcohol advertisements.The general public is largely unaware <strong>of</strong>the compla<strong>in</strong>t resolution system and, <strong>in</strong>particular, how to make compla<strong>in</strong>ts.The system lacks transparency. In particular,there is <strong>in</strong>sufficient report<strong>in</strong>g <strong>of</strong> theoutcomes <strong>of</strong> compla<strong>in</strong>ts.The current system does not apply to allforms <strong>of</strong> advertis<strong>in</strong>g; for example, packag<strong>in</strong>g,electronic advertis<strong>in</strong>g, sponsorships, po<strong>in</strong>t <strong>of</strong>sale advertis<strong>in</strong>g and promotions.34
nThe effectiveness <strong>of</strong> the current systemis compromised by the amount <strong>of</strong> timetaken to resolve compla<strong>in</strong>ts (MCDS 2003,unpublished).While some <strong>of</strong> these concerns have beenaddressed, pressure rema<strong>in</strong>s to move to a moretightly regulated advertis<strong>in</strong>g environment withstrict government controls. The WHO recentlyrecommended that governments be supported:nnnto effectively regulate the market<strong>in</strong>g <strong>of</strong>alcoholic beverages, <strong>in</strong>clud<strong>in</strong>g effectiveregulation or bann<strong>in</strong>g <strong>of</strong> advertis<strong>in</strong>g and <strong>of</strong>sponsorship <strong>of</strong> cultural and sports events,<strong>in</strong> particular those that have an impact onyounger peopleto designate statutory agencies to beresponsible for monitor<strong>in</strong>g and enforcement<strong>of</strong> market<strong>in</strong>g regulationsto work together to explore establish<strong>in</strong>g amechanism to regulate the market<strong>in</strong>g <strong>of</strong>alcoholic beverages, <strong>in</strong>clud<strong>in</strong>g effectiveregulation or bann<strong>in</strong>g <strong>of</strong> advertis<strong>in</strong>g andsponsorship, at the global level.One <strong>of</strong> the most formidable obstacles toeffective education and persuasion strategiesregard<strong>in</strong>g alcohol (which are discussed <strong>in</strong> thenext section below) is product advertis<strong>in</strong>g by thealcohol <strong>in</strong>dustry that <strong>in</strong>tentionally promotes prodr<strong>in</strong>k<strong>in</strong>gmessages to the general population,much <strong>of</strong> which also reaches young people. Inresponse, the governments <strong>of</strong> some countrieshave sponsored counter-advertis<strong>in</strong>g programs.[13] These might <strong>in</strong>clude public servicesannouncements, or warn<strong>in</strong>g messages with<strong>in</strong>actual product advertisements. However,studies suggest that counter-advertis<strong>in</strong>g usuallyhas only limited effectiveness, <strong>of</strong>ten becauseit is communicated at low frequencies and <strong>in</strong>poorer quality productions compared to alcoholbeverage advertis<strong>in</strong>g.[13] In contrast, counteradvertis<strong>in</strong>g <strong>in</strong> the tobacco field is <strong>of</strong> proveneffectiveness, primarily because <strong>in</strong> that contexthard-hitt<strong>in</strong>g messages were possible (essentiallythat the tobacco <strong>in</strong>dustry was not <strong>in</strong> bus<strong>in</strong>essfor the consumer’s good). Counter advertis<strong>in</strong>gmay be a more politically realistic option thanbann<strong>in</strong>g advertis<strong>in</strong>g altogether, and shouldbe strongly supported from a public healthperspective, but it is important that its messagenot be compromised. Although rare, there areexamples <strong>of</strong> well-planned and implementedcounter-advertis<strong>in</strong>g programs that have hadsome success, particularly <strong>in</strong> build<strong>in</strong>g support forpublic health-oriented alcohol controls,[13] andthere is very strong evidence from other publichealth areas such as tobacco about the value<strong>of</strong> such approaches.4.8 Education and persuasionInternational reviews <strong>of</strong> education andpersuasion strategies suggest that even withadequate resources, such approaches havelimited potential for success on their own.[13]Part <strong>of</strong> the reason for this is the counter effect<strong>of</strong> powerful forces that underp<strong>in</strong> unsafe andunhealthy dr<strong>in</strong>k<strong>in</strong>g cultures, such as the price,availability and promotion <strong>of</strong> alcohol products.Recent <strong>Australia</strong>n research for the development<strong>of</strong> a national alcohol social market<strong>in</strong>g <strong>in</strong>itiativereports that ‘the challenge for communicationis that <strong>in</strong>toxication is closely l<strong>in</strong>ked to alcoholper se. When we simply asked participantsabout their earliest memories <strong>in</strong> relation toalcohol there was an overwhelm<strong>in</strong>g tendencyto leap to their first drunk experience. Further,these experiences were recalled with a sense<strong>of</strong> pride and nostalgia, even though the stories<strong>in</strong>evitably <strong>in</strong>volved some embarrassment.’[89]A key element to the success <strong>of</strong> socialmarket<strong>in</strong>g <strong>in</strong> the public health area is effective<strong>in</strong>tegration with and re<strong>in</strong>forcement by othercomplementary strategies.[7] For <strong>in</strong>stance,the success <strong>of</strong> social market<strong>in</strong>g <strong>in</strong> promot<strong>in</strong>gquitt<strong>in</strong>g smok<strong>in</strong>g and road safety, <strong>in</strong>clud<strong>in</strong>ganti-dr<strong>in</strong>k-driv<strong>in</strong>g campaigns, is <strong>in</strong>dicative thateducation and persuasion strategies can beeffective when coupled with other measuressuch as support services, changes to theenvironment, regulation and enforcement.Throughout the world, alcohol education <strong>in</strong>schools is an enormously popular approach toaddress<strong>in</strong>g the issue <strong>of</strong> harmful consumption <strong>of</strong>alcohol among young people. The traditionalalcohol education programs that are based35
on an <strong>in</strong>formational approach, while still verycommon, have not been shown to prevent orreduce the harmful consumption <strong>of</strong> alcohol byyoung people, and <strong>in</strong> some cases have actuallybeen counterproductive by stimulat<strong>in</strong>g an<strong>in</strong>terest <strong>in</strong> dr<strong>in</strong>k<strong>in</strong>g among young people.[13]In recent years, there has been a shift towardsnormative education, which aims to correctyoung people’s perceptions about their peers’dr<strong>in</strong>k<strong>in</strong>g and thus de-normalise the harmfulconsumption <strong>of</strong> alcohol.[13] While this makes<strong>in</strong>tuitive sense, it has been found that suchschool-based educational <strong>in</strong>terventions, <strong>in</strong>general, produce only modest results that areshort-lived unless accompanied by ongo<strong>in</strong>gbooster sessions. Importantly, given there areconsiderable risks <strong>in</strong>volved <strong>in</strong> school-basededucation, it has been recommended that<strong>in</strong>vestment <strong>in</strong> such programs be accompaniedby a proportionate <strong>in</strong>vestment <strong>in</strong> evaluation.[7]There are some examples <strong>of</strong> sound outcomesbut these are relatively unusual. These generally<strong>in</strong>volve whole-<strong>of</strong>-community efforts and theyare usually associated with a close evaluationthat ensures they are implemented (withmodifications through feedback) as planned. In<strong>Australia</strong>, these <strong>in</strong>clude the School <strong>Health</strong> and<strong>Harm</strong> Reduction Project (SHAHRP) <strong>in</strong> Western<strong>Australia</strong>[43] and the Gatehouse Project <strong>in</strong>Victoria, whose primary target was reducedschool bully<strong>in</strong>g but where the side benefit wasa comparative reduction <strong>in</strong> the use <strong>of</strong> tobaccoand alcohol.[90] Related to alcohol educationprograms for school students are parenteducation programs. While some reviews citepromis<strong>in</strong>g signs <strong>of</strong> effectiveness, <strong>in</strong> general thererema<strong>in</strong>s a lack <strong>of</strong> research to fully determ<strong>in</strong>e thevalue <strong>of</strong> such programs.[7]Low-risk dr<strong>in</strong>k<strong>in</strong>g guidel<strong>in</strong>es have beenadopted <strong>in</strong> many countries, <strong>in</strong>clud<strong>in</strong>g <strong>Australia</strong>,to provide advice on the health risks andbenefits <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g at various levels for thegeneral adult population, and for particularsub-groups. Despite their popularity, thereis very little research that demonstrates theeffectiveness <strong>of</strong> guidel<strong>in</strong>es.[13]However, guidel<strong>in</strong>es do potentially fulfil animportant function as support<strong>in</strong>g <strong>in</strong>formationfor other measures known to be effective,such as brief <strong>in</strong>terventions <strong>in</strong> primary care, andas the basis for health promotion messagesand social market<strong>in</strong>g campaigns. In <strong>Australia</strong>,the current alcohol guidel<strong>in</strong>es.[91] are underreview. New draft guidel<strong>in</strong>es prepared forpublic consultation are due to be f<strong>in</strong>alised andreleased <strong>in</strong> late 2008. The new draft guidel<strong>in</strong>eshave been <strong>in</strong>formed by updated modell<strong>in</strong>gon the health risks <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g, which haveproduced new estimates <strong>of</strong> the lifetime risks<strong>of</strong> alcohol-<strong>related</strong> harm. Emerg<strong>in</strong>g evidencealso <strong>in</strong>dicates that previous studies claim<strong>in</strong>gthe significant health benefits <strong>of</strong> alcoholconsumption have tended to overestimate theeffects. The consultation draft <strong>in</strong>dicates thema<strong>in</strong> changes are expected to <strong>in</strong>clude a newsimplified, universal guidel<strong>in</strong>e level for alcohol<strong>in</strong>take for both short-term and long-term risks,a new guidel<strong>in</strong>e with special precautions forchildren and adolescents, and a new guidel<strong>in</strong>efor pregnant or breastfeed<strong>in</strong>g women.[18]Warn<strong>in</strong>g labels on alcohol products, while notrequired <strong>in</strong> <strong>Australia</strong>, have a high level <strong>of</strong> publicsupport. Evaluations <strong>of</strong> alcohol warn<strong>in</strong>g labelsare generally limited to the US experience,where labels were implemented <strong>in</strong> 1989. Whilethere is some evidence <strong>of</strong> effects on knowledgeand attitudes, there is no evidence that warn<strong>in</strong>glabels <strong>in</strong>fluence dr<strong>in</strong>k<strong>in</strong>g behaviour.[92] Bycontrast, the tobacco labell<strong>in</strong>g experience<strong>of</strong>fers strong evidence that warn<strong>in</strong>g labels canbe effective, not only <strong>in</strong> <strong>in</strong>creas<strong>in</strong>g <strong>in</strong>formationand chang<strong>in</strong>g attitudes but also <strong>in</strong> chang<strong>in</strong>gbehaviour. These successes <strong>of</strong> tobacco warn<strong>in</strong>glabels suggest that alcohol warn<strong>in</strong>g labelsshould be graphic and attention-gett<strong>in</strong>g,should occupy a considerable portion <strong>of</strong> thepackage surface, and should <strong>in</strong>volve rotat<strong>in</strong>gand chang<strong>in</strong>g messages.[92] Perhaps mostimportantly, they should complement and becomplemented by a wider range <strong>of</strong> strategiesaimed at chang<strong>in</strong>g dr<strong>in</strong>k<strong>in</strong>g behaviour.36
5. Policy imperatives5.1 The state <strong>of</strong> alcoholpolicy <strong>in</strong> <strong>Australia</strong>A recent report by the WHO warns that ‘thedifference between good and bad alcoholpolicy is not an abstraction, but very <strong>of</strong>ten amatter <strong>of</strong> life and death’.[13] Nonetheless, it isacknowledged <strong>in</strong>ternationally that ‘alcoholpolicy is <strong>of</strong>ten the product <strong>of</strong> compet<strong>in</strong>g<strong>in</strong>terests, values and ideologies’, and henceis not always based entirely on scientificevidence.[13] More specifically, the culturalsignificance <strong>of</strong> alcohol <strong>in</strong> many societies,along with its economic importance andthe political <strong>in</strong>fluence wielded by the globaland domestic alcohol beverage <strong>in</strong>dustries,create a hostile environment for public healthpolices, especially those aimed at reduc<strong>in</strong>gconsumption overall as a way <strong>of</strong> prevent<strong>in</strong>gand reduc<strong>in</strong>g alcohol-<strong>related</strong> harm.While we can see that it is politically necessaryto have ‘collaborative and cohesive’ alcoholpolicy where all <strong>in</strong>terested parties are<strong>in</strong>cluded, this poses significant impedimentsto the implementation <strong>of</strong> the most effectivepreventative <strong>in</strong>terventions. Notwithstand<strong>in</strong>gthis, <strong>Australia</strong> has been assessed as be<strong>in</strong>gcomparatively progressive and among the best<strong>in</strong> the world <strong>in</strong> terms <strong>of</strong> evidence-based alcoholpolicy.[93] In a recent commentary on nationalalcohol control policies <strong>in</strong> 18 countries, Baborand W<strong>in</strong>stanley [94] report that ‘contrary tothe generally pessimistic reports about alcoholpolicies, the case <strong>of</strong> <strong>Australia</strong> provides causefor optimism’. This assessment probably speaksto the relative low level <strong>of</strong> well-<strong>in</strong>tegratedpolicies globally, rather than an opportunity forcomplacency <strong>in</strong> <strong>Australia</strong>.Stockwell (2004:[42]) has judged that whilethere are ‘some significant disappo<strong>in</strong>tments’,there are also ‘some wonderful examples <strong>of</strong>successful <strong>Australia</strong>n public policies aroundalcohol from the past two decades’. Amongthe population-wide strategies that havebeen successful <strong>in</strong> reduc<strong>in</strong>g alcohol-<strong>related</strong>harm <strong>in</strong> <strong>Australia</strong>, Stockwell highlights taxationand dr<strong>in</strong>k-driv<strong>in</strong>g legislation/enforcement. Forhigh-risk groups, the compulsory fortification <strong>of</strong>bakers flour with thiam<strong>in</strong>e and liquor licens<strong>in</strong>grestrictions <strong>in</strong> some Indigenous communitiesare considered as successes. Among thestrategies not likely to have been effective,Stockwell po<strong>in</strong>ts to the dissem<strong>in</strong>ation <strong>of</strong>national dr<strong>in</strong>k<strong>in</strong>g guidel<strong>in</strong>es, the <strong>in</strong>troduction<strong>of</strong> standard dr<strong>in</strong>k labell<strong>in</strong>g on alcoholconta<strong>in</strong>ers, and efforts to encourage GPs todeliver brief <strong>in</strong>terventions and advice aboutlow-risk dr<strong>in</strong>k<strong>in</strong>g. Stockwell also underl<strong>in</strong>essome significant ‘setbacks’ <strong>in</strong> <strong>Australia</strong>nalcohol policy, such as the relaxation <strong>of</strong>liquor licens<strong>in</strong>g laws, which has led to theproliferation <strong>of</strong> outlets <strong>in</strong> many <strong>Australia</strong>njurisdictions; changes to the tax rate on w<strong>in</strong>e,which has encouraged the production andharmful consumption <strong>of</strong> cheap w<strong>in</strong>e; and,s<strong>in</strong>ce 1997, the <strong>in</strong>ability <strong>of</strong> states and territories<strong>in</strong> <strong>Australia</strong> to collect levies on the sale <strong>of</strong>alcohol products.The recent review <strong>of</strong> alcohol policies <strong>in</strong> 30OECD nations rated <strong>Australia</strong> as fifth overall,beh<strong>in</strong>d Norway (1st), Poland, Iceland andSweden.[93] The study rated the state <strong>of</strong>alcohol policy <strong>in</strong> each <strong>of</strong> the 30 countries bycreat<strong>in</strong>g a composite score based on theextent to which the country had adoptedpolices <strong>in</strong> various policy doma<strong>in</strong>s such as thephysical availability <strong>of</strong> alcohol, prices, dr<strong>in</strong>k<strong>in</strong>gcontext, alcohol advertis<strong>in</strong>g and road safety.37
The study also exam<strong>in</strong>ed the relationshipbetween each country’s score and per capitaalcohol consumption, and found a strongnegative correlation that implied a decrease<strong>in</strong> consumption <strong>of</strong> 1 litre <strong>of</strong> alcohol per yearfor each 10-po<strong>in</strong>t <strong>in</strong>crease <strong>in</strong> the score. Inother words, as alcohol policies <strong>in</strong>creased<strong>in</strong> strength (i.e. effectiveness), alcoholconsumption decreased.S<strong>in</strong>ce the late 1980s, <strong>Australia</strong> has adoptedseveral national strategies to tackle the harmfulconsumption <strong>of</strong> alcohol. <strong>Australia</strong>’s first nationalalcohol strategy was completed <strong>in</strong> 1989 [95]followed by subsequent <strong>in</strong>erations <strong>in</strong> 1996, [96]2001, [97] and most recently <strong>in</strong> 2006.[6] If thesuccess <strong>of</strong> these strategies is to be measured onthe basis <strong>of</strong> any change <strong>in</strong> rates <strong>of</strong> overall percapita dr<strong>in</strong>k<strong>in</strong>g, rates <strong>of</strong> adult b<strong>in</strong>ge dr<strong>in</strong>k<strong>in</strong>g,rates <strong>of</strong> underage dr<strong>in</strong>k<strong>in</strong>g, and outcomessuch as hospitalisations and crime, then thesestrategies appear to have had only modestsuccess. One <strong>Australia</strong>n commentator hassaid that ‘while these documents provide thebasis for a coherent and legitimate nationalapproach to alcohol there has been poorfollow-through on implementation’.[98]A recent summary <strong>of</strong> the state <strong>of</strong> alcohol policy<strong>in</strong> <strong>Australia</strong> reported that ‘what is needednow is not so much an understand<strong>in</strong>g <strong>of</strong> whatworks, but an appreciation <strong>of</strong> how to makeit work <strong>in</strong> the various contexts <strong>in</strong> which it isimplemented’[43] [emphasis added]. Essentially,even the most effective strategies <strong>in</strong> the worldwill not be effective if they are not properlyimplemented as <strong>in</strong>tended.5.2 The best mix <strong>of</strong> <strong>in</strong>terventionsWhile some <strong>in</strong>terventions are more effectivethan others, there is no s<strong>in</strong>gle strategy thatcan <strong>of</strong>fer a ‘quick fix’ or ‘silver bullet’ to theprevention <strong>of</strong> harmful consumption <strong>of</strong> alcohol.The review undertaken by Babor et al. (2003)[13] concludes that an <strong>in</strong>tegrated approachis required that <strong>in</strong>cludes a comb<strong>in</strong>ation <strong>of</strong>the strategies that are known to be effectiveand suitable for the particular context <strong>in</strong>which they are to be implemented. The NDRIemphasises[36] that it is important to considerthe quality, rather than the quantity, <strong>of</strong><strong>in</strong>terventions. For example, ‘a s<strong>in</strong>gle targetedrestriction (for example, hotel clos<strong>in</strong>g atmidnight) may be more effective than anentire suite <strong>of</strong> half-heartedly implemented,watered-down or ill-considered restrictions’.[36]Importantly, choos<strong>in</strong>g high-quality <strong>in</strong>terventionsdoes not mean choos<strong>in</strong>g the most expensive. Infact, many <strong>of</strong> the most effective strategies arethe cheapest.A recent analysis <strong>of</strong> studies <strong>in</strong>to the costeffectiveness <strong>of</strong> various alcohol-preventionmeasures found that there are very substantialdifferences <strong>in</strong> costs and effects, both between<strong>in</strong>terventions and between world regions.See Table 10.[99] Random breath test<strong>in</strong>g (dueto the need for regular sobriety checkpo<strong>in</strong>tsadm<strong>in</strong>istered by police) and brief advice <strong>in</strong>primary care (the <strong>in</strong>tervention itself, plus costsassociated with tra<strong>in</strong><strong>in</strong>g) are the most costly<strong>in</strong>terventions to achieve equivalent sav<strong>in</strong>gs <strong>in</strong>years <strong>of</strong> health, expressed as disability-adjustedlife years (DALYs) With regard to taxation, costeffectiveness appears to depend <strong>in</strong> part on theefficiency <strong>of</strong> the tax system and the degree <strong>of</strong>anti-dr<strong>in</strong>k<strong>in</strong>g sentiment. In the Americas andEurope, where like <strong>Australia</strong>, the prevalence <strong>of</strong>heavy dr<strong>in</strong>k<strong>in</strong>g is high, taxation was the mosteffective and cost-efficient strategy. However,by contrast, tax is actually least effective andleast efficient <strong>in</strong> South East Asia, where lowrates <strong>of</strong> heavy dr<strong>in</strong>k<strong>in</strong>g appear to favour moretargeted approaches such as random breathtest<strong>in</strong>g and brief physician advice.[99]38
Table 10: Cost-effectiveness (average cost per DALY) <strong>of</strong> <strong>in</strong>terventions for reduc<strong>in</strong>g the burden <strong>of</strong>alcohol <strong>in</strong> three WHO sub-regions (at different levels <strong>of</strong> economic development)Intervention Americas Europe South East AsiaBrief physician advice 776 2,612 856Random breath test<strong>in</strong>g 1,919 2,741 701Excise tax (current) 364 370 5,420Excise tax (current + 20%) 326 321 7,414Excise tax (current + 50%) 297 287 9,418Reduced retail access 484 1,208 1,406Comprehensive ad ban 536 660 1,807Source: Chisholm et al. (2006)[99]A more recent, <strong>Australia</strong>n-based study hasidentified the <strong>in</strong>terventions for which strong<strong>Australia</strong>n or <strong>in</strong>ternational evidence exists as totheir potential benefits, and has attempted toevaluate these benefits <strong>in</strong> terms <strong>of</strong> the reduction<strong>in</strong> the social costs <strong>of</strong> alcohol-<strong>related</strong> harm itwould be possible to achieve.[100] Interventionsidentified as be<strong>in</strong>g effective and for whichbenefits are quantifiable, <strong>in</strong>clude:nHigher alcohol taxation, <strong>in</strong>clud<strong>in</strong>gdifferential tax rates on forms <strong>of</strong> alcoholthat are particularly subject to abuseThe study estimates that through the adoption<strong>of</strong> these <strong>in</strong>terventions it would be possible toachieve a 48% reduction <strong>in</strong> alcohol-attributabledeaths, along with significant reductions<strong>in</strong> the social costs <strong>of</strong> alcohol-<strong>related</strong> harm.These <strong>in</strong>clude a $5.94 billion sav<strong>in</strong>g from higheralcohol taxation, a $5.83 billion sav<strong>in</strong>g from brief<strong>in</strong>terventions, a $2.45 billion sav<strong>in</strong>g from partialadvertis<strong>in</strong>g and market<strong>in</strong>g controls, and a$0.94 billion sav<strong>in</strong>g from greater enforcement<strong>of</strong> dr<strong>in</strong>k-drive laws.nnnPartial or complete bans on theadvertis<strong>in</strong>g and promotion <strong>of</strong> alcoholMeasures to reduce dr<strong>in</strong>k driv<strong>in</strong>g: more<strong>in</strong>tensive enforcement <strong>of</strong> random breathtest<strong>in</strong>g and lower<strong>in</strong>g the legal bloodalcohol concentration (BAC) levelBrief <strong>in</strong>terventions by primary carephysicians to reduce hazardousalcohol consumption.39
5.3 Challenges <strong>in</strong> implementation<strong>Australia</strong>’s <strong>in</strong>ternational score card <strong>in</strong> thearea <strong>of</strong> alcohol policy appears to be quiteimpressive, as the reviews mentioned abovetestify, and many would argue that <strong>in</strong>crementalpolicy change, rather than radical approaches,is the most appropriate way to proceed.However, some have cautioned aga<strong>in</strong>st tak<strong>in</strong>gcomfort <strong>in</strong> this approach because <strong>of</strong> the‘cultural <strong>in</strong>ertia’ surround<strong>in</strong>g alcohol policy <strong>in</strong><strong>Australia</strong>, which can be a formidable barrierto mean<strong>in</strong>gful policy changes. ‘Dr<strong>in</strong>k<strong>in</strong>g formspart <strong>of</strong> the <strong>Australia</strong>n legend, and there is goodprecedent <strong>in</strong> <strong>Australia</strong>n history to suggest that aradical alcohol reform agenda could provokecommunity backlash – beware the ‘wowser’label’.[98] An example <strong>of</strong> radical policy changethat has been successful is the <strong>in</strong>troduction <strong>of</strong>random breath test<strong>in</strong>g, thanks <strong>in</strong> part to theaccompany<strong>in</strong>g social market<strong>in</strong>g campaignsthat have highlighted both the seriousness <strong>of</strong>the problem and the effectiveness <strong>of</strong> the policyresponse. The level <strong>of</strong> public support <strong>in</strong> <strong>Australia</strong>for new alcohol policy <strong>in</strong>terventions and/or theextension <strong>of</strong> exist<strong>in</strong>g <strong>in</strong>terventions is encourag<strong>in</strong>g<strong>in</strong> some areas (see Fig. 14); for example, the level<strong>of</strong> public support for measures known to beeffective, such as the strict monitor<strong>in</strong>g <strong>of</strong> latenightlicensed premises (75%), is relatively high.While support for measures such as <strong>in</strong>creas<strong>in</strong>gtax on alcohol to pay for health, education andthe treatment <strong>of</strong> alcohol-<strong>related</strong> problems isrelatively lower (41%), it is a reasonably sufficientbase <strong>of</strong> public support on which to buildthrough public education and social market<strong>in</strong>gabout the rationale and potential benefits <strong>of</strong>such a measure.Figure 14. Support for alcohol measures,proportion <strong>of</strong> the population aged14+ years, <strong>Australia</strong>, 2007Source: AIHW 2008[2]40
There are some specific challenges that gobeyond public understand<strong>in</strong>g and attitudes.These have been raised throughout this paperand <strong>in</strong>clude:nnnNational Competition Policy, as it relates toliquor licens<strong>in</strong>g systems, regulat<strong>in</strong>g alcoholprices and restrict<strong>in</strong>g alcohol promotionsThe division <strong>of</strong> responsibilities between levels<strong>of</strong> governments for key alcohol policy areasand the historic complexity <strong>in</strong> achiev<strong>in</strong>gcoord<strong>in</strong>ated actionThe economic and political importance,and thus <strong>in</strong>fluence, <strong>of</strong> the alcohol beverageand <strong>related</strong> <strong>in</strong>dustries.These challenges arise <strong>in</strong> the context <strong>of</strong> broad,community-wide changes <strong>in</strong> the nature <strong>of</strong> work,education and social connectedness, andoccur at a time when:nnn<strong>Alcohol</strong> sponsorship <strong>of</strong> sport<strong>in</strong>g andcultural activities has replaced and isnow prom<strong>in</strong>ent <strong>in</strong> many areas previouslyoccupied by the tobacco <strong>in</strong>dustry.<strong>Alcohol</strong> consumption is symbolicallyassociated with positive and pleasurablelife <strong>in</strong> portrayals <strong>of</strong> <strong>Australia</strong>’s history andculture, <strong>in</strong>clud<strong>in</strong>g the ongo<strong>in</strong>g promotion<strong>of</strong> alcohol as a necessary <strong>in</strong>gredient <strong>of</strong>enterta<strong>in</strong>ment, celebration and all ‘rite <strong>of</strong>passage’ life course transitions.The ‘menu’ <strong>of</strong> psychoactive andperformance-enhanc<strong>in</strong>g substancesis <strong>in</strong>creas<strong>in</strong>g <strong>in</strong> scope and complexitywith<strong>in</strong> a society that is encouraged t<strong>of</strong>ocus on pleasure and performance, andwhere alcohol is seen, comparatively,as the ‘known’ commodity and thus‘unchallengeable’ (or at least acceptable).nnnnnThe debate regard<strong>in</strong>g the positive healthbenefits <strong>of</strong> small doses <strong>of</strong> alcohol makesforthright messages for social market<strong>in</strong>gpurposes awkward and less memorable,and where compromise is extracted <strong>in</strong>every effort to implement effective alcoholharm prevention measures.Intoxicated behaviour is regarded by manycommunity members as ‘normal’ and bymany young people as desirable.The significantly lower life expectancy <strong>of</strong>Indigenous people is <strong>in</strong>tr<strong>in</strong>sically l<strong>in</strong>kedto layered aetiology, <strong>in</strong>clud<strong>in</strong>g historicand structural issues, social and serviceexclusion, patterns <strong>of</strong> alcohol consumption,where there is great sensitivity to progress<strong>in</strong>gevidence-based approaches <strong>in</strong> somecommunities and where the consequentimmobilisation and <strong>in</strong>action from thebroader society is the most ready response.There is a parallel dilemma <strong>of</strong> too muchtoo fast, and the possibility <strong>of</strong> even greaterbroad dysfunction if not managed carefully.‘Consumer’ is a complex concept <strong>in</strong> thisfield. It can <strong>in</strong>clude both alcohol consumers(who generally seek liberal access to theirfavoured drug) and service users who arevery <strong>of</strong>ten extremely reluctant to seek ‘help’.Those who experience the ‘second-hand’effects <strong>of</strong> harmful consumption <strong>of</strong> alcoholare a somewhat untapped group (<strong>in</strong>clud<strong>in</strong>gparents, who are the most identifiable group,but extend<strong>in</strong>g well beyond this sub-category).The extent and level <strong>of</strong> detail <strong>of</strong> dataavailable precludes the evaluation <strong>of</strong>the outcomes <strong>of</strong> the <strong>in</strong>cremental andplanned changes to the levers that<strong>in</strong>fluence alcohol-consumption patterns,and patterns <strong>of</strong> <strong>related</strong> harm over the pastdecades, and similarly make effectivemodell<strong>in</strong>g or assessment <strong>of</strong> the likely impact<strong>of</strong> future directed changes <strong>in</strong>complete andthus less reliable.41
nnWhile there are few well-qualifiedspecialists, there are many middlemanag<strong>in</strong>ghealth and welfare personnelimplement<strong>in</strong>g <strong>in</strong>terventions that theysometimes have little faith <strong>in</strong>, and theconcomitant low expectations <strong>of</strong> successwith patients or clients can be self-fulfill<strong>in</strong>g.In this context there is now good evidence<strong>of</strong> what works and we know that treatment,for example, can be successful. Althoughmany will agree with this statement, few <strong>in</strong>the respond<strong>in</strong>g <strong>in</strong>dustry seem to believe itor lack the skills to utilise the most effectivemeans to achieve it.The views <strong>of</strong> community members tend tobe closer to the alcohol beverage <strong>in</strong>dustries’preferred preventative approaches, such asadvocat<strong>in</strong>g for measures <strong>in</strong>clud<strong>in</strong>g schoolbasedalcohol education, the responsibleservice <strong>of</strong> alcohol tra<strong>in</strong><strong>in</strong>g, parent supportand <strong>in</strong>formation, and education programsfor specific target populations on fetalalcohol effects.5.4 Opportunities for actionReflect<strong>in</strong>g on the evidence regard<strong>in</strong>g thedeterm<strong>in</strong>ants <strong>of</strong> harmful consumption <strong>of</strong>alcohol, as gleaned from the review <strong>of</strong><strong>in</strong>terventions earlier <strong>in</strong> this paper, is perhapsa start<strong>in</strong>g po<strong>in</strong>t for consider<strong>in</strong>g what thepriorities for action should be. In general:nnnnWhen alcohol availability <strong>in</strong>creases,alcohol-<strong>related</strong> harms are likely to <strong>in</strong>creaseWhen alcohol availability decreases,alcohol-<strong>related</strong> harms are likely to decreaseWhen alcohol prices decrease <strong>in</strong> real terms,alcohol-<strong>related</strong> harms are likely to <strong>in</strong>creaseWhen alcohol prices <strong>in</strong>crease <strong>in</strong> realterms, alcohol-<strong>related</strong> harms are likelyto decrease.In summary, chang<strong>in</strong>g the physical andeconomic availability <strong>of</strong> alcohol is probably themost effective and reliable way <strong>of</strong> reduc<strong>in</strong>g theharmful consumption <strong>of</strong> alcohol.As the NDRI (2007) suggests, ‘where the ultimateaim <strong>of</strong> decision makers is to m<strong>in</strong>imise or reducethe negative impact <strong>of</strong> alcohol on the publichealth, safety and amenity <strong>of</strong> a population,best practice is that which is evidence-basedand at very least, avoids implement<strong>in</strong>gchanges likely to <strong>in</strong>crease overall availabilityabove the current status quo’.Government decision mak<strong>in</strong>g relat<strong>in</strong>g to theavailability <strong>in</strong> <strong>Australia</strong>, whether it be liquorlicens<strong>in</strong>g decisions or changes to the exciserates <strong>of</strong> particular alcohol products, tends tobe reactionary. As an alternative, NDRI (2007)suggests that ‘authorities and decision makersmight consider adopt<strong>in</strong>g a pro-active style –one which acknowledges the l<strong>in</strong>ks betweenalcohol availability and harms and which plansaccord<strong>in</strong>gly. Optimally, such an approachwould: <strong>in</strong>clude policy and strategies basedon sound research evidence for efficacyand/or have a solid theoretical ground<strong>in</strong>g;<strong>in</strong>clude processes which support the ongo<strong>in</strong>g,systematic collection <strong>of</strong> detailed objective datafor monitor<strong>in</strong>g and evaluation purposes; employevaluation f<strong>in</strong>d<strong>in</strong>gs to <strong>in</strong>form and supportfuture evidence-based decisions and reliablemonitor<strong>in</strong>g <strong>of</strong> community sentiment.’Of course, ‘supply reduction’ measures thatrestrict availability are not the s<strong>in</strong>gle solutionto address<strong>in</strong>g the harmful consumption<strong>of</strong> alcohol – harm reduction and demandreduction measures are also important andvery necessary. Ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g and build<strong>in</strong>gon <strong>Australia</strong>’s impressive track record <strong>in</strong>dr<strong>in</strong>k-driv<strong>in</strong>g countermeasures is an obviouselement to <strong>in</strong>clude <strong>in</strong> an overall preventativestrategy, but it should not be taken for granted,especially given the powerful cultural forcessurround<strong>in</strong>g alcohol <strong>in</strong> <strong>Australia</strong> that couldunderm<strong>in</strong>e, stall or, worse still, reverse thega<strong>in</strong>s made <strong>in</strong> prevent<strong>in</strong>g and reduc<strong>in</strong>galcohol-<strong>related</strong> road <strong>in</strong>juries and fatalities. Brief<strong>in</strong>terventions are known to be one <strong>of</strong> the mosteffective preventative measures and more workis needed to exam<strong>in</strong>e the most appropriatesett<strong>in</strong>g for such an approach. Along with theusual health sett<strong>in</strong>gs considered, workplacesprovide a w<strong>in</strong>dow <strong>of</strong> opportunity for reach<strong>in</strong>g42
thousands <strong>of</strong> <strong>Australia</strong>ns at the early stages<strong>of</strong> problematic dr<strong>in</strong>k<strong>in</strong>g. This also opens anopportunity for novel partnerships. The success <strong>of</strong>prevention <strong>in</strong> other areas <strong>of</strong> public health, suchas tobacco control, tells us that social market<strong>in</strong>gis a key element that is necessary to <strong>in</strong>form targetaudiences, shift attitudes and positively re<strong>in</strong>forcebehaviour changes be<strong>in</strong>g driven by othercomplementary measures, such as restrictionson availability, regulation and enforcement.5.5 PrioritiesThe <strong>in</strong>tent <strong>of</strong> this paper has been to providebackground <strong>in</strong>formation about alcohol-<strong>related</strong>harm <strong>in</strong> <strong>Australia</strong>, and summarise <strong>in</strong>ternationalbest practice <strong>in</strong> alcohol-prevention policiesand programs, rather than to articulate aparticular course <strong>of</strong> action. However, somepriorities for preventative policies and programs,and for research, are most important and mosturgent, and should be s<strong>in</strong>gled out, becausethey represent a gap <strong>in</strong> current practiceor knowledge <strong>in</strong> <strong>Australia</strong> or because theywould enhance and/or <strong>in</strong>form exist<strong>in</strong>g andnew practices. In the first <strong>in</strong>stance, the majorimperatives for <strong>Australia</strong> are to:1. Reshape consumer demand towardssafer dr<strong>in</strong>k<strong>in</strong>g through:nnManag<strong>in</strong>g both the physical availability(access) and economic availability(price). The high accessibility <strong>of</strong> alcohol– <strong>in</strong> terms <strong>of</strong> outlet open<strong>in</strong>g hours, density<strong>of</strong> alcohol outlets and discount<strong>in</strong>g<strong>of</strong> alcohol products – is an issue <strong>in</strong> many<strong>Australia</strong>n communities.Address<strong>in</strong>g the cultural place <strong>of</strong> alcohol.Carefully planned, targeted andresearch-based social market<strong>in</strong>g andpublic education are required, and willbe more effective if the market<strong>in</strong>g <strong>of</strong>alcoholic beverages is restricted, <strong>in</strong>clud<strong>in</strong>gcurb<strong>in</strong>g advertis<strong>in</strong>g and sponsorship<strong>of</strong> cultural and sport<strong>in</strong>g events.2. Reshape supply towards lower-riskproducts through:nnChanges to the current taxation regimeto stimulate the production andconsumption <strong>of</strong> low-alcohol products.Improved enforcement <strong>of</strong> current legislativeand regulatory measures (such asResponsible Serv<strong>in</strong>g <strong>of</strong> <strong>Alcohol</strong> or banson serv<strong>in</strong>g <strong>in</strong>toxicated persons andm<strong>in</strong>ors, or cont<strong>in</strong>u<strong>in</strong>g to lower the bloodalcohol content <strong>in</strong> dr<strong>in</strong>k-driv<strong>in</strong>g laws).3. Strengthen, skill and support primaryhealth care to help people <strong>in</strong> mak<strong>in</strong>ghealthy choices:nSupport<strong>in</strong>g brief <strong>in</strong>terventions as part <strong>of</strong>rout<strong>in</strong>e practice by health pr<strong>of</strong>essionalsand other health workers <strong>in</strong> primaryhealthcare sett<strong>in</strong>gs can assist changes<strong>in</strong> dr<strong>in</strong>k<strong>in</strong>g behaviour and attitudesto alcohol consumption. This supportshould <strong>in</strong>clude consideration <strong>of</strong> build<strong>in</strong>gappropriate reimbursements and other<strong>in</strong>centives <strong>in</strong>to health system fund<strong>in</strong>g.4. Close the gap for disadvantagedcommunities:nThere is a need for tailored approachesand services to reach Indigenous andother disadvantaged groups.5. Improve the evaluation <strong>of</strong><strong>in</strong>terventions through:nnMonitor<strong>in</strong>g and evaluation <strong>of</strong> regulatorymeasures and other programsto underp<strong>in</strong> the further evolution <strong>of</strong>prevention strategies directed at <strong>in</strong>appropriatealcohol consumption.Develop<strong>in</strong>g effective models <strong>of</strong> saferpatterns <strong>of</strong> alcohol consumption <strong>in</strong> differentcommunities through changesto alcohol taxation arrangements, andan understand<strong>in</strong>g <strong>of</strong> the impact <strong>of</strong> differenttypes <strong>of</strong> alcohol outlets and theirdensity on hospitalisation, violenceand crime rates.43
References1. <strong>Australia</strong>n Institute <strong>of</strong> <strong>Health</strong> and Welfare. 2007 NationalDrug Strategy Household Survey: State and territorysupplement. Drug Statistics Series No. 21, Cat. no. PHE102. Canberra: <strong>Australia</strong>n Institute <strong>of</strong> <strong>Health</strong> and Welfare2008. Available from: www.aihw.gov.au/publications/<strong>in</strong>dex.cfm/title/106702. <strong>Australia</strong>n Institute <strong>of</strong> <strong>Health</strong> and Welfare. 2007 NationalDrug Strategy Household Survey: first results. DrugStatistics Series, Number 20. Canberra: <strong>Australia</strong>nInstitute <strong>of</strong> <strong>Health</strong> and Welfare, 2008a. Available from:www.aihw.gov.au/publications/phe/ndshs07-fr/ndshs07-fr-no-questionnaire.pdf3. Begg S, Vos T, Barker DC, Stanley L and Lopez A.Burden <strong>of</strong> disease and <strong>in</strong>jury <strong>in</strong> <strong>Australia</strong> <strong>in</strong> the newmillenium: measur<strong>in</strong>g health loss from diseases, <strong>in</strong>juriesand risk factors. Medical Journal <strong>of</strong> <strong>Australia</strong>. 2007;188:36−40. Available from: www.mja.com.au/public/issues/188_01_070108/beg10596_fm.html4. Coll<strong>in</strong>s D and Lapsley H. The costs <strong>of</strong> tobacco, alcoholand illicit drug abuse to <strong>Australia</strong>n society <strong>in</strong> 2004/05.P3 2625. Canberra: <strong>Department</strong> <strong>of</strong> <strong>Health</strong> and Age<strong>in</strong>g,2008. Available from: www.nationaldrugstrategy.gov.au/<strong>in</strong>ternet/drugstrategy/publish<strong>in</strong>g.nsf/Content/mono64/$File/mono64.pdf5. <strong>Australia</strong>n National Council on Drugs. Of substance.April 2008.6. M<strong>in</strong>isterial Council on Drug Strategy. Towards saferdr<strong>in</strong>k<strong>in</strong>g cultures: national alcohol strategy 2006–2009.Canberra: M<strong>in</strong>isterial Council on Drug Strategy, 2006.7. Loxley W, Toumbourou JW, Stockwell T, Ha<strong>in</strong>es B, ScottK, Godfrey C, et al. The prevention <strong>of</strong> substance use,risk and harm <strong>in</strong> <strong>Australia</strong>: a review <strong>of</strong> the evidence.Canberra: Commonwealth <strong>of</strong> <strong>Australia</strong>, 2004. Availablefrom: http://espace.lis.curt<strong>in</strong>.edu.au/archive/00000284/8. Hadfield P. Bar Wars. Oxford: Oxford University Press, 2007.9. Rudd K. National b<strong>in</strong>ge dr<strong>in</strong>k<strong>in</strong>g strategy – mediarelease. Canberra, 2008. Available from: www.pm.gov.au/media/Release/2008/media_release_0126.cfm10. Council <strong>of</strong> <strong>Australia</strong>n Governments. Communiqué – 21stMeet<strong>in</strong>g <strong>of</strong> the Council <strong>of</strong> <strong>Australia</strong>n Governments,23 March 2008. Council <strong>of</strong> <strong>Australia</strong>n Governments,2008, [viewed]. Available from: www.coag.gov.au/meet<strong>in</strong>gs/260308/<strong>in</strong>dex.htm11. M<strong>in</strong>isterial Council on Drug Strategy. 23 May 2008communiqué. Canberra: M<strong>in</strong>isterial Council on DrugStrategy, 2008.12. Hall W, Chikritzhs T, d’Abbs P and Room R. <strong>Alcohol</strong> salesdata are essential for good public policies towardsalcohol. The Medical Journal <strong>of</strong> <strong>Australia</strong>. 2008;189:188−9. Available from: www.mja.com.au/public/issues/189_04_180808/hal10593_fm.html13. Babor T, Caetano R, Casswell S, Edwards G, GiesbrechtG, Grube J, et al. <strong>Alcohol</strong>: no ord<strong>in</strong>ary commodity. NewYork: World <strong>Health</strong> Organization and Oxford UniversityPress, 2003.14. World <strong>Health</strong> Organization. World <strong>Health</strong> OrganisationStatistical Information System (WHOSIS) 2008. Availablefrom: www.who.<strong>in</strong>t/whosis/whostat/2008/en/<strong>in</strong>dex.html15. <strong>Australia</strong>n Institute <strong>of</strong> <strong>Health</strong> and Welfare. Submissionto Inquiry <strong>in</strong>to Ready-to-Dr<strong>in</strong>k <strong>Alcohol</strong> Beverages,Senate Community Affairs Committee. Drug StatisticsSeries, Number 20. Canberra: <strong>Australia</strong>n Institute <strong>of</strong><strong>Health</strong> and Welfare, 2008b. Available from: www.aihw.gov.au/publications/phe/ndshs07-fr/ndshs07-fr-noquestionnaire.pdf16. Stockwell T, Zhao J, Chikritzhs T and Greenfield T. Whatdid you dr<strong>in</strong>k yesterday? Public health relevance <strong>of</strong>a recent recall method used <strong>in</strong> the 2004 <strong>Australia</strong>nNational Drug Strategy Household Survey. Addiction.2008; 103:919–28.17. <strong>Australia</strong>n Bureau <strong>of</strong> Statistics and <strong>Australia</strong>n Institute<strong>of</strong> <strong>Health</strong> and Welfare. The health and welfare <strong>of</strong><strong>Australia</strong>’s Aborig<strong>in</strong>al and Torres Strait Islander People’s2005. Cat No. 4704.0. Canberra: <strong>Australia</strong>n Bureau <strong>of</strong>Statistics and <strong>Australia</strong>n Institute <strong>of</strong> <strong>Health</strong> and Welfare,2005. Available from: www.aihw.gov.au/publications/<strong>in</strong>dex.cfm/title/1017218. National <strong>Health</strong> and Medical Research Council.<strong>Australia</strong>n alcohol guidel<strong>in</strong>es for low-risk dr<strong>in</strong>k<strong>in</strong>g.Canberra: National <strong>Health</strong> and Medical ResearchCouncil, 2007. Available from: www.nhmrc.gov.au/guidel<strong>in</strong>es/_files/draft_australian_alcohol_guidel<strong>in</strong>es.pdf19. Begg S, Vos T, Barker B, Stevenson C, Stanley L andLopez A. The burden <strong>of</strong> disease and <strong>in</strong>jury <strong>in</strong> <strong>Australia</strong>2003. PHE 82. Canberra: <strong>Australia</strong>n Institute <strong>of</strong> <strong>Health</strong>and Welfare, 2007. Available from: www.aihw.gov.au/publications/<strong>in</strong>dex.cfm/title/1031720. Connor J, Broad J and Rehm J. The burden <strong>of</strong> death,disease, and disability due to alcohol <strong>in</strong> New Zealand.The New Zealand Medical Journal. 2005; 118:U1412.Available from: www.nzma.org.nz/journal/118-1213/1412/45
21. Chikritzhs T, Catalano P, Stockwell T, Donath S, Ngo H,Young D, et al. <strong>Australia</strong>n alcohol <strong>in</strong>dicators, 1990–2001:patterns <strong>of</strong> alcohol use and <strong>related</strong> harms for <strong>Australia</strong>nstates and territories. National Drug Research Institute,Curt<strong>in</strong> University <strong>of</strong> Technology and Turn<strong>in</strong>g Po<strong>in</strong>t, <strong>Alcohol</strong>and Drug Centre Inc., 2003. Available from: www.ndri.curt<strong>in</strong>.edu.au/pdfs/naip/naipaaiexecsumm.pdf22. Jackson R, Broad J, Connor J and Wells S. <strong>Alcohol</strong>and ischaemic heart disease: probably no freelunch. The Lancet. 2005; 366:1911−2. Availablefrom: www.thelancet.com/journals/lancet/article/PIIS0140673605677707/abstract23. Fillmore K, Kerr W and Stockwell T. Moderate alcoholuse and reduced mortality risk: systematic error <strong>in</strong>prospective studies. Addiction Research & Theory. 2006;14:101−32. Available from: www.<strong>in</strong>gentaconnect.com/content/tandf/gart/2006/00000014/00000002/art0000224. Royal College <strong>of</strong> Obstetricians and Gynaecologists(RCOG). <strong>Alcohol</strong> consumption and the outcomes<strong>of</strong> pregnancy. Statement No. 5. Royal College<strong>of</strong> Obstetricians and Gynaecologists (RCOG),2006. Available from: www.rcog.org.uk/<strong>in</strong>dex.asp?PageID=147725. O’Leary CM, Heuzenroeder L and Elliott EJ. A review <strong>of</strong>policies on alcohol use dur<strong>in</strong>g pregnancy <strong>in</strong> <strong>Australia</strong>and other English speak<strong>in</strong>g countries. The MedicalJournal <strong>of</strong> <strong>Australia</strong>. 2007; 186:466−71. Available from:www.mja.com.au/public/issues/186_09_070507/ole11155_fm.html26. Dawe S, Harnett P and Frye S. Improv<strong>in</strong>g outcomesfor children liv<strong>in</strong>g <strong>in</strong> families with parental substancemisuse: What do we know and what should we do.Child Prevention Issues. Melbourne: <strong>Australia</strong>n Institute<strong>of</strong> Family Studies, 2008. Available from: www.aifs.gov.au/nch/pubs/issues/issues29/issues29.html27. Government <strong>of</strong> Victoria <strong>Department</strong> <strong>of</strong> HumanServices. An <strong>in</strong>tegrated strategy for child protectionand placement services. Melbourne: CommunityCare Division 2002. Available from: www.cyf.vic.gov.au/policy-plann<strong>in</strong>g-fund<strong>in</strong>g/library/publications/<strong>in</strong>tegrated_strategy28. English DR, Holman CDJ and Milne E. The quantification<strong>of</strong> drug caused morbidity and mortality <strong>in</strong> <strong>Australia</strong>,1995. Canberra: Commonwealth <strong>Department</strong> <strong>of</strong> HumanServices and <strong>Health</strong>, 2005.29. Steer<strong>in</strong>g Committee for the Review <strong>of</strong> GovernmentService Provision. Overcom<strong>in</strong>g <strong>in</strong>digenousdisadvantage key <strong>in</strong>dicators 2005 report. Melbourne:Productivity Commission, 2005. Available from: http://papers.ssrn.com/sol3/papers.cfm?abstract_id=92577630. Matthews S, Chikritzhs T, Catalano P, Stockwell Tand Donath S. Trends <strong>in</strong> alcohol-<strong>related</strong> violence <strong>in</strong><strong>Australia</strong>,1991/92–1999/00. National <strong>Alcohol</strong> IndicatorsBullet<strong>in</strong> No.5. Melbourne: National Drug ResearchInstitute and Turn<strong>in</strong>g Po<strong>in</strong>t <strong>Alcohol</strong> and Drug Centre, 2002.31. Doherty S and Roche A. <strong>Alcohol</strong> and licensed premises:best practice <strong>in</strong> polic<strong>in</strong>g. A monograph for policeand policy makers. Adelaide: Australasian Centre forPolic<strong>in</strong>g Research, 2003. Available from: www.nceta.fl<strong>in</strong>ders.edu.au/pdf/licensed-premises/licencedpremises.pdf32. Briscoe S and Donnelly N. Assaults on Licensed Premises<strong>in</strong> Inner- Urban Areas. Sydney: New South Wales Bureau<strong>of</strong> Crime Statistics and Research, 2001.33. BOCSAR. Estimat<strong>in</strong>g the short-term cost <strong>of</strong> police timespent deal<strong>in</strong>g with alcohol-<strong>related</strong> crime <strong>in</strong> NSW, .Monograph No. 25. Canberra: National Drug LawEnforcement Research Fund, 2008.34. Chikritzhs T and Brady M. Fact or fiction? A critique <strong>of</strong>the National Aborig<strong>in</strong>al and Torres Strait Islander SocialSurvey 2002. Drug and <strong>Alcohol</strong> Review. 2006; 25:277−87.Available from: www.<strong>in</strong>formaworld.com/smpp/content~db=all?content=10.1080/0959523060064471535. <strong>Australia</strong>n Institute <strong>of</strong> <strong>Health</strong> and Welfare. National DrugStrategy Household Survey 2004 – detailed f<strong>in</strong>d<strong>in</strong>gs.AIWH Cat. No. PHE 66. Canberra: <strong>Australia</strong>n Institute <strong>of</strong><strong>Health</strong> and Welfare, 2005. Available from: www.aihw.gov.au/publications/<strong>in</strong>dex.cfm/title/1019036. National Drug Research Institute. Restrictions on the saleand supply <strong>of</strong> alcohol: evidence and outcomes. Perth:National Drug Research Institute, Curt<strong>in</strong> University <strong>of</strong>Technology, 2007. Available from: www.ndri.curt<strong>in</strong>.edu.au/pdfs/publications/R207.pdf37. Chikritzhs T, Stockwell T, Heale P, Dietze P and WebbM. Trends <strong>in</strong> alcohol-<strong>related</strong> road <strong>in</strong>jury <strong>in</strong> <strong>Australia</strong>,1990–1997. National <strong>Alcohol</strong> Indicators Bullet<strong>in</strong> No. 2.Perth and Melbourne: National Drug Research Instituteand Turn<strong>in</strong>g Po<strong>in</strong>t <strong>Alcohol</strong> and Drug Centre, 2000.38. Chikritzhs T and Pascal R. Trends <strong>in</strong> youth alcoholconsumption and <strong>related</strong> harms <strong>in</strong> <strong>Australia</strong>njurisdictions 1990–2002. National <strong>Alcohol</strong> IndicatorsBullet<strong>in</strong> No. 6. Perth: National Drug Research Institute,Curt<strong>in</strong> University <strong>of</strong> Technology, 2004. Available from:www.ndri.curt<strong>in</strong>.edu.au/pdfs/naip/naip006.pdf39. Room R and Liv<strong>in</strong>gston M. Variation by age <strong>in</strong> the harmper dr<strong>in</strong>k<strong>in</strong>g volume and heavier dr<strong>in</strong>k<strong>in</strong>g occasion.Melbourne: AER Centre for <strong>Alcohol</strong> Policy Research,Turn<strong>in</strong>g Po<strong>in</strong>t <strong>Alcohol</strong> and Drug Centre, 2007.40. Liv<strong>in</strong>gston M. Recent trends <strong>in</strong> risky alcohol consumptionand <strong>related</strong> harm aga<strong>in</strong>st young people <strong>in</strong> Victoria,<strong>Australia</strong>. <strong>Australia</strong>n and New Zealand Journal <strong>of</strong> Public<strong>Health</strong>. 2008; 32:266–27.46
41. Toumbourou J, Lyons Z, Loxley W and Bauld C. Researchneeds analysis and action plan for drug preventionresearch <strong>in</strong> Victoria. <strong>Department</strong> <strong>of</strong> Human Services,Victoria, Premier’s Drug Prevention Council, 2007.42. Stockwell T. <strong>Australia</strong>n alcohol policy and the public<strong>in</strong>terest: a brief report card. Drug and <strong>Alcohol</strong> Review.2004; 23:377–9. Available from: www.<strong>in</strong>formaworld.com/smpp/content~db=all?content=10.1080/0959523041233132449143. Loxley W, Gray D, Wilk<strong>in</strong>son C, Chikritzhs T, Midford Rand Moore D. <strong>Alcohol</strong> policy and harm reduction <strong>in</strong><strong>Australia</strong>. Drug and <strong>Alcohol</strong> Review. 2005; 24:559–68.Available from: www.<strong>in</strong>formaworld.com/smpp/content~db=all?content=10.1080/0959523050040413744. Chikritzhs T and Stockwell T. The impact <strong>of</strong> later trad<strong>in</strong>ghours for hotels on levels <strong>of</strong> impaired driver road crashesand driver breath alcohol levels. Addiction. 2006;1254–64.45. Chikritzhs T, Catalano P, Pascal R and Henrickson N.Predict<strong>in</strong>g alcohol-<strong>related</strong> harms from licensed outletdensity: a feasibility study. Monograph Series No. 28.Hobart: National Drug Law Enforcement ResearchFund, 2007. Available from: www.ndlerf.gov.au/pub/Monograph_28.pdf46. Donnelly N, Poynton S, Weatherburn D, Bamford E andNottage J. Liquor outlet concentrations and alcohol<strong>related</strong>neighbourhood problems. <strong>Alcohol</strong> StudiesBullet<strong>in</strong>. Sydney: NSW Bureau <strong>of</strong> Crime Statistics andResearch, 2006. Available from: www.lawl<strong>in</strong>k.nsw.gov.au/lawl<strong>in</strong>k/bocsar/ll_bocsar.nsf/vwFiles/ab08.pdf/$file/ab08.pdf47. Liv<strong>in</strong>gston M. <strong>Alcohol</strong> outlet density and assault: aspatial analysis. Addiction. 2008; 103:619−28. Availablefrom: www3.<strong>in</strong>terscience.wiley.com/journal/119411938/abstract48. Liv<strong>in</strong>gston M. A longitud<strong>in</strong>al analysis <strong>of</strong> alcohol outletdensity and assault. <strong>Alcohol</strong>: Cl<strong>in</strong>ical and ExperimentalResearch. 2008; 32:1074−9. Available from: www3.<strong>in</strong>terscience.wiley.com/journal/120084012/abstract49. Liv<strong>in</strong>gstone M. Recent trends <strong>in</strong> risky alchol consumptionand <strong>related</strong> harm amongst young people <strong>in</strong> Victoria.submitted for publication. 2008.50. Weitzman E, Folkman A, Folkman K and Wechsler H.The relationship <strong>of</strong> alcohol outlet density to heavy andfrequent dr<strong>in</strong>k<strong>in</strong>g and dr<strong>in</strong>k<strong>in</strong>g-<strong>related</strong> problems amongcollege students at eight universities. <strong>Health</strong> Place.2003; 9:1–6.51. Gruenewald P and Ponicki W. The relationship <strong>of</strong> theretail availability <strong>of</strong> alcohol and alcohol sales to alcohol<strong>related</strong>traffic crashes. Accid Anal Prev. 1995; 27.52. Cohen D, Ghosh-Dastidar B, Scribner RA, Miu A, Scott Mand Rob<strong>in</strong>son P. <strong>Alcohol</strong> outlets, gonorrhea, and the LosAngeles civil unrest: a longitud<strong>in</strong>al analysis. Soc Sci Med2006; 62.53. LaScala E, Johnson F and Gruenewald P. Neighborhoodcharacteristics <strong>of</strong> alcohol-<strong>related</strong> pedestrian <strong>in</strong>jurycollisions: a geostatistical analysis. Prev Sci. 2001;2:123–34.54. Freisthler B, Midanik L and Gruenewald P. <strong>Alcohol</strong> outletsand child physical abuse and neglect: apply<strong>in</strong>g rout<strong>in</strong>eactivities theory to the study <strong>of</strong> child maltreatment. JStud <strong>Alcohol</strong>. 2004; 65:586–92.55. Wechsler H, Lee J, Hall J, Wagenaar A and Lee H.Secondhand effects <strong>of</strong> student alcohol use reported byneighbors <strong>of</strong> colleges: the role <strong>of</strong> alcohol outlets. Soc SciMed. 2002; 55:425–35.56. Stockwell T, Masters L, Philips M, Daly A, Gahegan M,Midford R, et al. Consumption <strong>of</strong> different alcoholicbeverages as predictors <strong>of</strong> local rates <strong>of</strong> night-timeassault and acute alcohol-<strong>related</strong> morbidity. <strong>Australia</strong>and New Zealand Journal <strong>of</strong> Public <strong>Health</strong>. 1998;22:237–42.57. Drugs and Crime Prevention Committee (DCPC).Inquiry <strong>in</strong>to strategies to reduce harmful consumption<strong>of</strong> alcohol – discussion paper. Melbourne: Parliament <strong>of</strong>Victoria, 2006.58. Parliament <strong>of</strong> Victoria. Drugs and Crime PreventionCommittee (DCPC) Inquiry <strong>in</strong>to Strategies to Reduce<strong>Harm</strong>ful <strong>Alcohol</strong> Consumption – F<strong>in</strong>al Report.Melbourne, 2006.59. Kypri K. The health impacts and politics <strong>of</strong> changes<strong>in</strong> the m<strong>in</strong>imum purchase age for alcohol <strong>in</strong> NewZealand. Perth: National Drug Research Institute,Curt<strong>in</strong> University, 2006.60. Ward B and Snow P. The role <strong>of</strong> families <strong>in</strong> prevent<strong>in</strong>galcohol-<strong>related</strong> harm among young people. PreventionResearch Quarterly. West Melbourne: DrugInfoClear<strong>in</strong>ghouse, 2008.61. White V and Hayman J. Smok<strong>in</strong>g behaviours <strong>of</strong><strong>Australia</strong>n secondary students <strong>in</strong> 2005. Canberra: DrugStrategy Branch, <strong>Australia</strong>n Government <strong>Department</strong><strong>of</strong> <strong>Health</strong> and Age<strong>in</strong>g, 2006. Available from: www.nationaldrugstrategy.gov.au/<strong>in</strong>ternet/drugstrategy/publish<strong>in</strong>g.nsf/Content/mono5962. World <strong>Health</strong> Organization. Global strategy on diet,physical activity and health. Fifty-Seventh World <strong>Health</strong>Assembly. World <strong>Health</strong> Organization, 2004. Availablefrom: www.who.<strong>in</strong>t/dietphysicalactivity/goals/en/<strong>in</strong>dex.html47
63. Gruenewald P, Freisthler B and Remer L. EcologicalModels <strong>of</strong> <strong>Alcohol</strong> Outlets and Violent Assaults: CrimePotentials and Geospatial Analysis, <strong>Alcohol</strong> Taxation <strong>in</strong>the Western Pacific Region. WHO Collaborat<strong>in</strong>g Centrefor Research and Tra<strong>in</strong><strong>in</strong>g <strong>in</strong> <strong>Alcohol</strong> and Drug AbuseWorld <strong>Health</strong> Organization, 2006.64. Chaloupka FJ, Hyland A, Laux FL, Higbee C, Hast<strong>in</strong>gsG, Ross H, et al. Cigarette purchase patterns <strong>in</strong> fourcountries and the relationship with cessation: f<strong>in</strong>d<strong>in</strong>gsfrom the International Tobacco Control (ITC) FourCountry Survey. Tobacco Control. 2006; 15:iii59−64.Available from: http://tc.bmjjournals.com/cgi/content/abstract/15/suppl_3/iii5965. Kenkel DS and Mann<strong>in</strong>g WG. Perspectives on alcoholtaxation. <strong>Alcohol</strong> <strong>Health</strong> & Research World. 1996;20:230−8.66. Osterberg E. Do alcohol prices affect consumptionand <strong>related</strong> problems? <strong>Alcohol</strong> Taxation <strong>in</strong> the WesternPacific Region. World <strong>Health</strong> Organization, 2006.67. Econtech Pty Ltd. Modell<strong>in</strong>g health-<strong>related</strong> reforms totaxation <strong>of</strong> alcoholic beverages. 2004.68. Distilled Spirits Industry Council <strong>of</strong> <strong>Australia</strong>Incorporated (DSICA). Pre-budget submissions2008–09. Distilled Spirits Industry Council <strong>of</strong> <strong>Australia</strong>Incorporated, 2008.69. Doran C, M., , Gascoigne MB, Shakeshaft AP andPetrie D. The consumption <strong>of</strong> alcohol by <strong>Australia</strong>nadolescents: A comparison <strong>of</strong> revenue andexpenditure. Addictive Behaviours. 2006; 31:1919–28.70. Stockwell T and Crosbie D. Supply and demandfor alcohol <strong>in</strong> <strong>Australia</strong>: relationships between<strong>in</strong>dustry structures, regulation and the marketplace.International Journal <strong>of</strong> Drug Policy. 2001;12:139–52. Available from: www.ncbi.nlm.nih.gov/pubmed/1139941771. Gray D, Saggers S, Sputor B and Bourbon D. What works?A review <strong>of</strong> evaluated alcohol misuse <strong>in</strong>terventionsamong Aborig<strong>in</strong>al <strong>Australia</strong>ns. Addiction. 2000;95:11−22. Available from: www3.<strong>in</strong>terscience.wiley.com/journal/120190664/abstract?CRETRY=1&SRETRY=072. Stockwell T. Work<strong>in</strong>g with the alcohol <strong>in</strong>dustry onalcohol policy: should we sometimes sit at the sametable. Addiction. 2007; 102:1−3. Available from: www3.<strong>in</strong>terscience.wiley.com/journal/117967514/abstract73. Chikritzhs T, Loxley W, Gray D, Wilk<strong>in</strong>son C, Midford Rand Moore D. <strong>Alcohol</strong> policy and harm reduction <strong>in</strong><strong>Australia</strong>. Drug and <strong>Alcohol</strong> Review. 2005; 24:559−68.Available from: www.<strong>in</strong>formaworld.com/smpp/content~db=all?content=10.1080/0959523050040413774. Distilled Spirits Industry Council <strong>of</strong> <strong>Australia</strong> Incorporated(DSICA). <strong>Alcohol</strong> tax <strong>in</strong> <strong>Australia</strong>. Distilled Spirits IndustryCouncil <strong>of</strong> <strong>Australia</strong> Incorporated, 2006.75. Havard A, Shakeshaft A and Sanson-Fisher R. Systematicreview and meta-analyses <strong>of</strong> strategies target<strong>in</strong>galcohol problems <strong>in</strong> emergency departments:<strong>in</strong>terventions reduce alcohol-<strong>related</strong> <strong>in</strong>juries. Addiction.2008; 103:368–76. Available from: www3.<strong>in</strong>terscience.wiley.com/journal/119411900/abstract76. Roche AM, Pidd K, Berry JG and Harrison JE. Workers’dr<strong>in</strong>k<strong>in</strong>g patterns: the impact on absenteeism <strong>in</strong> the<strong>Australia</strong>n work-place. Addiction. 2008; 103:738–48.Available from: www.<strong>in</strong>gentaconnect.com/content/bsc/add/2008/00000103/00000005/art0001377. LaMontagne AD, Ostry A and Shaw A. Workplace stress<strong>in</strong> Victoria: develop<strong>in</strong>g a systems approach. Victorian<strong>Health</strong> Promotion Foundation, 2006.78. Harper CG, Sheedy DL, Lara AI, Garrick TM, Hilton JMand Raisanen J. Prevalence <strong>of</strong> Wernicke--Korsak<strong>of</strong>fsyndrome <strong>in</strong> <strong>Australia</strong>: has thiam<strong>in</strong>e fortification madea difference? The Medical Journal <strong>of</strong> <strong>Australia</strong>. 1998;168:542–5. Available from: www.mja.com.au/public/issues/jun1/harper/harper.html79. Gray D, Pulver LJ, Saggers S and Waldon J. Address<strong>in</strong>g<strong>in</strong>digenous substance misuse and <strong>related</strong> harms. Drugand <strong>Alcohol</strong> Review. 2006; 25:183−8. Available from:www.<strong>in</strong>formaworld.com/smpp/content~db=all?content=10.1080/0959523060064461680. Brady M, Nicholls R, Henderson G and Byrne J. The role<strong>of</strong> a rural sober<strong>in</strong>g-up centre <strong>in</strong> manag<strong>in</strong>g alcohol<strong>related</strong>harm to Aborig<strong>in</strong>al people <strong>in</strong> South <strong>Australia</strong>.Drug and <strong>Alcohol</strong> Review. 2006; 25:201–6.81. Mosher J, Toomey T, Harwood E and Wagenaar A.State laws mandat<strong>in</strong>g or promot<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g programsfor alcohol servers and establishment managers: Anassessment <strong>of</strong> statutory and adm<strong>in</strong>istrative proceduresJournal <strong>of</strong> Public <strong>Health</strong> Policy. 2002; 23:90–113.82. Mosher J and Jernigan D. New directions <strong>in</strong> alcoholpolicy. Annual Review <strong>of</strong> Public <strong>Health</strong>. 1989; 10:245−79.83. Wiggers J, Joauncey M, Consid<strong>in</strong>e R, Daly J, K<strong>in</strong>gslandM, Purss K, et al. Strategies and outcomes <strong>in</strong> translat<strong>in</strong>galcohol harm reduction research <strong>in</strong>to practice: the<strong>Alcohol</strong> L<strong>in</strong>k<strong>in</strong>g Program. Drug and <strong>Alcohol</strong> Review.2004; 23:355−64. Available from: www.<strong>in</strong>formaworld.com/smpp/content~db=all?content=10.1080/0959523041233128951884. Jones S and Donovan R. Messages <strong>in</strong> alcoholadvertis<strong>in</strong>g targeted to youth. <strong>Australia</strong>n & New ZealandJournal <strong>of</strong> Public <strong>Health</strong>. 2001; 25:126–31.85. <strong>Alcohol</strong> Beverages Advertis<strong>in</strong>g Code. Annual report2006–07. <strong>Alcohol</strong> Beverages Advertis<strong>in</strong>g Code,2008. Available from: www.abac.org.au/files/ABAC2006AnnualReport.pdf48
86. K<strong>in</strong>g E, Taylor J and Carroll T. <strong>Australia</strong>n alcoholbeverage advertis<strong>in</strong>g <strong>in</strong> ma<strong>in</strong>stream <strong>Australia</strong>n media2003 to 2005: expenditure, exposure and <strong>related</strong> issues.Research and Market<strong>in</strong>g Group, <strong>Department</strong> <strong>of</strong> <strong>Health</strong>and Age<strong>in</strong>g, 2005. Available from: www.alcohol.gov.au/<strong>in</strong>ternet/alcohol/publish<strong>in</strong>g.nsf/content/BD9ED91EDC948718CA2571E30023FAD3/$File/aust-ma<strong>in</strong>stream.pdf87. K<strong>in</strong>g E, Taylor J and Carroll T. Consumer perceptions <strong>of</strong>alcohol advertis<strong>in</strong>g and the revised <strong>Alcohol</strong> BeveragesAdvertis<strong>in</strong>g Code. Research and Market<strong>in</strong>g Group,<strong>Department</strong> <strong>of</strong> <strong>Health</strong> and Age<strong>in</strong>g, 2005b. Availablefrom: www.alcohol.gov.au/<strong>in</strong>ternet/alcohol/publish<strong>in</strong>g.nsf/Content/consum-percept88. Senate. Inquiry <strong>in</strong>to <strong>Alcohol</strong> Toll Reduction Bill 2007.Senate Community Affairs Committee, Parliament <strong>of</strong><strong>Australia</strong>, 2008a. Available from: www.aph.gov.au/senate/committee/clac_ctte/alcohol_reduction/<strong>in</strong>dex.htm89. Woolcott Research. Formative research for thedevelopment <strong>of</strong> a national alcohol social market<strong>in</strong>g<strong>in</strong>itiative. <strong>Australia</strong>n Government <strong>Department</strong> <strong>of</strong> <strong>Health</strong>and Age<strong>in</strong>g, 2007. Available from: www.alcohol.gov.au/<strong>in</strong>ternet/alcohol/publish<strong>in</strong>g.nsf/Content/7C6B70D6091A3E4ACA25739A0082EFA5/$File/aaa-woolcott-rep.pdf90. Bond L, Patton G, Glover S, Carl<strong>in</strong> JB, Butler H, Thomas L,et al. The Gatehouse Project: can a multi-level school<strong>in</strong>tervention affect emotional wellbe<strong>in</strong>g and health riskbehaviours? Journal <strong>of</strong> Epidemiology and Community<strong>Health</strong>. 2004; 58:997–1003. Available from: http://jech.bmj.com/cgi/content/full/58/12/99795. M<strong>in</strong>isterial Council on Drug Strategy. National healthpolicy on alcohol <strong>in</strong> <strong>Australia</strong>, Canberra: M<strong>in</strong>isterialCouncil on Drug Strategy, 1989.96. <strong>Department</strong> <strong>of</strong> <strong>Health</strong> and Family Services (DHFS).National <strong>Alcohol</strong> Action Plan 1995–1997. Canberra:Commonwealth <strong>Department</strong> <strong>of</strong> <strong>Health</strong> and FamilyServices, 1996.97. M<strong>in</strong>isterial Council on Drug Strategy. National alcoholstrategy: a plan for action 2001 to 2003/04, Canberra:Commonwealth <strong>Department</strong> <strong>of</strong> <strong>Health</strong> and AgedCare, 2001.98. Midford R. <strong>Australia</strong> and alcohol: liv<strong>in</strong>g down the legend.Addiction. 2005; 100:891–6. Available from: www3.<strong>in</strong>terscience.wiley.com/journal/118739423/abstract99. Chisholm D, Doran C, Shibuya K and Rehm J.Comparative cost-effectiveness <strong>of</strong> policy <strong>in</strong>strumentsfor reduc<strong>in</strong>g the global burden <strong>of</strong> alcohol, tobaccoand illicit drug use. Drug and <strong>Alcohol</strong> Review. 2006;25:553–65. Available from: www.<strong>in</strong>formaworld.com/smpp/content~content=a762363140~db=all~tab=content~order=page100. Coll<strong>in</strong>s D and Lapsley H. The avoidable costs <strong>of</strong> alcoholabuse <strong>in</strong> <strong>Australia</strong> and the potential benefits <strong>of</strong> effectivepolicies to reduce the social costs <strong>of</strong> alcohol. Canberra:<strong>Department</strong> <strong>of</strong> <strong>Health</strong> and Age<strong>in</strong>g, 2008. Availablefrom: www.nationaldrugstrategy.gov.au/<strong>in</strong>ternet/drugstrategy/publish<strong>in</strong>g.nsf/Content/mono7091. National <strong>Health</strong> and Medical Research Council.<strong>Australia</strong>n alcohol guidel<strong>in</strong>es: health risk and benefits.Canberra: National <strong>Health</strong> and Medical ResearchCouncil, 2001. Available from: www.nhmrc.gov.au/publications/synopses/_files/ds9.pdf92. Wilk<strong>in</strong>son C and Room R. Informational and warn<strong>in</strong>glabels on alcohol conta<strong>in</strong>ers, sales places andadvertisements: experience <strong>in</strong>ternationally andevidence on effects (Report submitted to the Victorian<strong>Department</strong> <strong>of</strong> Human Services, 15 January 2008).AER Centre for <strong>Alcohol</strong> Policy Research, Turn<strong>in</strong>g Po<strong>in</strong>t<strong>Alcohol</strong> and Drug Centre, 2007.93. Brand DA, Saisana M, Rynn LA, Pennoni F andLowenfels AB. Comparative analysis <strong>of</strong> alcohol controlpolicies <strong>in</strong> 30 countries. PLoS Medic<strong>in</strong>e. 2007; 4:e151.Available from: http://medic<strong>in</strong>e.plosjournals.org/perlserv/?request=get-document&doi=10.1371/journal.pmed.004015194. Babor TF and W<strong>in</strong>stanley EL. The world <strong>of</strong> dr<strong>in</strong>k<strong>in</strong>g:national alcohol control experiences <strong>in</strong> 18 countries.Addiction. 2008; 103:721–5. Available from: www3.<strong>in</strong>terscience.wiley.com/journal/119411977/abstract49